Chapter Notes: Clinical Anatomy of the Pelvis and Reproductive Tract

Introduction
This chapter provides a summary of the key anatomical features of the abdomen and pelvis that are crucial for Obstetric and Gynaecological specialists. A solid understanding of anatomy is necessary to comprehend many of the investigations and treatments we use regularly.
Surface Anatomy
The anterior abdominal wall is divided into four quadrants by drawing horizontal and vertical lines through the umbilicus.
- The area just below the xiphisternum is called the epigastrium, located in the upper abdomen.
- In the lower abdomen, you will find the right and left iliac fossae, as well as the hypogastrium.
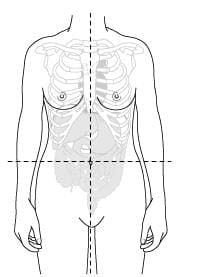 The abdomen can be divided into quadrants.
The abdomen can be divided into quadrants.
Dermatomes
The cutaneous nerve supply to the anterior abdominal wall comes from the anterior rami of the lower thoracic and lumbar vertebrae. The dermatomes of important structures on the anterior abdominal wall are as follows:
- T7 - xiphisternum
- T10 - umbilicus
- L1 - symphysis pubis
The blood supply to the anterior abdominal wall is provided by the superior epigastric vessels, which are branches of the internal thoracic artery, and the inferior epigastric vessels, which are branches of the external iliac artery.
During laparoscopy, the inferior epigastric vessels can be observed between the peritoneum and the rectus muscle on the anterior abdominal wall. These vessels originate from approximately two-thirds of the way along the inguinal ligament, closer to the symphysis pubis, and travel superiorly.
It is crucial to exercise caution when using accessory trocars during laparoscopy to avoid damaging the inferior epigastric vessels. Additionally, these vessels should be identified when performing a Maylard incision on the abdominal wall.
The Anterior Abdominal Wall
- Beneath the skin and fat of the outer anterior abdominal wall lies a layer composed of various muscles, including the rectus abdominus, external and internal oblique, and transversalis muscles.
- At the center, where these muscles converge, the linea alba is formed.
- In some individuals, particularly women, there may be a pyramidalis muscle, which originates from the front of the pubis and attaches to the linea alba.
- The arrangement of these muscles can differ based on the location of any surgical incision.
The Umbilicus: Anatomy and Clinical Significance
- The umbilicus, commonly known as the belly button, is essentially a scar resulting from the cutting of the umbilical cord. It is situated along the linea alba, a fibrous structure that runs down the midline of the abdomen. The exact location of the umbilicus can differ depending on the patient's level of obesity. However, the base of the umbilicus is consistently the thinnest part of the front abdominal wall. This makes it the most common site for inserting the primary port during laparoscopic surgeries.
- Beneath the umbilicus lies the urachus, which is a remnant of the allantois from fetal development. The urachus connects the top of the bladder to the umbilicus. In some newborns, this connection can remain open. During early embryonic development, the vitelline duct also passes through the umbilicus from the developing midgut. Although this duct is usually cut long before birth, a small remnant of it can be found in about 2% of the population as a condition known as Meckel's diverticulum.
- In most slender women, the aorta divides into the common iliac arteries about 1 to 2 centimeters below the umbilicus. Just below this point, the common iliac veins join to form the inferior vena cava. These vascular structures can pose a potential risk during laparoscopic procedures involving port insertion at the umbilicus.
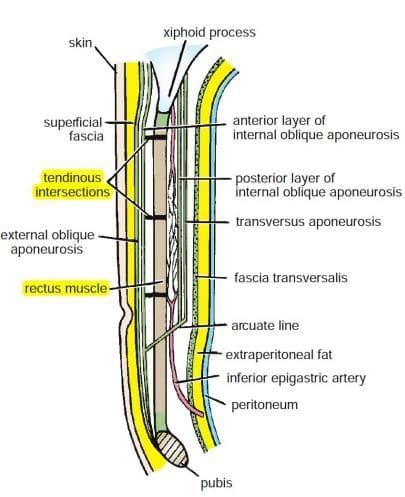
Layers of the Anterior Abdominal Wall
- Rectus Muscle: This is a long, flat muscle that extends along the front of the abdomen. It plays a crucial role in flexing the spine and maintaining posture.
- External Oblique Aponeurosis: The external oblique muscle is located on the side and front of the abdomen. Its aponeurosis (a type of connective tissue) helps in forming the abdominal wall and provides support.
- Tendinous Intersections: These are horizontal fibrous bands that divide the rectus abdominis muscle into sections. They contribute to the muscle's strength and definition.
- Superficial Fascia: This is a layer of connective tissue found just beneath the skin. It contains fat and helps insulate the body, as well as providing a pathway for blood vessels and nerves.
- Skin: The outermost layer of the body, which protects underlying tissues and organs, regulates temperature, and provides sensory information.
- Fascia Transversalis: This is a thin layer of connective tissue that lies beneath the abdominal muscles and above the peritoneum. It helps in containing abdominal organs and provides structural support.
- Extraperitoneal Fat: This layer of fat is located between the fascia transversalis and the peritoneum. It acts as a cushion for abdominal organs and provides insulation.
- Peritoneum:. thin membrane that lines the abdominal cavity and covers the abdominal organs. It plays a role in protecting organs and allowing them to move smoothly against each other.
- Pubis: The pubic bone is part of the pelvic girdle and provides support for the lower body. It also serves as an attachment point for various muscles.
- Transversus Aponeurosis: This is a layer of connective tissue associated with the transversus abdominis muscle, which is located deep in the abdomen. The aponeurosis helps in stabilizing the abdominal wall.
- Posterior Layer of Internal Oblique Aponeurosis: The internal oblique muscle is located beneath the external oblique and helps in rotating and bending the trunk. The posterior layer of its aponeurosis contributes to the strength of the abdominal wall.
- Anterior Layer of Internal Oblique Aponeurosis: This is the front part of the internal oblique muscle's aponeurosis. It also aids in strengthening the abdominal wall and supporting internal organs.
Epithelium of the Genital Tract
- The vulva, vagina, and perineal regions of the anterior abdominal wall are covered by squamous epithelium.
- The endocervix and uterine cavity are lined with columnar epithelium, while the squamocolumnar junction is usually found at the ectocervix in women of reproductive age.
- This junction is important because it is the site where cervical intraepithelial neoplasia (CIN) and potentially cervical cancer can arise.
- The lining of the bladder consists of transitional epithelium, which has the ability to change into columnar epithelium.
- The anal verge is covered by squamous epithelium, which transitions to columnar epithelium just inside the anus and extending into the rectum.
- The genital tract provides a continuous passage from the vagina through the uterus and into the fallopian tubes, leading into the peritoneal cavity.
- This pathway is essential for the movement of sperm during fertilization.
- However, it also poses a risk for the transfer of pathogenic organisms, which can result in ascending infections.
Understanding the Peritoneum
- The peritoneum is a delicate membrane that lines the interior of the abdominal and pelvic cavities.
- In simpler terms, the peritoneum acts as a protective layer covering the organs within these cavities, including the bladder, uterus, and rectum.
- This membrane is not continuous; it is interrupted by the fallopian tubes and the ovaries.
- At the rear, the rectum passes through the peritoneum, establishing a connection with the sigmoid colon.
- The space located between the back of the uterus, its supporting ligaments, and the rectum is known as the Pouch of Douglas.
- This area holds particular importance in gynecology because it tends to be a site where fluid accumulates due to gravitational forces.
- As a result, the Pouch of Douglas is often associated with the presence of blood in cases of ectopic pregnancies, pus in instances of infections, and various conditions related to endometriosis.
- One theory regarding endometriosis, known as Samson's theory, suggests that this condition may arise from retrograde menstruation, where menstrual fluid flows backward into the pelvic cavity.
Vulva
- The vulva refers to the area surrounding the perineum and comprises the following parts:
- Mons pubis: The fatty tissue covering the pubic bone.
- Labia majora: The outer folds of skin that protect the inner structures.
- Labia minora: The inner folds of skin located within the labia majora.
- The openings of the vagina and urethra.
- The labia majora consist of skin with underlying fat and serve to outline and protect the vagina.
- The labia minora are situated closer to the vaginal opening and are composed of tissue rich in blood vessels, which can become engorged during sexual arousal.
- At the front, the labia minora connect to form the prepuce of the clitoris, and at the back, they create the forchette.
- The hymen is a fold of tissue at the entrance of the vagina. In some virgins, it may have a small opening, while in sexually active women, it is often irregular.
- On either side of the vaginal opening (introitus) are the ducts of the vestibular glands, known as Bartholin's glands, which provide lubrication during sexual intercourse.
- The blood supply to the vulva comes from the pudendal artery.
- Lymphatic drainage occurs through the inguinal lymph nodes.
- The main nerve supply is from the pudendal nerve and pelvic plexus, with contributions from the perineal nerves and the posterior cutaneous nerve of the thigh in the posterior area.
The Clitoris
- The clitoris is an organ with distinct functions and structures. It shares some similarities with the male penis and consists of three masses of erectile tissue.
- The clitoris is made up of three masses of erectile tissue, similar to the male penis.
- The bulb of the vestibule connects to the urogenital diaphragm and splits into two parts because of the vagina's presence.
- The right and left crura become the corpora cavernosa and are covered by the ischiocavernosus muscles.
Bony Pelvis
The bony pelvis consists of two hip bones, the ilium and ischium, which are joined at the back by the sacrum and at the front by the symphysis pubis. The coccyx is situated beneath the sacrum.
- A line from the sacral promontory to the top of the symphysis pubis indicates the pelvic inlet.
- Another line from the tip of S5 to the bottom of the symphysis pubis marks the pelvic outlet.
Clinical Significance
- The ischial spine is important because it can be felt vaginally and serves as a landmark for measuring progress during labour.
- It is also the attachment point for the sacrospinous ligament, which connects the ischial spine to the lower part of the sacrum.
- The sacrospinous ligament, along with the sacrotuberous ligament and the bony pelvis, forms the boundaries of the greater sciatic foramen and the lesser sciatic foramen.
- The greater sciatic foramen is where the sciatic nerve passes, and the lesser sciatic foramen is where the pudendal nerve enters the pelvis.
The sacrum and ilium are joined by the sacroiliac joint, a robust synovial joint reinforced by the posterior and interosseous sacroiliac ligaments. The symphysis pubis is a cartilaginous joint with a fibrocartilaginous disc separating the two bones, which are tightly bound by supporting ligaments. This joint is meant to have minimal movement.
Pelvic Floor
- The pelvic floor is made up of muscles and ligaments that create a strong support system for the organs in the lower abdomen.
- This area includes important structures such as the obturator internus muscle, which is located on the inside of the ischial bone and helps form a wall with the pubis to support the pelvic floor.
- The pelvic floor muscles form a sling-like structure that allows the urethra, vagina, and anal canal to pass through.
- Behind the vagina, these muscles create the perineal body, which is an important support structure.
- The puborectalis muscle is part of this group and wraps around the junction of the rectum and anus. Other muscles, such as the pubococcygeus, contribute to the formation of the anococcygeal body in the midline.
- Together, these muscles are often called the pelvic diaphragm or levator ani, and they play a crucial role in supporting the pelvic organs, keeping them in place, and resisting increased pressure during activities like coughing or straining.
- The nerve supply for these muscles comes from the fourth sacral nerve and the pudendal nerve.
- Ischiopubic ramus
- Ischiocavernous muscle
- Bulbocavernous muscle
- Deep layer of superficial fascia (Colles fascia)
- Superficial perineal compartment
- Ischial tuberosity
- Sacrotuberous ligament
- Levator ani muscle
- External anal sphincter
- Gluteus maximus muscle
- Coccyx
- Suspensory ligament of clitoris
- Clitoris
- Vestibular bulb
- Inferior fascia of urogenital diaphragm
- Bartholin's gland
- Superficial transverse perineal muscle
- Central point of perineum
- Fascia of obturator internus
- Ischiorectal fossa
- Anococcygeal body
Pelvic organs
- The vagina is a flexible and muscular tube that extends from its entrance to the cervix.
- It goes through the pelvic floor and is supported by resting against the back surface of the pelvic floor.
- The vagina is approximately 8 cm long, with its front and back walls touching each other.
- Sometimes, anatomical drawings may incorrectly show the vagina as an open tube with an empty space inside.
- In reality, a healthy vagina is not expanded and usually does not contain air.
- The upper part of the vagina connects to the uterine cervix.
- The areas of the vagina next to the cervix are called the fornices, which are designated as anterior, posterior, right, or left.
- The vaginal wall consists of outer and inner layers of muscles that blend together.
- The epithelium of the vaginal wall does not have glands but contains a significant amount of glycogen, especially in premenopausal women.
- The normal bacteria present in the vagina, known as Lactobacillus, breaks down this glycogen, leading to the formation of an acidic environment.
Uterus
- Size and Structure. The uterus is roughly the size and shape of a pear, with a central cavity and thick muscular walls.
- Layers of the Uterus. The uterus has several important layers:
- Serosal Surface. This is the outermost layer, covered by the peritoneum.
- Myometrium. Beneath the serosal surface, this layer is made up of smooth muscle and connective tissue. It has three sub-layers:
- External Layer
- Intermediate Layer
- Internal Layer
- Endometrium. This is the mucous membrane lining the uterus cavity, located above the myometrium.
- Fibroids. When fibroids are removed, these layers are preserved. The three muscle layers run in different directions, which aids in blood flow during contractions. This is important for menstrual blood loss and controlling postpartum bleeding.
- Uterine Parts. The uterus consists of several parts:
- Fundus. The top part of the uterus.
- Body. The main part of the uterus.
- Isthmus (Internal Os). The narrow part leading to the cervix.
- Cervix (External Os). The lower part of the uterus opening into the vagina.
- Cervical Structure. The cervix has a cylindrical shape and is muscular at the top. It changes to fibrous connective tissue where it connects to the vagina.
- Cervical Lining. The cervix is lined with columnar epithelium that produces alkaline mucus. This mucus helps balance the acidity of the vagina.
- Uterine Positioning. The uterus can be positioned in different ways:
- Anteflexed. When the uterine body tilts forward.
- Retroflexed. When it tilts backward.
- Anteverted. The entire uterus tilts forward in relation to the vagina.
- Retroverted. The entire uterus tilts backward in relation to the vagina.
- Support Structures. The uterus is supported by pelvic floor muscles and three main connective tissue ligaments:
- Pubocervical Ligaments. These ligaments extend from the cervix to the pubis.
- Cardinal Ligaments. They run from the cervix and upper vagina to the pelvic side walls.
- Uterosacral Ligaments. These connect the cervix and upper vagina to the sacrum.
- Uterosacral Ligaments. These ligaments are visible behind the uterus in the Pouch of Douglas and are common sites for endometriosis.
- Blood Supply. The main blood supply to the uterus comes from the uterine artery, which branches from the internal iliac artery. There is also a connection through the ovarian ligament, supplied by the ovarian artery.
- Round Ligament. This ligament is a remnant of the gubernaculum. It extends from the uterus to the pelvic side wall, through the inguinal canal, and into the labia majora. The round ligament helps keep the uterus in an anteverted position, although it can stretch during pregnancy. During a hysterectomy, it is usually one of the first structures to be cut, allowing access to the broad ligament covering the uterus.
Fallopian Tubes
- The fallopian tubes are narrow tubes responsible for transporting either the ovum (egg) or sperm between the ovary and the uterine cavity.
- These tubes are made up of several sections: the cornu and interstitial portion, which are located within the uterine wall, followed by the isthmus, infundibulum, and the fimbrial ends.
- The interior of the fallopian tubes is lined with columnar epithelium and cilia. These structures, along with the peristaltic action of the surrounding smooth muscle, help move the fertilised ovum towards the uterine cavity.
- The blood supply to the fallopian tubes is provided by the uterine and ovarian arteries, as well as branches from the abdominal aorta. This blood supply reaches the tubes through the mesosalpinx, which is covered by peritoneum.
Ovaries
- The size of the ovaries varies with age and function. They typically measure about 2 × 4 cm², are oriented vertically, and are attached to the broad ligament by the mesovarium .
- The ovaries are held in place by the ovarian ligament (which attaches medially to the uterus) and the infundibulopelvic ligament, responsible for carrying blood from the aorta.
- Venous drainage occurs through the ovarian veins, which drain into the inferior vena cava on the right side and the left renal vein on the left side.
- The aortic nerve plexus follows the ovary as it descends from around the level of the first lumbar vertebra.
- The lateral pelvic side wall is covered by peritoneum, which folds to create the ovarian fossa .
- Pathological adhesions around the ovary can lead to complications.
Fixed in the ovarian fossa, this can lead to cyclical pain or dyspareunia. The ovary is not covered by peritoneum; instead, it has a thin membranous capsule called the tunica albuginea, covered by germinal epithelium.
Urinary Bladder
- The urinary bladder is situated directly behind the pubic bone and in front of the uterine cervix and upper vagina.
- It features a robust muscular wall composed of three layers of fibers, collectively known as the detrusor muscles.
- The trigone is the only smooth region of the bladder, firmly attached to the underlying muscles.
- The openings for the ureters are located at the top of the trigone, while the urethra is situated at the bottom.
- An interureteric ridge is often visible horizontally between the ureters during cystoscopy, serving as a helpful orientation guide.
- The bladder is highly distensible, capable of expanding while maintaining constant pressure.
- The bladder receives blood supply from the superior and inferior vesical arteries, which branch from the internal iliac artery.
- Nerve supply to the bladder is provided by the inferior hypogastric plexus.
- Sympathetic nerves originate from the first and second lumbar ganglia, while the parasympathetic supply comes from the splanchnic nerves of the second, third, and fourth sacral nerves.
Urethra in Females
- Length and Structure: The female urethra is approximately 4 cm long. It starts at the internal opening of the bladder and extends through the pelvic floor to the vestibule.
- Tissue Composition: Near the external opening of the urethra, the tissue is squamous. About two-thirds of the way towards the bladder, this tissue changes to transitional epithelium. The deeper layers of the urethra consist of muscular tissue, which helps maintain muscle tone in the urethra.
- Sphincter Mechanisms: While there are no anatomical sphincters in the female urethra, the muscle fibers at the internal opening of the bladder act like an internal sphincter. The pelvic floor functions as a voluntary external sphincter.
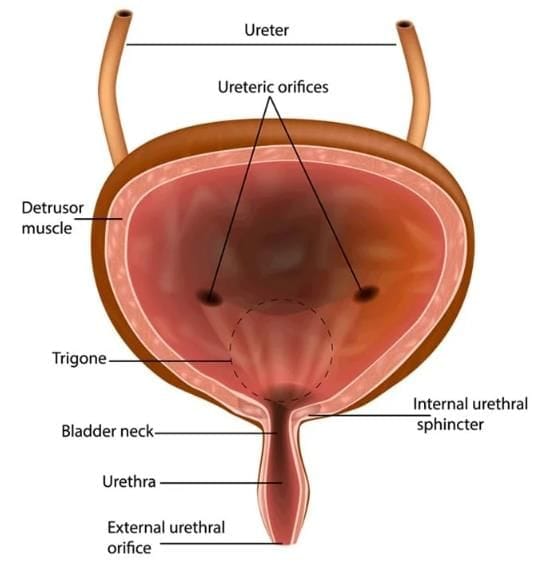 The bladder
The bladder
Ureters
- The ureters are muscular tubes that are approximately 30 cm long, serving as the conduit between the kidneys and the bladder.
- They stretch from the renal hilum to the trigone of the bladder, entering the pelvic region by crossing over the common iliac bifurcation at the pelvic brim.
- The ureters run along the side wall of the pelvis before advancing forward and inward, passing beneath the uterine artery, which branches from the internal iliac artery, and into the base of the bladder.
- They are located in proximity to the ovarian artery and vein, with the possibility of adhering to these vessels or the ovary in certain medical conditions.
- Given their location near the uterine artery, there is a rare risk of them being inadvertently clamped or cut during a hysterectomy procedure.
- The lining of the ureters consists of transitional epithelium, and their blood supply varies along their length, making it essential to carefully preserve small blood vessels during surgical dissection.
Rectum
- The rectum is approximately 12 cm long and begins at the level of the S3 vertebra, continuing from the sigmoid colon.
- At its lower end, the puborectalis muscle forms a sling around the rectum where it meets the anal canal.
- Although anatomical illustrations often depict the rectum as dilated, its appearance can differ between cadavers and living individuals. In healthy patients, the rectum is usually empty, allowing other pelvic structures to rest on the pelvic floor.
- The mucosal lining of the rectum is made up of columnar tissue, and it is surrounded by smooth muscle fibers arranged in an inner circular and outer longitudinal pattern. The outer surface of the rectum is covered by peritoneum.
- Blood supply to the rectum is primarily from the superior rectal artery, a branch of the inferior mesenteric artery. The middle and inferior rectal arteries arise from the posterior division of the internal iliac artery.
- The nerve supply to the rectum comes from the inferior hypogastric plexus, which makes the rectum sensitive to stretching.
Conclusion
- A solid grasp of anatomy is crucial for various gynaecological diagnoses and surgical procedures.
- Many clinicians do not fully understand pelvic anatomy until they start performing surgeries.
- Once they gain this understanding, they often neglect to review anatomical textbooks.
- The emergence of advanced pelvic floor surgeries, particularly minimal access surgery, has changed the skill set required for gynaecological surgeons.
- This change necessitates a more profound understanding of practical anatomical knowledge.
FAQs on Chapter Notes: Clinical Anatomy of the Pelvis and Reproductive Tract
| 1. What is the anatomical significance of the umbilicus in relation to the reproductive tract? |  |
| 2. How does the epithelium of the genital tract differ from that of other parts of the body? | |
| 3. What role does the peritoneum play in the pelvic cavity? | |
| 4. What are the primary functions of the uterus in the reproductive system? | |
| 5. How do the fallopian tubes contribute to fertility? | |



