Chronic Kidney Disease - Free MCQ Practice Test with solutions, NEET PG
MCQ Practice Test & Solutions: Test: Chronic Kidney Disease (30 Questions)
You can prepare effectively for NEET PG Topic Wise MCQs for NEET PG with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Chronic Kidney Disease". These 30 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 30 minutes
- - Number of Questions: 30
Sign up on EduRev for free to attempt this test and track your preparation progress.

Which of the following drug does not cause nephrotoxicity? (Recent Question 2016-17)
Detailed Solution: Question 1
A 50 year-old diabetic patient is feeling unwell. On work up his serum creatinine = 5.0 mg% and blood urea = 125 mg%. Urine MICRAL test is positive. Which of the following will be useful for this patient? (Recent Question 2016-17)
Detailed Solution: Question 2

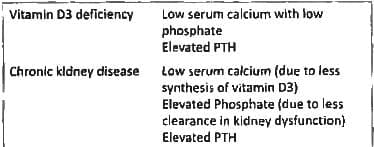
Which of the following conditions typically has rickets with normal or low calcium, elevated phosphorus, elevated parathormone, and elevated alkaline phosphatase? (APPG 2016)
Detailed Solution: Question 3
The triad of 'saturnine gout' + hypertension + renal failure is seen in? (APPG 2016)
Detailed Solution: Question 4
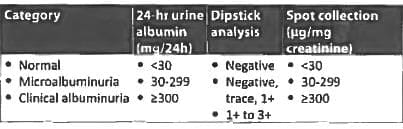
Which of the following statement on microalbuminuria is not true? (AIIMS Nov 2015)
Detailed Solution: Question 5
All of the following may result in polyuria except: (UPSC 2015)
Detailed Solution: Question 6

Regarding adult polycystic kidney disease, which one of the following statements is not correct? (UPSC 2015)
Detailed Solution: Question 7

Which of the following is not a feature of chronic renal failure? (UPSC 2015)
Detailed Solution: Question 8

Patient on insulin in CKD stage 4. What is the dose adjustment of insulin required? (Recent Question 2015-16)
Detailed Solution: Question 9
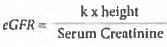
All are true about GFR except? (Recent Question 2015-16)
Detailed Solution: Question 10
Patient with CRF is having a sodium level = 110 mEq/dl. Till what level should serum sodium be corrected in next 24 hours? (Recent Pattern 2014-15)
Detailed Solution: Question 11
Detailed Solution: Question 12
Diagnostic feature of CRF is: (Recent Pattern 2014-15)
Detailed Solution: Question 13
Which one of the following studies is most sensitive for detecting diabetic nephropathy in early stage? (Recent Pattern 2014-15)
Detailed Solution: Question 14
Detailed Solution: Question 15
Clinical features of CRF/uraemia appear when renal function is reduced to: (Recent Pattern 2014-15)
Detailed Solution: Question 16
Detailed Solution: Question 17
Detailed Solution: Question 18
A 28 yr old man has lenticonus and ESRD. His maternal uncle also died of similar illness. Diagnosis is: (AIIMS May 2012)
Detailed Solution: Question 19
Central nervous system manifestations in chronic renal failure are a result of all of the following except: (Recent Pattern 2014-15)
Detailed Solution: Question 20
Dialysis disequilibrium occurs due to: (Recent Pattern 2014-15)
Detailed Solution: Question 21
Normal sized to enlarged kidneys in a patient with chronic renal failure is indicative of: (Recent Pattern 2014-15)
Detailed Solution: Question 22
Metabolic complication in CRF include all of the following except : (AI 1998)
Detailed Solution: Question 23
Chronic renal failure is often complicated by all of the following except: (Recent Pattern 2014-15)
Detailed Solution: Question 24
Dementia in patient of chronic renal failure with chronic hemodialysis is due to: (Recent Pattern 2014-15)
Detailed Solution: Question 25
Convulsions are commonly precipitated in terminal renal failure by: (Recent Pattern 2014-15)
Detailed Solution: Question 26
Anaemia of advanced renal insufficiency is best treated by: (Recent Pattern 2014-15)
Detailed Solution: Question 27
In chronic renal failure there is: (Recent Pattern 2014-15)
Detailed Solution: Question 28
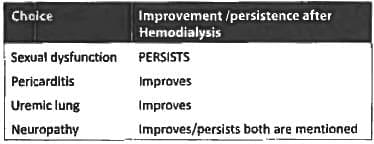
In uraemia all are reversed by dialysis except: (Recent Pattern 2014-15)
Detailed Solution: Question 29
Detailed Solution: Question 30