Chapter Notes: Physiology of Hearing and Audiology

Physiology of Hearing
When sound is detected by the pinna, it follows a specific pathway:
- Pinna → External Auditory Canal (EAC) → Tympanic Membrane (TM) → Ossicular Chain → Footplate of Stapes (Oval Window) → Organ of Corti → Eighth Cranial Nerve → Auditory Pathways → Auditory Cortex (Area No. 41).
Conductive Pathway
- Sound is conducted from the pinna to the footplate of the stapes. This pathway is known as the conductive pathway. Any defect in this pathway results in conductive deafness.
Sensory and Neural Hearing Loss
- The organ of Corti is the sensory organ for hearing. A defect in this area leads to sensory or cochlear hearing loss.
- Defects in the auditory nerves and pathways beyond the cochlea result in retro-cochlear or neural hearing loss.
- Sensory and neural hearing loss together are referred to as sensorineural hearing loss.
Mixed Hearing Loss
- Mixed hearing loss occurs when there are defects in both the conductive and sensorineural pathways.
Mechanism of Hearing: Transformer Action of the Middle Ear
- When sound travels from the external and middle ear to the inner ear, it changes from air to liquid. This transition can cause a significant amount of sound energy to be reflected back.
- To address this issue and match the impedance (resistance to sound flow) of the middle ear (which has low impedance) with that of the inner ear (which has high impedance), the middle ear acts like a transformer.
- Through this transformer action, the middle ear increases the force of sound entering it, allowing more sound to reach the inner ear instead of being reflected back.
- The middle ear changes sound from a higher amplitude and lower force to a lower amplitude and higher force, facilitating more sound entering the inner ear. This process is known as the transformer action of the middle ear.
- During normal hearing, the middle ear boosts sound intensity, but when noise levels are very loud (70-100 dB above the hearing threshold), it reduces sound intensity. This adjustment is made possible by the stapedius and tensor tympani muscles, which are part of the stapedial reflex.
Step-Up Phenomenon of Middle Ear
Areal Ratio (Hydraulic Ratio)
- The total area of the tympanic membrane (TM) is 90 mm², but not all of it is effective in conducting sound.
- The effective vibrating area of the TM is 55 mm², while the footplate of the stapes is only 3.2 mm².
- When sound is focused from the larger area of the TM to the smaller area of the stapes, the sound force increases based on the ratio of these areas.
- This ratio, known as the Areal Ratio, is 17:1 (55 mm²/3.2 mm²).
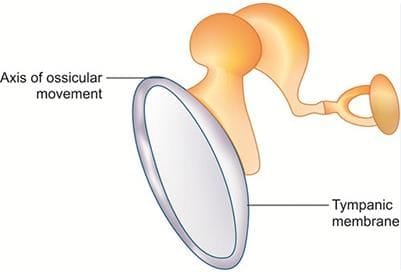
Lever Ratio
- The handle of the malleus is 1.3 times longer than the long process of the incus.
- This means the incus moves 1.3 times more than the malleus, resulting in a 1.3-fold increase in sound force.
- Therefore, the lever ratio is 1.3:1.
Total Transformer Ratio
- The total transformer ratio is the product of the Areal Ratio and the Lever Ratio.
- This is calculated as 17 × 1.3 = 22.
Transformer Action
- The transformer action increases the sound pressure at the inner ear by the stapes footplate to about 18-22 times higher than at the tympanic membrane.
- This compensates for the loss of sound energy due to the change of medium.
Minor Contributing Factors
- Curved Membrane Effect/Catenary Lever. The TM is more mobile at the edges than at the center, which enhances sound force. This effect doubles the amplification of sound pressure.
- Phase Difference. There is a timing difference in sound reaching the oval and round windows due to the different pathways through the ossicular chain and middle ear air. This phase difference aids in effective sound transmission to the inner ear fluids.
- Natural Resonance. Each part of the external and middle ear has its own resonating frequency, which enhances the transmission of sounds matching these frequencies. The resonating frequencies are:
- External auditory canal: 3000 Hz
- Tympanic membrane: 1000-3000 Hz
- Middle ear: 1000-3000 Hz
- Ossicles: 500-2000 Hz (normal speech frequencies)
Summary of Contributing Factors
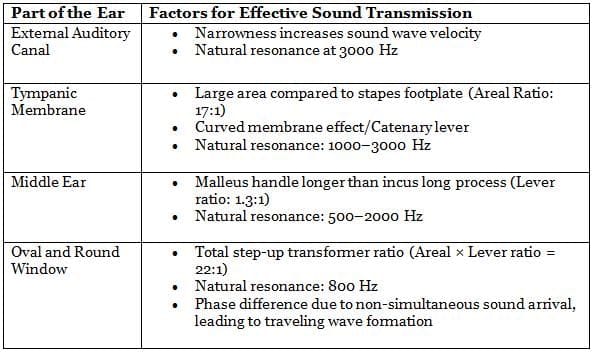
Overall, these factors work together to enhance the transmission of sound from the external and middle ear to the inner ear fluids, facilitating effective hearing.
Audiology
Tuning Fork Tests
Initial tests for patients with hearing complaints in the ENT outpatient department.
Commonly performed tests include:
- Rinne's test
- Weber test
- Absolute bone conduction (ABC) test
- Schwabach's test
- Bing test
- Gelé's test
These tests help locate the problem and estimate the degree of hearing loss.
Typically use a 512 Hz tuning fork for better audibility. In neurology, a 126 Hz tuning fork is used to assess vibration sense due to its stronger sensation.
Higher frequencies above 512 Hz fade quickly and are less commonly used for certain tests.
To activate the tuning fork, strike it gently against the elbow to avoid unwanted sounds that can interfere with the tone produced.
Air Conduction (AC)
- Tuning fork placed 2 cm in front of the pinna.
- Sound pathway:
- Pinna
- External auditory canal (EAC)
- Tympanic membrane (TM)
- Ossicular chain
- Footplate of stapes (oval window)
- Organ of Corti
- 8th nerve
- Auditory pathway
- Auditory cortex (area no. 41)
Air conduction (AC) assesses all three pathways: conductive, sensory, and neural.
Bone Conduction (BC)
- Tuning fork placed over the mastoid.
- Bone conduction pathway:
- Vibrating tuning fork
- Vibration of the skull
- Movement of cochlear fluid
- Stimulation of organ of Corti
- 8th nerve
- Auditory pathway
- Auditory cortex (area no. 41)
Bone conduction (BC) measures the sensory and neural pathways. Both air conduction and bone conduction share common sensory and neural pathways.
Air conduction (AC) typically louder and longer-lasting than bone conduction (BC) in normal ears.
1. Rinne's Test
- In this test, we compare air conduction (AC) and bone conduction (BC) in the same ear to see which is better.
- Rinne's test can be either positive or negative.
- Positive Rinne. This means AC is better than BC.
- Negative Rinne. This means BC is better than AC.
- When Rinne is positive (AC > BC), there are two possibilities:
- Normal Ear. AC is better than BC, which is normal.
- Sensorineural Deafness. Both AC and BC are reduced, but AC is still better. This happens because sound passes through the middle ear and reaches the inner ear more effectively.
- Rinne is positive in both a normal ear and in cases of sensorineural deafness.
- When Rinne is negative (BC > AC), there are two possibilities:
- Conductive Deafness. This means the patient hears better through bone conduction, indicating a problem in the conductive pathway.
- Rinne Test Sensitivity. The Rinne test is not very sensitive and can only detect conductive hearing loss greater than 15-20 dB.
- Tuning Fork Frequencies. If Rinne is negative with 256 Hz, 512 Hz, and 1024 Hz tuning forks, it suggests hearing loss of approximately 15 dB, 30 dB, and 45 dB, respectively.
- Audiometry. The exact degree of hearing loss is better assessed through audiometry.
- Severe Sensorineural Hearing Loss. In cases of severe sensorineural hearing loss on one side, the patient may not hear either air or bone conduction sounds on that side.
- During bone conduction testing, sound travels through the skull and stimulates the normal cochlea on the opposite side, allowing the patient to hear from the normal ear. This can result in BC being better than AC, making Rinne test negative. However, this negative result is a false negative.
- Conductive Deafness. Rinne is negative in cases of conductive deafness.
- Severe Sensorineural Deafness. Rinne can be falsely negative in severe sensorineural deafness, which can delay the diagnosis and treatment of this condition, potentially leading to irreversible damage.
- To differentiate between a true negative and a false negative Rinne result, Weber's test is performed.
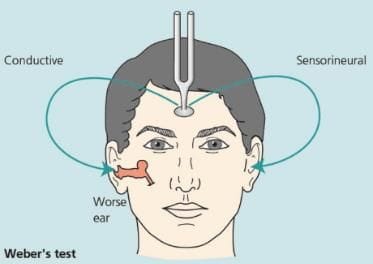
2. Weber Test
- The vibrating tuning fork is placed on the forehead or teeth, and the patient is asked to identify which ear hears the sound louder.
- This test is highly sensitive, capable of detecting lateralisation with as little as a 5 dB difference between the ears.
- Weber's test evaluates bone conduction (BC) and compares it between both sides.
- In individuals with normal hearing, sound is perceived equally in both ears.
Sensorineural (SN) Hearing Loss
- In cases of SN hearing loss, the sound lateralises towards the better ear, indicating that the patient hears it more clearly in that ear.
- This occurs because bone conduction (BC) is decreased in the affected ear, making it better heard in the ear with normal SN pathways.
- Both mild to moderate and severe SN hearing loss exhibit lateralisation towards the better ear.
Conductive Hearing Loss
- In conductive hearing loss, the Weber test lateralises to the worse ear, meaning the patient hears the sound better in that ear.
- This phenomenon occurs because ambient noise entering through air conduction (AC) interferes with sound transmission via the SN pathway in the normal ear.
- For instance, in conditions like secretory otitis media (SOM) or otosclerosis, patients perceive their own voice as louder.
- This is due to the fact that speaking vibrates the jaw, directly stimulating BC.
- As a result, patients with conductive hearing loss produce a low tone speech, in contrast to those with SN hearing loss who struggle to hear their own voice and speak loudly.
- In summary, Weber's test lateralises to the worse ear in conductive hearing loss and to the better ear in sensorineural hearing loss. (Mnemonic: We Create-Best Students).
3. Absolute Bone Conduction Test
- The Absolute Bone Conduction (ABC) Test is specifically designed to evaluate bone conduction, which is related to sensorineural (SN) deafness.
- In this test, the bone conduction of the patient is compared to that of the examiner, who is assumed to have normal hearing.
- Both the patient and the examiner experience conductive hearing loss during the test by pressing the tragus, which blocks the external auditory canal.
- The ABC Test is exclusively used for diagnosing sensorineural hearing loss.
- The test procedure involves placing a vibrating tuning fork on the patient's mastoid while the external auditory canal is blocked.
- When the patient can no longer hear the tuning fork, it is then placed on the examiner's mastoid.
- If the examiner can still hear it, this indicates that the patient's bone conduction is decreased.
- However, it is important to note that decreased bone conduction does not automatically indicate sensorineural hearing loss, as it may indicate other types of hearing impairment.
- In cases of sensorineural hearing loss, the ABC is reduced when comparing the patient's results to those of the examiner.
4. Schwabach's Test
- Schwabach's Test is similar to the ABC test, but in this case, the meatus is not blocked. This allows for an assessment of the conductive pathway as well.
- Sensorineural Hearing Loss. If the examiner has normal hearing and the patient's bone conduction (BC) is shorter than the examiner's, it indicates that the patient's sensorineural (SN) pathway is affected, suggesting SN hearing loss.
- Normal Hearing. If the patient's BC matches the examiner's, it signifies that the patient's hearing is normal, similar to the examiner's.
- Conductive Hearing Loss. If the patient hears the BC for a longer time than the examiner, it indicates that the patient has conductive hearing loss. This occurs because the sound is not disrupted by outside noise entering through the air conduction (AC) route, which is faulty due to issues in the conductive pathway.
- Duration Differences. Schwabach's test shows a shortened duration in SN hearing loss and an extended duration in conductive hearing loss. To remember this, think of the phrase: 'Students Let's Conclude and Study Summary' → Schwabach's is Lengthened in Conductive and Shortened in Sensorineural hearing loss.
5. Bing Test
- The Bing test involves using a vibrating tuning fork placed on the bone behind the ear (mastoid process).
- The ear canal is alternately left open and blocked while the patient listens.
- The patient is asked to indicate whether the sound is louder with the ear open or blocked.
- In cases of conductive hearing loss, there is no difference in sound perception whether the ear is open or blocked, resulting in a Bing negative.
- If the patient's hearing is normal or if they have sensorineural deafness, the sound will be perceived as louder when the ear is blocked due to the reduction of background noise, resulting in a Bing positive.
- Similar to the Rinne test, the Bing test is negative in cases of conductive deafness.
6. Gelle's Test
- Gelle's Test involves using a Siegel's speculum to insert into the external auditory canal (EAC) while a vibrating tuning fork is placed on the mastoid bone.
- Increasing pressure in the EAC pushes the tympanic membrane (TM) inward, which reduces the movement of the ossicles and improves hearing. This occurs because the added pressure creates a conductive hearing loss, effectively masking background noise.
- When the pressure is released, both the ossicular chain and TM regain their mobility, restoring normal hearing. This phenomenon, where hearing changes due to pressure adjustments in the EAC, is known as Gelle's positive.
- In cases where the ossicular chain is fixed, there will be no change in hearing with pressure variations, a condition called Gelle's negative. This is commonly seen in conditions like otosclerosis.
- Similar observations to Gelle's Test are noted in the Rinne and Bing tests for individuals with normal hearing and those with sensorineural deafness.
Audiometric Tests
Audiometric tests are used to assess hearing ability and identify the type and degree of hearing loss. The first audiometric test, known as "Bekesy" audiometry, was developed by Von Bekesy, a Nobel Prize winner in Physiology or Medicine for his work on travelling waves in the cochlea. However, this test is no longer in use today.
Pure Tone Audiometry (PTA)
Pure Tone Audiometry (PTA) is a widely used test to evaluate air conduction (AC) and bone conduction (BC) of sound in the ear. It is conducted using an electronic device called an audiometer, typically in a soundproof room.
- PTA helps identify the type of hearing loss, whether it is conductive, sensorineural (SN), or mixed.
- It also provides an accurate measure of the degree of hearing loss, which can indicate the specific location of the defect in the ear.
In PTA, the intensity of sound is measured in decibels (dB). The formula used is: dB = 20 log SPLo/SPLR, where SPLo is the sound pressure level of the tested sound and SPLR is the sound pressure level of a reference sound.
- PTA tests a wide range of sound frequencies. The human ear can detect frequencies from 20 Hz to 20,000 Hz, but in standard audiometry, AC is measured for frequencies from 125 Hz to 8000 Hz, while BC is measured from 250 Hz to 4000 Hz.
- Pathologies and Approximate Hearing Loss: Various ear conditions and their associated hearing loss levels are as follows:
- Complete obstruction of the ear canal
- Perforation of the tympanic membrane (TM): 10-40 dB
- Ossicular interruption with intact TM: 54 dB
- Ossicular interruption with perforated TM: 38 dB (less loss due to direct sound transmission through the perforation)
- Complete fixation of the footplate: 60 dB
- High-frequency audiometry tests frequencies ranging from 8000 Hz to 20,000 Hz. It is important to note that most human speech falls within the frequency range of 500 Hz to 2000 Hz, which are referred to as speech frequencies (500 Hz, 1000 Hz, and 2000 Hz).
- Degree of Hearing Loss: During PTA, the thresholds for determining normal hearing are as follows:
- Air Conduction (AC) threshold: Up to 15 dB is considered normal.
- Bone Conduction (BC) threshold: Up to 25 dB is considered normal.
- Hearing loss is classified based on these thresholds, with variations in criteria set by organizations such as the American Speech-Language-Hearing Association (ASHA) and the World Health Organization (WHO).
Audiogram
- The results of PTA are visually represented on a graph called an audiogram.
- In the audiogram, different symbols are used to indicate the hearing thresholds for each ear.
- The right ear is marked in red, and the left ear is marked in blue on the audiogram. A helpful mnemonic to remember this is "R for Right."
Masking
When a sound reaches one ear through the air, it also travels to the other ear via the air. During this process, some sound is lost, resulting in interaural attenuation of about 40 dB. For instance, if a sound of 60 dB is heard in the right ear, it will only be perceived as 20 dB in the left ear.
If a patient has a hearing loss greater than 50 dB in one ear and a 50 dB sound is presented to that ear, they won't hear it, but they may hear a 10 dB sound in the other ear and respond. This can lead to incorrect results. Therefore, masking is essential to prevent the better ear from participating in the hearing test while assessing the worse ear.
Hearing loss
- ASHA:
- Mild: 26-40
- Moderate: 41-55
- Moderately severe: 56-70
- Profound: >91
- WHO:
- 41-60
- 61-80
- >81
In Table 2.4, according to ASHA, there is an increase of 15 dB, except in severe cases where the range is 20 dB. Thus, air conduction (AC) or bone conduction (BC) thresholds above 90 dB are considered profound hearing loss. WHO guidelines indicate a change in hearing loss degree at every 20 dB, with AC or BC thresholds at or above 81 dB being profound hearing loss. ASHA also includes an additional category for moderately severe hearing loss.
Masking is necessary when there is a difference of at least 40 dB between the two ears in the air conduction threshold.
For bone conduction, the interaural attenuation is 0 dB, so masking the better ear is required for all bone conduction sounds.
Masking is achieved by presenting a complex noise to the ear.
Steps to Read Any Audiogram
- Determine the Ear: Check if the audiogram displays results for the right ear, left ear, or both.
- Identify Curves: Look for the Air Conduction (AC) and Bone Conduction (BC) curves using the symbols from Table 2.5.
- AC Curve Normality: If the AC curve is normal (below 25 dB) and present, the ear is considered normal. The AC curve assesses both conductive and sensorineural pathways, and the BC curve, which evaluates only the sensorineural pathway, is not needed.
- Abnormality Threshold: If the AC/BC curve exceeds 25 dB, it is considered abnormal.
- Check AB Gap:
- AB Gap Present: If the AB gap is greater than 15 dB, it indicates conductive hearing loss (CHL).
- If the AB gap is absent or less than 15 dB, it suggests sensorineural hearing loss.
- AC and BC Curves: If the AC curve is abnormal and the BC curve is normal or not provided (assume it is normal), this indicates CHL.
- Examine Curve Shapes: Look at the shapes of the curves-upsloping, downsloping, U-shaped, Carhart notch, and acoustic dip-to identify potential underlying causes.
Calculation of Hearing Impairment and Degree of Handicap
Hearing impairment is assessed by calculating the percentage of hearing impairment based on the average hearing thresholds at specific frequencies. The degree of handicap is then determined by considering the impairment in both ears.
Steps to Calculate Percentage of Hearing Impairment
- Step 1: Calculate Average Hearing Threshold
- Obtain the hearing thresholds at 500 Hz, 1000 Hz, and 2000 Hz from the audiogram.
- Calculate the average of these thresholds. For example, if the thresholds are 30 dB, 45 dB, and 60 dB, the average is 45 dB.
- Step 2: Adjust the Average Threshold
- Subtract 25 dB from the average threshold. This adjustment is made because hearing up to 25 dB is considered normal.
- Using the previous example, 45 dB. 25 dB. 20 dB.
- Step 3: Calculate Percentage Hearing Loss
- Multiply the adjusted figure by 1.5 to obtain the percentage of hearing loss.
- Continuing with the example, 20 dB. 1.5. 30% hearing loss.
Formula for Overall Impact of Hearing Impairment
To determine the overall impact of hearing impairment, use the following formula:
- ( % hearing impairment of the better ear × 5. + ( % hearing impairment of the worse ear ) divided by 6.
High-Frequency Audiometry
High-Frequency Audiometry is a specialized hearing test that focuses on frequencies ranging from 8000 Hz to 20,000 Hz. This method is particularly useful for detecting early signs of ototoxicity and noise-induced hearing loss, conditions that typically lead to high-frequency hearing loss. By identifying these issues early, it is possible to prevent or mitigate problems with lower frequencies, which are crucial for understanding speech.
In contrast, conventional audiometry tests frequencies between 250 Hz and 8000 Hz.
Impedance Audiometry
Impedance audiometry is a vital, objective test used in hearing assessments, unlike subjective methods such as tuning fork tests and pure tone audiometry (PTA). It comprises two main tests: tympanometry and stapedial reflex/acoustic reflex.
Tympanometry evaluates the middle ear's condition by measuring the impedance (resistance) to sound energy as pressure varies in the external auditory canal (EAC). A probe with three channels is inserted into the EAC, delivering a sound frequency of 226 Hz or 220 Hz (or 1000 Hz for infants. to the tympanic membrane (TM). The reflected sound is detected, and EAC pressure is adjusted from +200 to -400 mm of H2O. The point of maximum TM mobility indicates the middle ear pressure and compliance.
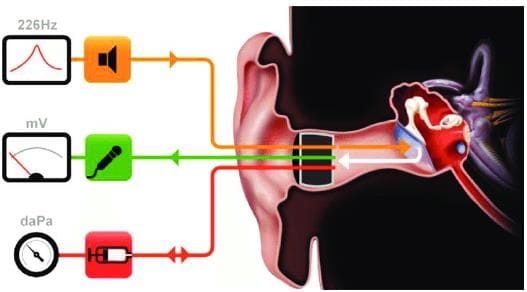 Tympanogram probe with three channels
Tympanogram probe with three channels
- Compliance refers to the TM's ease of movement, with higher compliance indicating conditions like ossicular discontinuity and lower compliance indicating ossicular fixation or fluid in the middle ear.
- Middle ear pressure is typically around 0 mm of H2O, with adult ranges between -50 and +50 mm of H2O and children's ranges from -150 to +50 mm of H2O.
A tympanogram graphically represents the results, with the X-axis showing pressure and the Y-axis showing compliance.
Types of Patterns on the Tympanogram
- Type A: This pattern indicates normal middle ear pressure and compliance, typically observed in a healthy middle ear.
- Type AS: In this type, compliance is decreased while Eustachian tube function remains normal, resulting in normal middle ear pressure. The 'S' stands for stiffness, often seen in conditions like otosclerosis or ossicular fixation. It can also occur in tympanosclerosis and middle ear tumors such as glomus jugulare.
- Type AD: This pattern is characterized by increased compliance, meaning the tympanic membrane (TM) moves excessively while middle ear pressure is normal. Type AD is associated with ossicular discontinuity ('D' for discontinuity) and a thin or lax TM, as well as in post-stapedectomy cases.
- Type C: Type C indicates negative middle ear pressure due to Eustachian tube closure (C for Closure), while compliance remains normal. This condition is typically short-term and insufficient for fluid collection, commonly observed in early Eustachian tube obstruction.
- Type B: Type B occurs when the Eustachian tube is blocked (B) for an extended period, leading to fluid accumulation in the middle ear. This results in decreased compliance, negative middle ear pressure, and a dome-shaped curve with reduced compliance and no sharp peak. Type B is commonly seen in serous otitis media (SOM) and adhesive otitis media. A mnemonic for this is SOM, which can be remembered as Blocked Eustachian tube Otitis media (type B curve).
- When fluid completely fills the middle ear cavity, causing no TM movement, a flat curve appears. This can be remembered with the mnemonic FFF - Fluid Fill completely - Flat curve.
- In cases of TM perforation, tympanometry cannot be performed as pressure changes on the TM are not possible, resulting in a flat curve. A mnemonic in Hindi for this is Fatta TM - Flat curve, observed in late SOM and TM perforation.
- Tympanometry can still assess Eustachian tube function in cases of TM perforation. This is done by sealing the ear canal with a probe and applying positive or negative pressure of +200 or -200 mm of H2O. The patient is instructed to swallow five times in 20 seconds. If the Eustachian tube is functioning normally, pressure equilibrates to atmospheric pressure after swallowing.
Acoustic/Stapedial Reflex
The acoustic or stapedial reflex is a protective mechanism of the inner ear that is triggered by loud sounds. Here's how it works:
- When a loud sound, typically between 70-100 dB, is heard in one ear, the stapedius muscle in both ears contracts.
- This contraction reduces the movement of the stapes bone, which is one of the tiny bones in the middle ear.
- By reducing the movement of the stapes, the reflex helps protect the inner ear from potential damage caused by loud noises.
Pathways Involved:
- The afferent pathway for the stapedial reflex is controlled by the 8th cranial nerve, which is responsible for carrying sound information from the ear to the brain.
- The efferent pathway is controlled by the 7th cranial nerve, which sends signals to the stapedius muscle to contract.
- This reflex occurs in both ears, even if the sound is only heard in one ear, indicating that it is a bilateral reflex.
Clinical Significance:
- If the stapedial reflex is present, it indicates that there are no issues with the afferent pathway, central connections, or efferent pathway of this reflex.
- In afferent palsy, the stapedial reflex is absent on both sides, meaning there is a problem with the afferent pathway.
- In efferent palsy, also known as facial nerve palsy, the reflex is absent only on the affected side (the ipsilateral side), indicating a problem with the efferent pathway.
Delay in Reflex:
- The acoustic/stapedial reflex takes about 100-200 milliseconds to activate after a loud sound is heard.
- If a sound exceeds 140 dB, it can reach the cochlea (the hearing part of the inner ear) before the reflex kicks in, potentially leading to permanent hearing loss.
Clinical Importance of the Stapedial/Acoustic Reflex
- Detecting Malingering: When someone claims complete deafness in an ear, a normal stapedial reflex on the same side indicates that the ear is not truly deaf. A normal reflex shows that the involved pathways and systems are functioning correctly.
- Differentiating Types of Hearing Loss: In a healthy ear, the acoustic reflex threshold is typically 70 to 100 dB above the pure tone hearing threshold. In cases of cochlear problems, the reflex activates at 60 dB above the pure tone threshold due to a phenomenon called recruitment, where loud sounds are perceived to be much louder than normal. Conversely, in retrocochlear issues, the reflex threshold may be elevated or absent, depending on the severity and nature of the condition.
- Acoustic Reflex Decay Test: This test involves playing a sound at 500 or 1000 Hz for 10 seconds at approximately 10 dB above the acoustic reflex threshold. If the reflex amplitude decreases to less than 5% within 5 seconds, it indicates abnormal decay, suggesting rapid fading of the reflex. This rapid decline points to potential nerve fatigue and retrocochlear problems.
- Diagnosing Facial Nerve Palsy: In patients with facial nerve palsy, the presence of a stapedial reflex indicates that the injury to the facial nerve is located beyond the nerve's connection to the stapedius muscle. If the facial nerve is injured before this point, the reflex will be absent, leading to a condition known as hyperacusis, where normal sounds are perceived as excessively loud and potentially painful.
Recruitment in Cochlear Problems
Recruitment refers to an abnormal increase in loudness perception, where an ear that typically struggles to detect soft sounds begins to hear louder sounds, potentially even louder than what a normal ear would hear. This phenomenon is commonly associated with cochlear issues.
Testing for Recruitment
The presence of recruitment can be evaluated using two specific tests: the "ABLB" and "SISI" tests.
- ABLB Test: The Alternate Binaural Loudness Balance (ABLB) test is used in cases of unilateral cochlear lesions.
- Test Procedure: In the ABLB test, a specific frequency is presented to the patient's left ear (the normal ear) at 0 dB loudness, which serves as a reference sound level. To hear the same sound in the defective right ear, the loudness must be increased significantly.
- Interpretation: The test reveals that as loudness increases, an 80 dB sound in the left ear, which should be heard at 110 dB in the right ear, is only heard at 80 dB in the right ear. This discrepancy indicates right-sided cochlear deafness in the patient.
- Conductive Hearing Loss: Figure 2.8A illustrates a patient with conductive hearing loss in the right ear at 20 dB, consistent across all sound intensities.
- SISI Test: The Short Increment Sensitivity Index (SISI) test assesses the ability of the recruiting ear to detect small increases in sound.
- Normal vs. Recruiting Ear:. normal ear cannot perceive a 1 dB increase, such as between 25 dB and 26 dB or between 40 dB and 41 dB. In contrast, a recruiting ear, typically seen in cases of cochlear lesions, can detect these small 1 dB increments.
- Test Procedure: The SISI test begins 20 dB above the patient's hearing threshold, presenting 20 increments of 1 dB every 5 seconds. The total number of increments identified by the patient is recorded.
- Interpretation:. SISI score of 70-100% suggests a cochlear lesion, while a score of 0-20% indicates a retrocochlear problem.
Tone Decay: An Overview
- Tone decay is a concept related to nerve fatigue, much like acoustic reflex decay.
- In a tone decay test, a tone at a specific frequency is played continuously for 1 minute at a level of 30 dB above the patient's Pure Tone Average (PTA) threshold.
- If the patient can hear the sound for the full 1 minute, it indicates that their nerves are functioning normally.
- However, if the nerves are fatigued, the patient may stop hearing the sound before the 1 minute is up.
- In such cases, the loudness of the sound is increased until the patient can hear it for the entire minute.
- If the loudness needs to be raised by more than 30 dB for the patient to hear the sound continuously for 1 minute, it may suggest the possibility of retrocochlear hearing loss.
Electrocochleography (Eco G)
Eco G is a diagnostic test that evaluates the electrical activity of the cochlea and the auditory nerve in response to sound. This test is particularly useful for diagnosing conditions like Menière's disease.
During the procedure, an electrode is inserted through the tympanic membrane (TM) and positioned on the promontory of the cochlea. The test records three important aspects of electrical activity:
- Cochlear microphonic (CM): This reflects the electrical activity generated by the hair cells in the cochlea in response to sound.
- Summating potential (SP): This represents the total electrical activity occurring within the cochlea.
- Action potential (AP): This indicates the electrical activity in the distal part of the auditory nerve and corresponds to wave I in Brainstem Evoked Response Audiometry (BERA).
Typically, the Action Potential (AP) is greater than the Summating Potential (SP). However, certain conditions can alter this relationship. The ratio of SP to AP (SP/AP) is usually less than 45%. In cases of cochlear disorders such as Menière's disease, this ratio is often greater than 0.45 (or 45%).
Otoacoustic Emissions (OAEs)
Otoacoustic Emissions (OAEs) are a type of objective test used to assess hearing. They are based on the biological activity of the outer hair cells in the cochlea, which produce sound that can be detected and recorded.
Types of Otoacoustic Emissions (OAEs)
- Spontaneous OAEs: These sounds are produced spontaneously by the outer hair cells without any external stimulation. They are found in about 50% of individuals with normal hearing.
- Evoked OAEs: These sounds are generated in response to an external sound stimulus. Evoked OAEs are present in all individuals with normal hearing.
Transient Evoked OAEs (TEOAEs):
- TEOAEs are elicited by a transient sound stimulus, such as a click or tone pip.
- The click sounds used in TEOAEs stimulate a large area of the basilar membrane, providing information about the overall function of the cochlea.
- TEOAEs are useful for assessing the presence and function of the entire cochlea.
Distortion Product OAEs (DPOAEs):
- DPOAEs are generated when two pure tones of different frequencies (F1 and F2) are presented to the ear simultaneously.
- The distortion product is a continuous tone with a frequency calculated as 2F1 - F2.
- DPOAEs provide frequency-specific information about the cochlea and are useful for assessing hearing sensitivity at specific frequencies.
Clinical Application of OAEs:
- OAEs are valuable in diagnosing hearing loss and assessing cochlear function.
- Absent TEOAEs or DPOAEs can indicate hearing loss, especially when pure-tone thresholds exceed 35 dB for TEOAEs and 40 dB for both TEOAEs and DPOAEs.
- OAEs are particularly useful in newborn hearing screening and monitoring cochlear function in individuals at risk of hearing loss.
Limitations of OAEs:
- OAEs may be absent in individuals with significant outer or middle ear pathology, regardless of cochlear function.
- Factors such as background noise and external ear canal conditions can affect the detection of OAEs.
Applications of Otoacoustic Emissions (OAE) Testing
- OAE testing is easy to perform, non-invasive, quick, and cost-effective, providing immediate results.
- It is commonly used for screening hearing in large groups, especially in healthy newborns, infants, and young children.
- For newborns in the Intensive Care Unit (ICU), Brainstem Evoked Response Audiometry (BERA) is used for initial screening.
- Transient Evoked OAEs (TEOAEs) are the most frequently used type for healthy infants.
- If the OAE response is within acceptable limits, it is marked as "Pass"; if not, it is marked as "Refer," indicating the need for further testing with BERA.
- The term "Fail" is avoided to prevent causing unnecessary concern for parents.
- Absent OAEs may suggest potential cochlear lesions, but additional testing is necessary for confirmation.
- To distinguish between cochlear and retro-cochlear hearing loss:
- If a patient with sensorineural (SN) hearing loss has present OAEs, it indicates that the cochlea is functioning normally, suggesting retro-cochlear hearing loss.
- The patient can then undergo BERA to pinpoint the exact location of the lesion.
- OAEs are useful for the early detection of noise-induced hearing loss because outer hair cells are especially vulnerable to damage from noise and ototoxic substances.
- Since OAEs are produced by outer hair cells, their absence can be an early indicator of damage.
- OAEs are also used to monitor cochlear function in patients receiving potentially ototoxic medications, such as cisplatin during chemotherapy.
- Distortion Product OAEs are specifically employed in these situations, followed by high-frequency audiometry to confirm and assess the severity of hearing loss.
Brainstem Evoked Response Audiometry (BERA/ABR)
BERA is an objective test that measures the electrical activity in the auditory pathway within the brainstem. Unlike Otoacoustic Emissions (OAEs), which detect natural electrical activity from the cochlea's outer hair cells, BERA focuses on the brainstem's response to sound, occurring within 10 milliseconds of sound detection.
In a typical BERA test, a graph displays 5-7 electrical waves, with latency (the time it takes for the wave to appear after the sound stimulus) on the x-axis and amplitude on the y-axis. These waves are generated from various points along the auditory pathway, with Wave V being the most prominent and significant.
Wave Origins
- Wave I: Distal part of the cochlear nerve in the inner ear.
- Wave II: Proximal part of the cochlear nerve near the brainstem.
- Wave III: Cochlear nucleus.
- Wave IV: Superior olivary complex.
- Wave V: Lateral lemniscus (the largest and most consistent wave).
- Wave VI and VII: Inferior colliculus.
The remaining waves also originate from the superior olivary complex and the lateral lemniscus.
Understanding BERA Results
- Delayed Wave I with normal interpeak latency of I-V: This suggests an issue before Wave I, likely in the distal part of the cochlear nerve. It points to potential problems in the cochlea or middle ear, indicating either conductive or cochlear pathology.
- Present Wave I with absent subsequent waves: This indicates a retrocochlear pathology.
- Increased inter-peak latency of wave I-V: This suggests a possible issue between the cochlear nerve and the lateral lemniscus, which could indicate acoustic neuroma.
- Increased interaural latency of wave V greater than 0.2 msec: Normally, waves appear simultaneously in both ears, meaning they have the same latency. The interaural latency difference is the time difference in the appearance of the same wave in both ears. If wave V appears later in one ear, a difference greater than 0.2 msec suggests retrocochlear pathology in that ear. This finding is significant, but other signs may also indicate acoustic neuroma.
Applications of BERA
- Determining Hearing Thresholds: Wave V is detected at 10 dB above the Pure Tone Audiometry (PTA) hearing level. To identify the PTA hearing threshold, subtract 10 dB from the level at which wave V is first observed.
- Confirming Hearing Loss: BERA is the most reliable audiometric test for confirming hearing loss in neonates, infants, and individuals with intellectual disabilities. While Otoacoustic Emissions (OAEs) are the best screening test, BERA is used as a screening test for neonates in the ICU for over 48 hours due to its higher sensitivity and specificity.
- Identifying Non-Organic Hearing Loss: BERA is the most effective test for identifying non-organic hearing loss, such as malingering.
- Differentiating Hearing Loss Types: BERA differentiates between cochlear and retro-cochlear hearing loss. The exact location of the lesion can be determined by analyzing the latency and amplitude of the affected wave.
- Detecting Acoustic Neuroma: BERA is the best audiometric test for detecting acoustic neuroma.
- Investigating Central Auditory Disorders: BERA is used to investigate central auditory disorders.
- Important Note: Patients with severe to profound hearing loss may not show measurable responses on BERA testing. Hearing assessments in such cases should be performed using Auditory Steady-State Response (ASSR).
- Recording in Premature Infants: BERA can be recorded in premature infants as young as 27 weeks, but the detection of waves I, III, and V improves with gestational age due to the maturation of auditory pathways. By 18 months to 3 years, BERA waveforms resemble those of adults.
High-Risk Neonates and Infants for Hearing Loss
The following neonates and infants are at high risk of developing hearing loss and should be tested periodically with behavioral observation audiometry, even if they pass Transient Evoked Otoacoustic Emissions (TEOAE) at birth:
- In Utero Infections: History of in utero infections such as Cytomegalovirus (CMV), herpes, Rubella, syphilis, and toxoplasmosis.
- Maternal Use of Ototoxic Drugs: Use of ototoxic drugs by the mother during pregnancy.
- Postnatal Infections: Postnatal infections like bacterial meningitis and encephalitis.
- Severe Hyperbilirubinemia: Severe hyperbilirubinemia in the neonate.
- Craniofacial Anomalies: Neonates with craniofacial anomalies.
- Syndromes Associated with Hearing Loss: Any syndrome associated with hearing loss, such as Down's syndrome or Treacher-Collins syndrome.
- Family History of Early Childhood Deafness: Family history of early childhood deafness.
Clinical Evaluation of Hearing Loss in Children
( Behavioural Observation Audiometry )
Tests for assessing hearing in children are tailored to different age groups, considering how children respond to sounds at various stages of development.
Birth - 4 months
- Startle reflex: Sudden movement in response to a loud sound.
- Auro-palpebral reflex: Blinking of the eyelids when exposed to loud sounds.
- Arousal reflex: Waking suddenly from sleep due to a loud noise.
5-24 months
- Free field audiometry: The child is placed between two loudspeakers in a sound-treated environment. When the child hears a sound from one speaker, they turn their head towards it.
- Visual reinforcement audiometry:. moving toy is positioned above the loudspeaker. When the child turns their head towards the sound, the toy is briefly activated, encouraging them to respond to sounds.
2 years-5 years
- Play audiometry: The child learns to respond to sounds by engaging in a play activity, such as placing a ball in a bowl.
If the results from these behavioural tests are inconclusive, the child may undergo Otoacoustic Emissions (OAE) followed by Brainstem Evoked Response Audiometry (BERA).
Auditory Steady-State Response (ASSR)
- The Auditory Steady-State Response (ASSR) test is a method used to assess hearing ability, similar to the Brainstem Auditory Evoked Response (BERA) test. However, instead of using quick sound clicks like in BERA, ASSR employs steady-state pure tone signals.
- During the ASSR test, EEG (electroencephalogram) activity is recorded in response to these acoustic signals. When a listener perceives the acoustic signal, their EEG activity will exhibit periodic fluctuations that align with the gradual changes in the sound signal.
- This pattern of EEG activity allows for the determination of specific hearing thresholds across different frequencies.
- ASSR is particularly valuable for measuring hearing in individuals with severe to profound sensorineural hearing loss. It is especially useful in cases where responses may not be detectable using the BERA test.
Speech Audiometry
- Speech audiometry evaluates how well a person can hear and understand spoken words, which is crucial for determining the effectiveness of hearing aids or implants.
- Speech Reception Threshold (SRT) is the level at which a person can correctly identify 50% of two-syllable words. It is often related to the Pure Tone Average (PTA) but can vary among individuals. A large discrepancy may indicate malingering.
- Speech Discrimination Score (SDS) measures the ability to recognize single-syllable words at a volume 30 dB above the SRT. The SDS helps differentiate between cochlear and retrocochlear lesions.
- In cases of cochlear lesions, the percentage of correctly identified words increases with sound levels until it stabilizes. In retrocochlear lesions, the percentage decreases after a certain intensity, known as the Roll Over phenomenon, indicating nerve fatigue.
- The normal range for SDS is 90% to 100%. It is lower in cochlear lesions and significantly reduced in retrocochlear or neural lesions, often disproportionate to the level of hearing loss.
- Cortical deafness, affecting auditory area 41, represents one of the most severe forms of retrocochlear lesions.
Non-Organic Hearing Loss (NOHL)
Non-organic hearing loss refers to a type of hearing loss where there is no physical cause for the impairment. In such cases, the patient may be pretending to be deaf. To identify non-organic hearing loss, several key tests are used:
- Stenger Test: The Stenger test is based on the principle that when two different sound levels are played simultaneously in both ears, only the ear with the louder sound will perceive it. In this test, the patient is blindfolded, and tuning forks or an audiometer are used to assess hearing. When two tuning forks of the same frequency are placed 25 cm apart, the sound should only be heard in the normal ear. If the tuning fork is moved closer to the supposed deaf ear (e.g., 8 cm), the sound should still be heard in the normal ear. However, if the patient is faking deafness in one ear, they will start to hear the sound in the claimed deaf ear when the tuning fork is placed closer to it, even though they should still hear it from the normal ear.
- Stapedial Reflex: The stapedial reflex test evaluates the entire hearing pathway and its connection with the facial nerve. A normal stapedial reflex indicates that the hearing pathway is functioning properly. If a patient claims deafness in one ear, but the stapedial reflex is present in that ear when a loud sound is played, it suggests that the patient may be malingering.
- Speech Audiometry: In speech audiometry, the speech reception threshold should typically be within 10 dB of the pure tone audiometry threshold. A larger difference between these thresholds may indicate malingering. Inconsistencies between repeated pure tone audiometry (PTA) and speech audiometry results can also suggest that the patient is faking their hearing loss.
- BERA (Brainstem Evoked Response Audiometry): BERA is a useful test for evaluating hearing, but it should be considered alongside other tests when assessing non-organic hearing loss.
Distinguishing Between Cochlear and Retrocochlear Pathologies
When a patient is diagnosed with sensorineural (SN) hearing loss through tuning fork tests and confirmed by pure tone audiometry (PTA), various tests can help differentiate between cochlear and retrocochlear pathologies.
Cochlear Pathology
- Recruitment: Abnormal increase in loudness, as seen in the ABLB test.
- SISI Score: Measures the ability to detect short sound increments (1 dB).
- Acoustic Reflex Threshold: Decreased due to recruitment.
- Tone Decay: Indicates nerve fatigue.
- Acoustic Reflex Decay: Also indicative of nerve fatigue.
- BERA (Brainstem Auditory Evoked Response): Shows delayed wave I, while other waves are normal or absent.
- Speech Discrimination Score (SDS): Reduced with the Roll Over Phenomenon absent.
FAQs on Chapter Notes: Physiology of Hearing and Audiology
| 1. What is the function of the middle ear in the hearing mechanism? |  |
| 2. How do tuning fork tests help in assessing hearing loss? | |
| 3. What steps are involved in reading an audiogram? | |
| 4. What is impedance audiometry and its significance in audiology? | |
| 5. What is the acoustic reflex and its role in hearing? | |



