Birth Control, Contraception & Medical Termination of Pregnancy

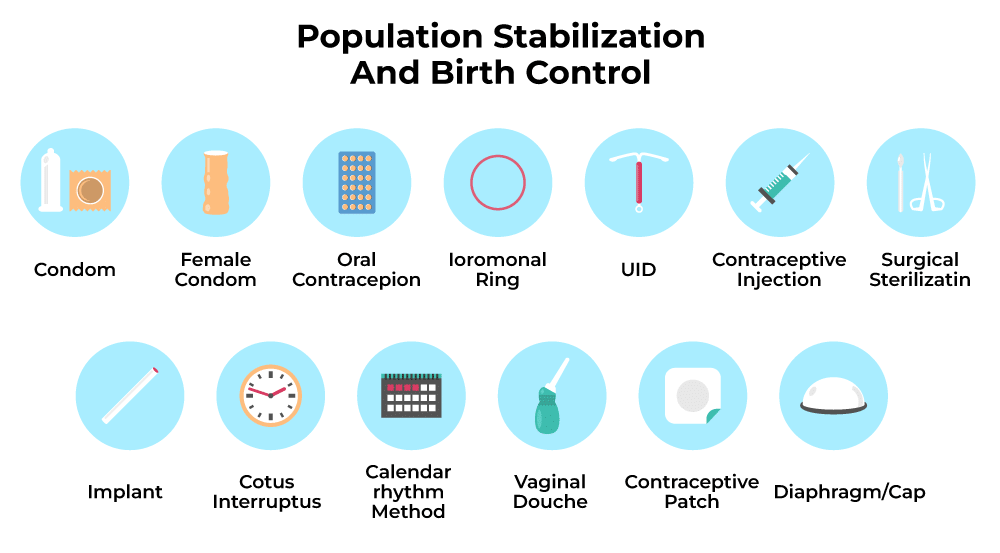
Population Stabilisation and Birth Control
Rapid Growth of Population
(a) Population Explosion in the 20th Century
Improvements in public health, nutrition, sanitation and medical care during the 20th century reduced mortality rates and increased life expectancy. These changes produced a rapid rise in global population: about 2 billion in 1900, about 6 billion by 2000 and approximately 7.2 billion by 2011.
(b) Population Growth in India
- India experienced a similar demographic transition. The population rose from roughly 350 million at independence to nearly a billion by 2000 and exceeded 1.2 billion by May 2011.
- Key contributors to this growth were a sharp decline in death rates, reductions in maternal mortality rate (MMR) and infant mortality rate (IMR), and an increased proportion of the population in the reproductive age group.
Efforts to Control Population Growth
- The Reproductive and Child Health (RCH) programme and other family planning initiatives aimed to reduce fertility and stabilise the population; these produced measurable benefits though the overall decline in growth rate was gradual.
- According to the 2011 census, although the decadal growth rate slowed, continued rapid increase in absolute numbers raised concerns about pressure on resources such as food, housing and employment.
- Governments have therefore used a mix of health services, information, incentives and legislation to promote smaller family norms and to limit population growth.
Measures to Encourage Smaller Families
- Awareness campaigns such as Hum Do Hamare Do (We Two, Our Two) promoted the benefits of smaller families.
- Some urban couples adopted an informal one-child norm, encouraged by social campaigns, incentives and public messaging.
- Legal measures and social policy included raising the minimum legal age of marriage to 18 years for females and 21 years for males, and offering incentives (economic or social) to couples who practised family planning.
 Hum Do Hamare Do
Hum Do Hamare DoContraceptive Methods
Contraceptive methods are procedures, devices or medicines used to prevent unwanted pregnancy. An ideal contraceptive is one that is easily available, simple to use, highly effective, reversible (unless permanent method is chosen), has minimal side effects, and does not interfere with sexual behaviour or desire.
Categories of Contraceptive Methods
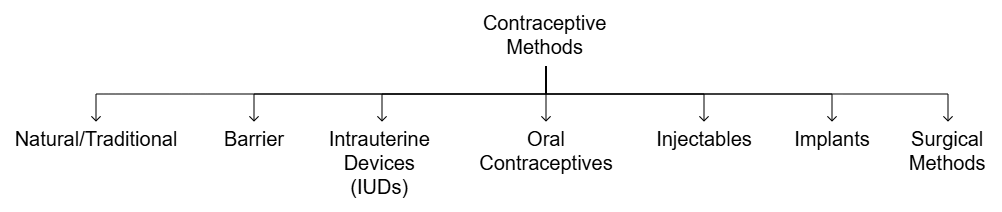 Types of Contraceptive Methods
Types of Contraceptive Methods1. Natural Methods
Natural methods prevent conception by avoiding intercourse during the fertile period or by using physiological conditions that reduce fertility.
- Periodic abstinence (rhythm method): Avoiding sexual intercourse around the expected time of ovulation (approximately days 10-17 in a typical 28-day cycle). This requires careful tracking of the menstrual cycle and is less reliable if cycles are irregular.
- Withdrawal (coitus interruptus): The male withdraws the penis from the vagina just before ejaculation to prevent semen entering the female tract. Failure rate is relatively high due to pre-ejaculate and timing errors.
- Lactational amenorrhoea: Intense breastfeeding suppresses ovulation for a time after childbirth. When exclusive breastfeeding is practised, the chance of conception is low, particularly during the first six months; effectiveness declines thereafter and if breastfeeding is not exclusive.
Advantages of natural methods include absence of medical side effects and no use of devices or medicines. Disadvantages include relatively high failure rates and the need for discipline and accurate knowledge of fertility signals.

2. Barrier Methods
Barrier methods physically prevent sperm from reaching the ovum. They are available for both males and females and can also reduce the transmission of sexually transmitted infections.
- Condoms
- Male condoms are sheath-like coverings made of latex or similar material, worn on the penis before intercourse to collect ejaculate and prevent sperm entry. Examples: commercial brands such as Nirodh. Male condoms also protect against many sexually transmitted infections including HIV/AIDS.
- Female condoms are inserted into the vagina before intercourse and form a barrier that lines the vaginal canal and covers the cervix. Both male and female condoms are disposable, can be self-used and provide privacy to users.
- Diaphragms, cervical caps and vaults: These are rubber devices inserted into the vagina to cover the cervix and block sperm entry; they are reusable and are often used with spermicidal agents to increase efficacy.
- Spermicidal creams, jellies and foams: Chemical agents that immobilise or kill sperm; commonly used together with barrier devices to improve contraceptive effectiveness.
 Male Condom
Male Condom Female Condom
Female CondomBarrier methods are generally reversible and carry few systemic side effects. Their effectiveness depends on correct and consistent use.
3. Intra Uterine Devices (IUDs)
IUDs are small devices inserted into the uterine cavity by a trained health professional. They provide long-term, reversible contraception and are among the most widely used methods.
Types of IUDs include:
- Non-medicated IUDs: e.g., the Lippes loop.
- Copper-releasing IUDs: e.g., CuT, Cu7, Multiload 375. Copper ions released locally affect sperm motility and viability.
- Hormone-releasing IUDs: e.g., Progestasert, LNG-20, which release progesterone (or its analogues) locally to alter the endometrium and cervical mucus.
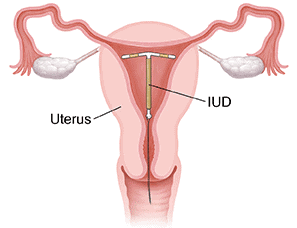 Placement of IUD in the Uterus
Placement of IUD in the Uterus- Mechanism: IUDs increase local uterine defence mechanisms such as phagocytosis of sperm and ova. Copper ions impair sperm motility and fertilising capacity. Hormone-releasing IUDs make the uterine lining less suitable for implantation and thicken cervical mucus to hinder sperm passage.
- Indications: Suitable for women who wish to delay pregnancy or space births. IUDs are long-acting, reversible and do not require daily attention.
- Advantages and limitations: IUDs are highly effective, cost-effective over time and reversible, but may cause local side effects such as spotting, heavier menstrual flow with copper IUDs, or hormonal side effects with LNG devices; insertion and removal must be performed by trained personnel.
4. Oral Contraceptives
Oral contraceptive pills contain progestogens alone or a combination of progestogen and oestrogen. They are taken orally and are widely used.
- Dosage and schedule: Combined oral contraceptive regimens commonly involve taking tablets daily for 21 days followed by a 7-day pill-free interval during which withdrawal bleeding occurs. Tablets are most effective when started within the first five days of the menstrual cycle and taken consistently at the same time each day.
- Mechanism of action: Pills prevent ovulation, thicken cervical mucus to obstruct sperm passage and alter the endometrium to reduce the likelihood of implantation.
- Effectiveness and side effects: When taken correctly they are very effective. Possible side effects include nausea, abdominal discomfort, breakthrough bleeding, and in some cases an increased risk of thromboembolic events or hormone-sensitive conditions. Women should choose pills under medical advice.
- Saheli: A non-steroidal oral contraceptive introduced as a \"once a week\" pill with fewer hormonal side effects; it offers an alternative mechanism and dosing schedule compared to conventional steroidal pills.
5. Injectables and Implants
- Injectables: Long-acting progestogen injections given at regular intervals (for example, monthly or quarterly) that suppress ovulation and change cervical mucus.
- Implants: Small rods placed under the skin (usually of the upper arm) that release progestogen continuously for months or years, providing long-term contraception.
- Both methods share mechanisms similar to oral hormonal methods but provide longer duration of action and do not require daily compliance. Side effects may include irregular bleeding patterns and hormone-related symptoms.
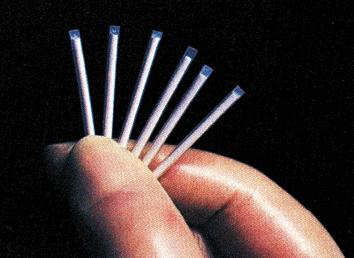 Implants
ImplantsEmergency Contraception:Emergency contraception reduces the risk of pregnancy after unprotected intercourse. Progestogen-only emergency pills (for example, those containing levonorgestrel) are most effective when taken as soon as possible and typically within 72 hours. A copper-bearing IUD inserted by a trained professional can be used as emergency contraception and is effective if inserted within five days of unprotected intercourse. Emergency methods should not be used as a regular contraceptive and are more effective the earlier they are used.
Emergency contraception is also important in cases of sexual assault or contraceptive failure.
6. Surgical Methods (Sterilisation)
Sterilisation is a permanent method of contraception for those who have decided not to have more children. It works by blocking the transport of gametes.
Sterilisation in Males: Vasectomy
- Procedure: A small portion of the vas deferens (the duct that carries sperm from the testes) is ligated and removed or tied; the operation is carried out through a small incision in the scrotum.
- Effect: Sperm cannot be transported in the ejaculate; sexual function and ejaculation remain normal because semen volume is largely from accessory glands, not sperm.
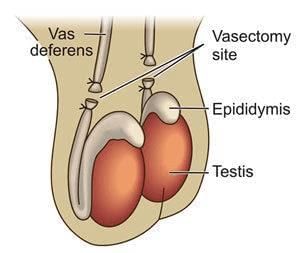 Vasectomy
VasectomySterilisation in Females: Tubectomy (Tubal Ligation)
- Procedure: A segment of the fallopian tube is removed or blocked through an abdominal or vaginal approach, preventing the ovum from reaching the uterus and sperm from reaching the ovum.
- Effect: It is a highly effective permanent method; reversal is complex and has limited success.
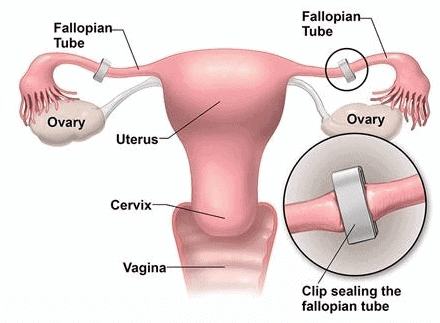 Tubectomy
Tubectomy- Both vasectomy and tubectomy are highly effective permanent methods. Reversibility is limited and should not be relied upon when choosing sterilisation.
(ii) Consultation and Considerations in Contraceptive Use
Consultation with Medical Professionals
- Selection of an appropriate contraceptive method should be made after consultation with a qualified medical practitioner who can advise on suitability, contraindications and expected side effects.
- Contraceptives are not routine requirements for health maintenance but are used for preventing, delaying or spacing pregnancies according to personal and family needs.
Role in Population Control
- Contraceptives contribute substantially to reducing fertility rates and achieving population stabilisation goals when combined with education and health services.
- Users should be informed about possible side effects such as nausea, abdominal pain, irregular bleeding, and, in rare cases, increased risk for hormone-related conditions; the benefits and risks must be balanced individually.
Balancing Benefits and Risks
- Widespread, informed use of contraception reduces unintended pregnancies and maternal mortality associated with unsafe abortion.
- Health professionals must provide counselling on correct use, management of side effects and alternative choices to ensure safe and acceptable family planning.
Medical Termination of Pregnancy (MTP)
Medical Termination of Pregnancy (MTP), also called induced abortion, is the intentional interruption of a pregnancy before the foetus reaches viability. It may be performed surgically or by approved medical regimens under conditions laid down by law and medical guidelines.
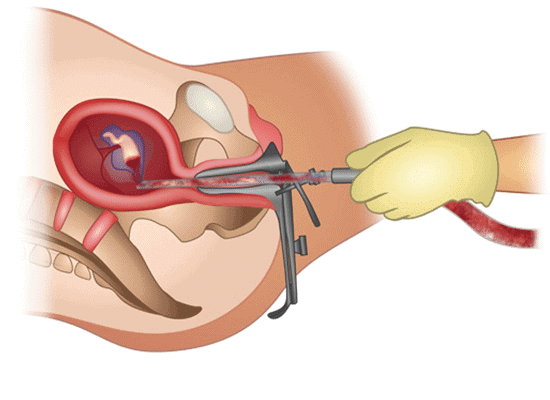 Medical Termination of Pregnancy (MTP)
Medical Termination of Pregnancy (MTP)- Globally, an estimated 45-50 million terminations are performed each year; they represent a significant proportion of conceived pregnancies annually. Legal, ethical and social issues about MTP vary across countries.
- In India, MTP was legalised in 1971 under specified conditions and safeguards to permit termination in certain circumstances and to reduce unsafe practices. Legal frameworks aim also to prevent misuse such as sex-selective terminations.
(i) Reasons for MTP
- Unwanted pregnancies: Arising from contraceptive failure, unprotected intercourse or sexual violence.
- Health risks: Pregnancies that threaten the life of the pregnant woman or would cause serious physical or mental harm to her; or where there is a substantial risk that the child will be born with serious physical or mental abnormalities.
(ii) Safety of MTP
- First trimester: Abortions performed in the first 12 weeks are generally safer, with lower complication rates, when carried out by trained providers in appropriate settings.
- Second trimester: Abortions after the first trimester carry higher medical risks and require greater clinical expertise and facilities.
(iii) Illegal and Unsafe Practices
- Unqualified practitioners: Unsafe abortions performed by untrained or unqualified persons pose serious health risks, including infection, haemorrhage and death.
- Misuse of prenatal diagnosis: The illegal use of diagnostic procedures (such as amniocentesis) to determine foetal sex, followed by sex-selective termination, is a serious social and legal problem and is prohibited.
(iv) Importance of Counselling and Healthcare Facilities
Counselling about the risks of unprotected intercourse, provision of contraception and safe, accessible healthcare facilities for MTP reduce the incidence of unsafe abortions and associated maternal morbidity and mortality. Post-abortion counselling and family planning services are essential to prevent repeat unintended pregnancies.
The Medical Termination of Pregnancy (Amendment) Act, 2017
 Medical Termination of Pregnancy (Amendment) Act, 2017
Medical Termination of Pregnancy (Amendment) Act, 2017- The 2017 amendment aimed to reduce unsafe abortions and associated maternal deaths by widening access under regulated conditions and clarifying the cadre of authorised providers.
- Under the amended provisions, termination of pregnancy up to 12 weeks may be authorised on the opinion of a single registered medical practitioner.
- For pregnancies beyond 12 weeks and up to 24 weeks, the opinion of two registered medical practitioners is required; they must be satisfied that the grounds for termination are met. Certain categories of women (for example, survivors of sexual assault, minors, and women with foetal malformations) are given special consideration.
Grounds for termination under the Act include:
- Risk to the pregnant woman: Where continuation of pregnancy would be life-threatening or would cause grave physical or mental injury to the woman.
- Risk of severe abnormality: Where there is substantial risk that the child, if born, would suffer from serious physical or mental abnormalities.
Medical Methods and Drugs
Medical termination in early pregnancy can be performed using approved drug regimens. One well-known drug is mifepristone (also called RU-486), administered under medical supervision and often followed by a prostaglandin analogue such as misoprostol to expel uterine contents. These methods must be used according to clinical guidelines and within legal time limits and settings to ensure safety.
Summary
Population stabilisation depends on a combination of informed family planning, accessible and acceptable contraceptive methods, safe clinical services for pregnancy termination where legally permitted, and social policies that encourage smaller families. Contraceptive options range from natural and barrier methods to hormonal, intrauterine, long-acting and permanent surgical methods; each option has specific mechanisms, advantages and limitations. Safe MTP services, legal safeguards, appropriate counselling and quality healthcare facilities reduce unsafe practices and protect maternal health.
FAQs on Birth Control, Contraception & Medical Termination of Pregnancy
| 1. What is the difference between birth control and contraception? |  |
| 2. What are the natural methods of contraception? | |
| 3. How do barrier methods of contraception work? | |
| 4. What are the benefits of oral contraceptives? | |
| 5. When should emergency contraceptives be used? | |