NEET Exam > NEET Notes > Biology Class 12 > Revision Notes: Human Reproduction
Revision Notes: Human Reproduction


Reproduction
Reproduction in humans comprises formation of male and female gametes, transfer of the male gamete into the female reproductive tract, fusion of gametes (fertilisation), implantation of the fertilised egg and subsequent embryo and fetal development leading to parturition and post-natal care (lactation). This chapter presents concise, syllabus-aligned revision notes covering structure, function, hormonal control, key events from gametogenesis to birth, and important applied topics such as assisted reproductive techniques and common contraceptive methods.
Male Reproductive System
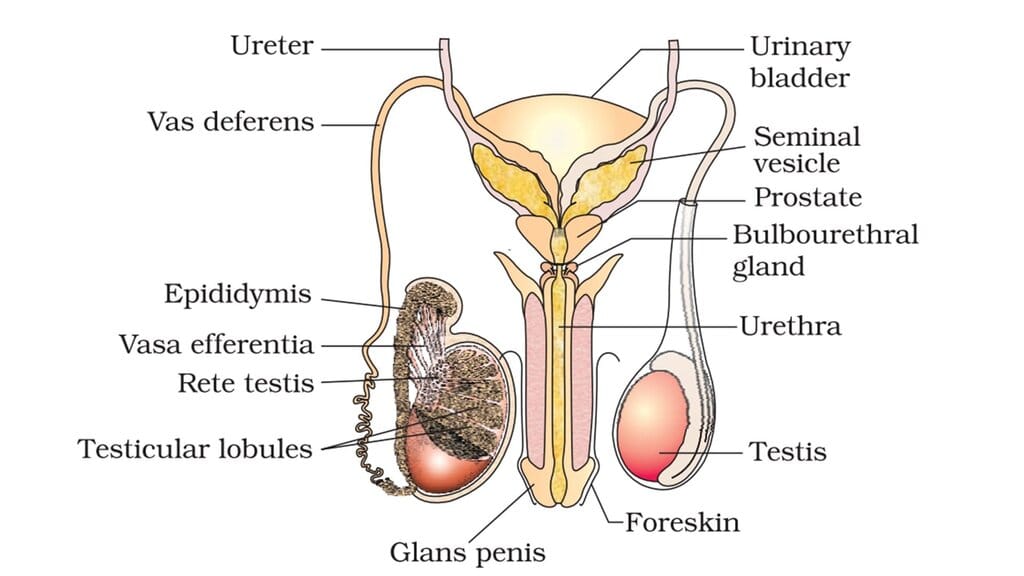
- Testes: Paired gonads located in the scrotum, held 2-2.5°C cooler than core body temperature for optimal spermatogenesis. Each testis has about 200-300 lobules; each lobule contains one to three highly coiled seminiferous tubules where spermatogenesis occurs.
- Spermatogenic cells and supporting cells: Seminiferous tubules contain germ cells at various stages (spermatogonia, primary and secondary spermatocytes, spermatids) and non-germinal Sertoli cells that nourish and support developing germ cells. Leydig cells (interstitial cells) in the spaces between tubules synthesise androgens (notably testosterone).
- Accessory ducts: Spermatozoa released from seminiferous tubules pass into the rete testis, through vasa efferentia to the epididymis where they mature and are stored; mature sperm travel via the vas deferens which joins the duct of the seminal vesicle to form the ejaculatory duct and then the urethra.
- Accessory glands: The seminal vesicles, prostate gland and bulbourethral glands produce seminal plasma - a nutritive and buffering fluid containing fructose, enzymes, calcium and other substances that aid sperm viability, motility and transport.
- External genitalia: The penis (erectile organ) facilitates insemination. The glans penis is covered by the foreskin (prepuce) unless removed by circumcision.
Structure of a Sperm
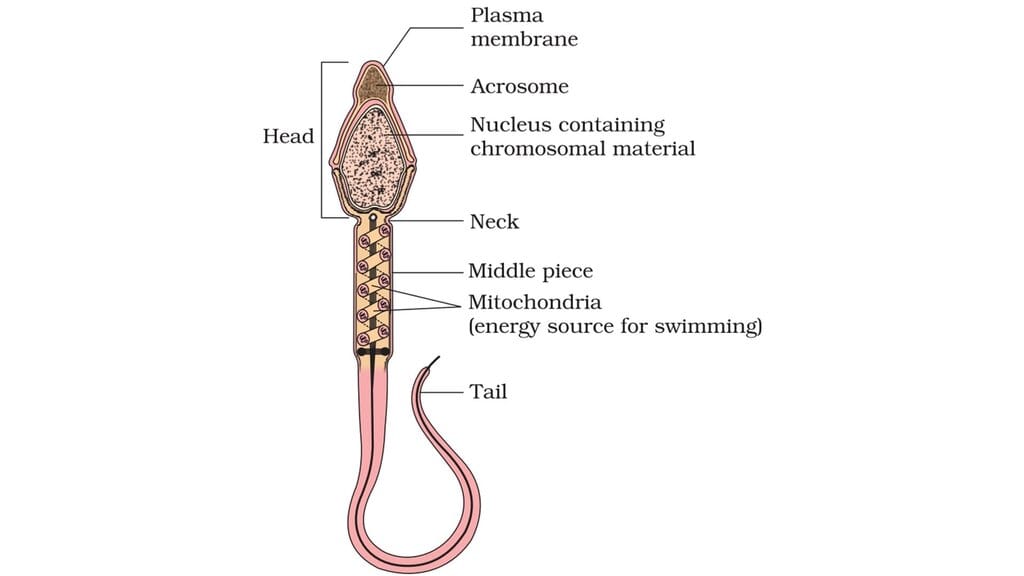
- A mature spermatozoon has a head (haploid nucleus) covered anteriorly by the acrosome which contains enzymes for zona pellucida penetration, a middle piece packed with mitochondria that supply ATP for motility, and a long tail (flagellum) for propulsion; the whole cell is bounded by a plasma membrane.
- Normal ejaculate volume and quality: a typical ejaculate contains about 200-300 million sperm. Fertility assessments often consider percentage of morphologically normal sperm (generally ≥60% considered adequate) and percentage of progressively motile sperm (≥40% vigorous motility considered desirable).
- Semen is spermatozoa suspended in seminal plasma derived from accessory glands; testicular hormones and accessory gland secretions regulate sperm function.
Gametogenesis (Males) - Spermatogenesis
- Overview: Spermatogenesis is the process by which diploid spermatogonia divide and differentiate into haploid spermatozoa. It occurs within seminiferous tubules and continues from puberty throughout adult life.
- Sequence: Spermatogonia (2n) divide by mitosis to maintain the stem cell pool and produce cells that differentiate into primary spermatocytes (2n). Primary spermatocytes undergo meiosis I to yield two secondary spermatocytes (n). Secondary spermatocytes undergo meiosis II to produce four haploid spermatids. Spermatids undergo morphological transformation (spermiogenesis) into spermatozoa and are released by spermiation.
- Duration: The entire process takes several weeks (approximately 60-70 days in humans) with continuous production thereafter.
- Hormonal control: The hypothalamus secretes GnRH (gonadotropin-releasing hormone) in a pulsatile manner, stimulating the anterior pituitary to release LH and FSH. LH acts on Leydig cells to stimulate androgen (testosterone) production. FSH acts on Sertoli cells to support spermatogenesis and stimulate production of inhibin, which provides negative feedback on FSH secretion. Testosterone also exerts negative feedback on LH and GnRH.
- Capacitation and acrosome reaction: After ejaculation, sperm undergo capacitation (physiological changes in the female reproductive tract rendering them capable of fertilising an ovum). When a capacitated sperm contacts the zona pellucida, the acrosome reaction releases hydrolytic enzymes allowing penetration of the zona.
Female Reproductive System
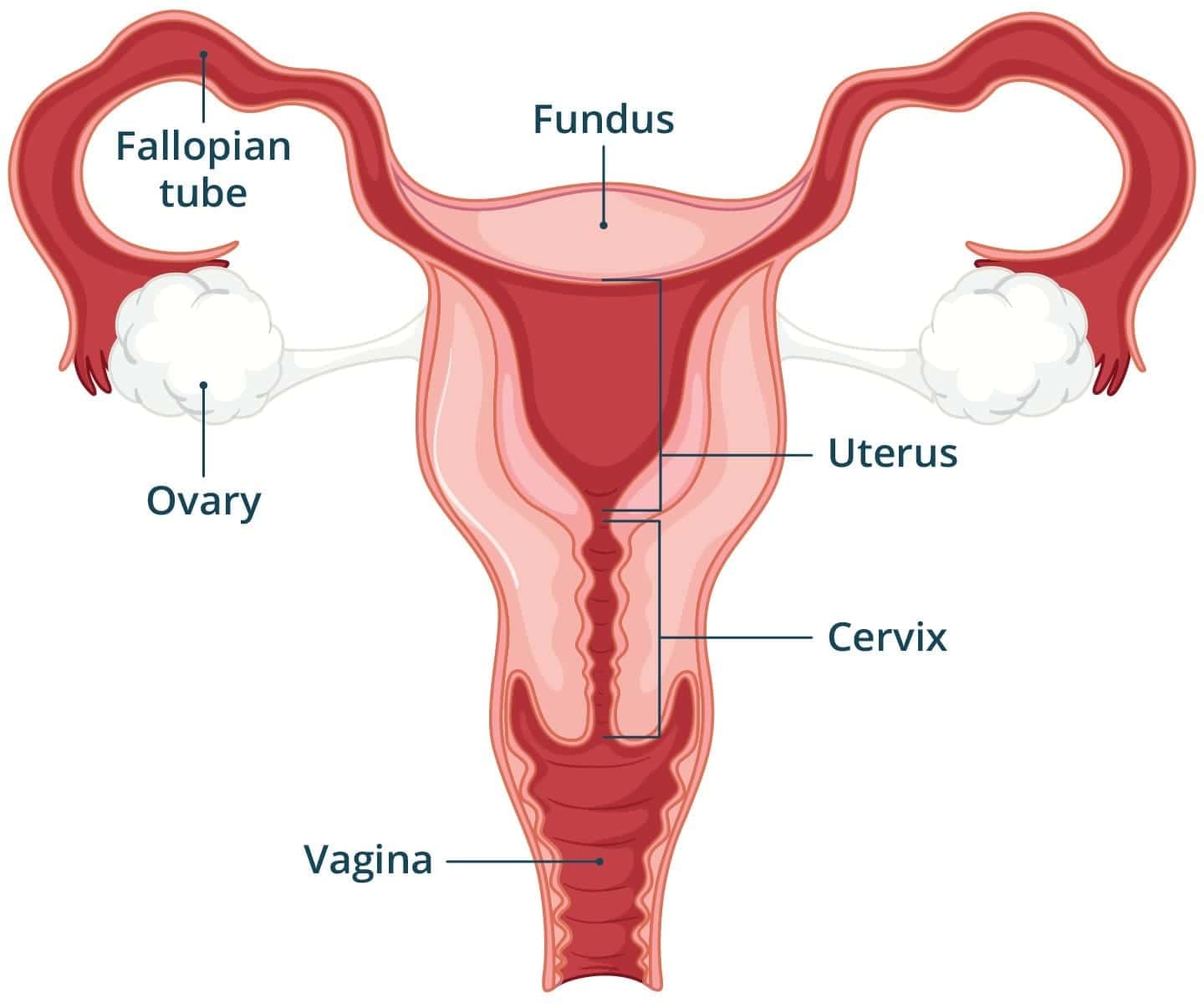
- The system includes paired ovaries, paired oviducts (fallopian tubes), the uterus, cervix, vagina, external genitalia and paired mammary glands.
- Main functions are oogenesis (formation of ova), ovulation, fertilisation, embryo implantation and pregnancy, childbirth and newborn care via lactation.
Ovary and Oviduct
- Ovaries: Each ovary has a surface germinal epithelium, a cortical region containing ovarian follicles at various stages and a central medulla with blood vessels and connective tissue. Follicles progress through stages: primordial → primary → secondary → tertiary (antral) → mature or Graafian follicle.
- Oviduct (fallopian tube): Approximately 10-12 cm long, with three parts: infundibulum bearing fimbriae which capture the ovulated oocyte, ampulla (usual site of fertilisation), and isthmus which joins the uterus. Ciliated epithelium and peristaltic contractions transport the oocyte/zygote towards the uterus.
Uterus and External Genitalia
- Uterus: A hollow, muscular organ (womb), roughly pear-shaped and supported by pelvic ligaments. The narrow lower region is the cervix that opens into the vagina. The uterine wall comprises three layers: outer serous perimetrium, thick muscular myometrium (powerful contractions at parturition), and inner glandular endometrium which undergoes cyclical changes to prepare for implantation.
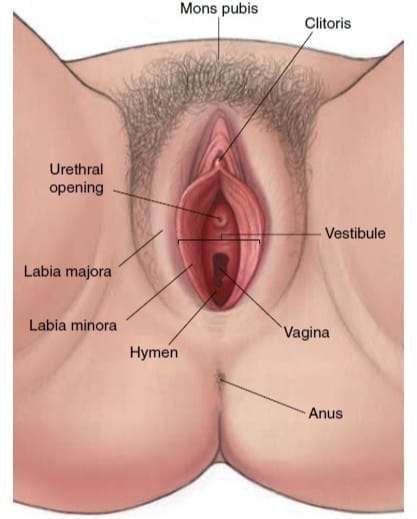
- External genitalia: Includes the mons pubis, labia majora, labia minora, clitoris and the hymen (a mucosal fold that may partially cover the vaginal opening).
Mammary Glands
- Paired mammary glands in the female breast contain 15-20 lobes each. Lobes subdivide into lobules with milk-secreting alveoli. Milk drains from alveoli into mammary tubules, then into the mammary ampulla and exits via the lactiferous ducts at the nipple. Mammary glands differentiate during puberty and further under the influence of pregnancy hormones.
Gametogenesis (Females) - Oogenesis
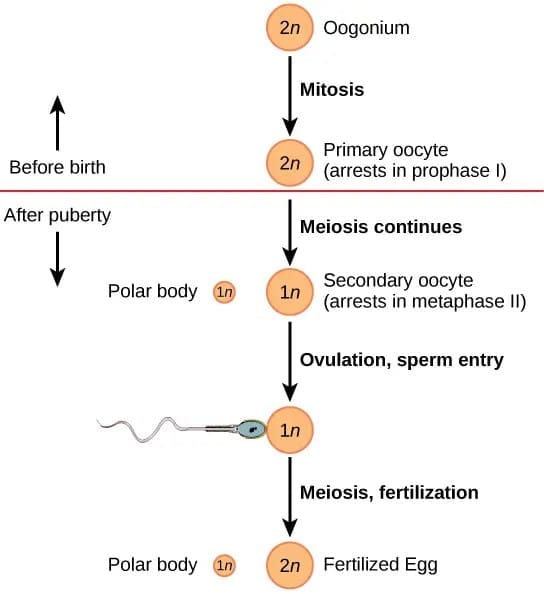
- Origin and arrest: Oogenesis begins during fetal development. Diploid oogonia divide mitotically and differentiate into primary oocytes which enter meiosis I and arrest at prophase I; these are stored within primordial follicles.
- Follicular development: At puberty, under hormonal influence, cohorts of follicles resume development. Many follicles atresia (degenerate), while selected follicles mature from primary → secondary → tertiary (antral) → Graafian follicles.
- Meiotic divisions: Just before ovulation, the primary oocyte completes meiosis I to form a large haploid secondary oocyte and a small first polar body. The secondary oocyte initiates meiosis II but arrests at metaphase II and is ovulated. Meiosis II completes only if a sperm penetrates, producing a fertilised ovum and a second polar body.
- Ovulation: The release of the secondary oocyte from the Graafian follicle; usually occurs around day 14 in a typical 28-day cycle.
Menstrual Cycle and Hormonal Regulation
- Menarche is the first menstrual bleed. Typical cycle length is about 28 days, though 21-35 days is common.
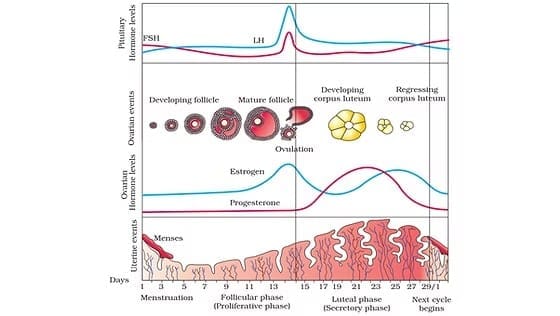
- Phases of the cycle (approximate timings in a 28-day cycle): menstrual phase (days 1-5) - shedding of the functional layer of endometrium if fertilisation has not occurred; follicular (proliferative) phase (days 6-13) - follicle growth and endometrial repair under rising FSH and increasing estrogen; ovulatory phase (~day 14) - a midcycle LH surge triggers rupture of the Graafian follicle and ovulation; luteal (secretory) phase (days 15-28) - the ruptured follicle forms the corpus luteum which secretes progesterone (and estrogen) to prepare and maintain the endometrium for potential implantation.
- Hormonal interactions: GnRH (hypothalamus) → stimulates anterior pituitary to release FSH and LH. FSH promotes follicular growth and estrogen secretion from granulosa cells. Rising estrogen exerts a positive feedback on the pituitary and hypothalamus just before ovulation causing the LH surge. After ovulation, progesterone and estrogen from the corpus luteum exert negative feedback on FSH and LH. If fertilisation does not occur, the corpus luteum degenerates (corpus albicans), progesterone falls and menstruation begins. If implantation occurs, trophoblast cells produce hCG which maintains the corpus luteum and its progesterone secretion.
- Menopause: The permanent cessation of menstruation, typically around age ≈50 years, due to depletion of functional follicles and reduced estrogen production.
Fertilisation
- During coitus, semen is deposited in the vagina. Motile sperm undergo capacitation in the female tract, then migrate through the cervix and uterus to the ampullary region of the fallopian tube where the ovum is usually present.
- Sperm-egg recognition and entry: Sperm binds to the zona pellucida surrounding the oocyte, triggering the acrosome reaction. Enzymes released from the acrosome digest a path through the zona enabling a sperm to reach the oocyte membrane. Fusion of membranes allows the sperm nucleus to enter the oocyte.
- Completion of meiosis and formation of zygote: On penetration, the secondary oocyte completes meiosis II to produce the ovum and a second polar body. The haploid nuclei of sperm and ovum fuse to form a diploid zygote.
- Sex determination: The ovum always contributes an X chromosome; the sperm contributes either X or Y. A zygote with XX becomes genetically female; XY becomes genetically male. Thus the male gamete determines chromosomal sex.
Cleavage and Early Embryo
- After fertilisation the zygote undergoes a series of rapid mitotic divisions called cleavage producing 2, 4, 8, 16... cells called blastomeres. The 8-16 cell compacted mass is called the morula.
- The morula develops a fluid-filled cavity and forms the blastocyst composed of an outer cell layer - the trophoblast (which will contribute to the placenta) - and an inner cell mass (which will form the embryo proper).
- Implantation occurs when the blastocyst attaches to and then embeds into the endometrium (usually about 6-7 days after fertilisation). Trophoblastic cells invade the endometrium and contribute to formation of the placenta.
Placenta and Pregnancy
- The placenta develops from the trophoblast (chorion) and maternal uterine tissue. Chorionic villi are finger-like projections that increase surface area for exchange and form the functional interface between maternal and fetal circulations.
- Functions of the placenta: transfer of oxygen and nutrients from maternal blood to the fetus; removal of fetal metabolic wastes (e.g., CO₂) to maternal blood; endocrine functions by producing hormones essential for maintenance of pregnancy and fetal development; protection - physical barrier (though not absolute) and selective transport of antibodies.
- Key placental hormones and maternal changes: The placenta secretes human chorionic gonadotropin (hCG) which maintains the corpus luteum in early pregnancy; human placental lactogen (hPL) (also called human chorionic somatomammotropin) which modulates maternal metabolism to favour fetal nutrition; and placental estrogens and progestogens which support endometrium and mammary development. Maternal blood levels of cortisol, prolactin and thyroxine are typically elevated during pregnancy.
- Umbilical cord connects fetus and placenta and contains two umbilical arteries (carry deoxygenated blood from fetus to placenta) and one umbilical vein (carry oxygenated blood from placenta to fetus), embedded in Wharton's jelly.
- Pregnancy detection: Presence of hCG in maternal blood or urine is the basis of pregnancy tests.
Early Embryonic Differentiation and Timeline
- The inner cell mass of the blastocyst gives rise to the embryo and differentiates into the three primary germ layers during gastrulation: ectoderm (gives rise to skin and nervous system), mesoderm (muscles, skeleton, cardiovascular system and urogenital structures), and endoderm (lining of gut and associated organs). The inner cell mass contains pluripotent stem cells.
- Typical developmental milestones (approximate): 1 month - early heart formation and beginning of organogenesis; 2 months - limb buds elongate and digits begin to form; end of first trimester (≈12 weeks) - major organ systems established; 5 months - fetal movement felt (quickening), hair and skin features appear; 24 weeks - finer details such as eyelashes and eyelid separation, viability outside uterus increases though intensive care required; 9 months - fetal growth completes and the fetus is ready for delivery.
- Types of twins: Dizygotic (fraternal) twins arise from two separate ova fertilised by two sperm (two zygotes); they are genetically like ordinary siblings. Monozygotic (identical) twins arise from the splitting of a single zygote - the timing of splitting determines whether they share the same chorion or amnion.
Parturition and Lactation
- Parturition (childbirth): Initiation involves fetal signals, placental hormones and maternal responses. Increased fetal cortisol and placental factors influence uterine contractility. Stretching of the cervix and uterus activates a neuroendocrine reflex causing release of maternal oxytocin from the posterior pituitary. Oxytocin stimulates uterine contractions and prostaglandin release; a positive feedback loop intensifies contractions until the baby and then the placenta are expelled.
- Stages of labour: the first stage is dilation of the cervix, the second stage is expulsion of the baby, and the third stage is expulsion of the placenta (afterbirth).
- Lactation: Mammary glands undergo further differentiation during pregnancy. Prolactin (anterior pituitary) stimulates milk synthesis, while oxytocin causes milk ejection (let-down reflex) by contracting myoepithelial cells around alveoli. Colostrum, the first milk, is rich in proteins (including secretory IgA), antibodies and minerals, and provides early immune protection to the newborn. Establishment of breastfeeding soon after birth supports neonatal immunity and nutrition.
The document Revision Notes: Human Reproduction is a part of the NEET Course Biology Class 12.
All you need of NEET at this link: NEET
FAQs on Revision Notes: Human Reproduction
| 1. What is the process of fertilization in human reproduction? |  |
Ans. Fertilization is the process in human reproduction where the sperm and egg cells unite to form a zygote. It occurs in the fallopian tubes when the sperm penetrates the egg, leading to the fusion of their genetic material. This fusion forms a zygote, which then undergoes cell division and development to form an embryo.
| 2. What are the phases of embryonic development? | |
Ans. The phases of embryonic development are: 1. Cleavage: After fertilization, the zygote undergoes rapid cell division, called cleavage. During this phase, the number of cells increases, but the overall size remains the same. 2. Blastulation: Cleavage leads to the formation of a blastocyst, which is a hollow ball of cells. The blastocyst consists of an outer layer called the trophoblast and an inner cell mass. 3. Implantation: The blastocyst implants itself into the uterine lining during this phase. The trophoblast cells release enzymes that help in the penetration and attachment of the blastocyst to the uterus. 4. Gastrulation: The inner cell mass of the blastocyst differentiates into three germ layers: ectoderm, mesoderm, and endoderm. This process is known as gastrulation. 5. Organogenesis: During organogenesis, the three germ layers further differentiate and form the various organs and tissues of the developing embryo.
| 3. What is the menstrual cycle and its importance in human reproduction? | |
Ans. The menstrual cycle is a monthly physiological process that occurs in females of reproductive age. It involves the shedding of the uterine lining and prepares the body for potential pregnancy. The menstrual cycle is controlled by hormonal changes and consists of three main phases: the follicular phase, ovulation, and the luteal phase. The menstrual cycle is important in human reproduction as it regulates the release of eggs from the ovaries and prepares the uterus for the implantation of a fertilized egg. If fertilization does not occur, the uterine lining is shed during menstruation. It also provides a regular indication of a woman's fertility and helps in family planning.
| 4. What is the importance of the zygote in human reproduction? | |
Ans. The zygote is the first cell that forms after fertilization and marks the beginning of a new individual's life. It is formed by the fusion of the genetic material from the sperm and egg cells. The zygote contains all the genetic information necessary for the development of a complete human being. The zygote undergoes cell division and differentiation to form an embryo, which further develops into a fetus. It is during the early stages of development that the zygote establishes the basic body plan and starts the process of organ formation. Without the zygote, human reproduction and the development of a new individual would not be possible.
| 5. What are the factors that affect human reproductive health? | |
Ans. Several factors can affect human reproductive health, including: 1. Age: Both male and female fertility decline with age, with women experiencing a more significant decline after the age of 35. Advanced age can increase the risk of infertility and pregnancy complications. 2. Lifestyle factors: Smoking, excessive alcohol consumption, drug abuse, and poor nutrition can negatively impact reproductive health in both men and women. Maintaining a healthy lifestyle is crucial for optimal reproductive function. 3. Hormonal imbalances: Hormonal disorders such as polycystic ovary syndrome (PCOS) and thyroid disorders can affect fertility and menstrual regularity in women. Similarly, hormonal imbalances in men can lead to reduced sperm production and quality. 4. Sexually transmitted infections (STIs): STIs, such as chlamydia and gonorrhea, can cause infertility if left untreated. It is important to practice safe sex and get regular check-ups to prevent and treat STIs. 5. Environmental factors: Exposure to certain chemicals, toxins, and pollutants in the environment can have detrimental effects on reproductive health. Prolonged exposure to these substances can lead to infertility, hormonal imbalances, and birth defects.
About this Document

1.5K Views

4.68/5 Rating

Apr 18, 2026 Last updated
Document Description: Revision Notes: Human Reproduction for NEET 2026 is part of Biology Class 12 preparation. The notes and questions for Revision Notes: Human Reproduction have been prepared according to the NEET exam syllabus. Information about Revision Notes: Human Reproduction covers topics like and Revision Notes: Human Reproduction Example, for NEET 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Revision Notes: Human Reproduction.
Introduction of Revision Notes: Human Reproduction in English is available as part of our Biology Class 12 for NEET & Revision Notes: Human Reproduction in Hindi for Biology Class 12 course. Download more important topics related with notes, lectures and mock test series for NEET Exam by signing up for free. NEET: Revision Notes: Human Reproduction
Description
Revision Notes: Human Reproduction of Biology Class 12 with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET exam.
Information about Revision Notes: Human Reproduction
In this doc you can find the meaning of Revision Notes: Human Reproduction defined & explained in the simplest way possible. Besides explaining types of Revision Notes: Human Reproduction theory, EduRev gives you an ample number of questions to practice Revision Notes: Human Reproduction tests, examples and also practice NEET tests

Related Searches
Important questions, ppt, Previous Year Questions with Solutions, Viva Questions, pdf , past year papers, Free, Sample Paper, shortcuts and tricks, practice quizzes, MCQs, Revision Notes: Human Reproduction, Summary, study material, Objective type Questions, video lectures, Revision Notes: Human Reproduction, Extra Questions, Revision Notes: Human Reproduction, Semester Notes, Exam, mock tests for examination;