Chapter Notes: Abdomen - 2


Nerve Supply
Genitofemoral Nerve
- Arises from the L1 and L2 ventral rami, travels diagonally forward through the psoas major muscle, and emerges on its anterior surface near the medial border at the level of the third or fourth lumbar vertebra.
- Descends under the peritoneum on the psoas major, crosses behind the ureter at an angle, and splits into genital and femoral branches.
- The genital branch enters the inguinal canal via the deep ring, travels with the spermatic cord or round ligament, and exits through the superficial inguinal ring, typically dorsal to the cord or ligament. It innervates the cremaster muscle and the skin of the external genitalia (scrotum, mons pubis, labia majora). Similar to the ilioinguinal nerve, it is prone to injury during inguinal surgery (open or laparoscopic), which may cause neuralgic pain.
- The femoral branch passes behind the inguinal ligament (rarely through it), enters the femoral sheath lateral to the femoral artery, pierces the anterior femoral sheath and fascia lata, and supplies the skin of the upper femoral triangle and the anteromedial thigh.
Autonomic innervation of abdominal viscera (Splanchnic nerves)
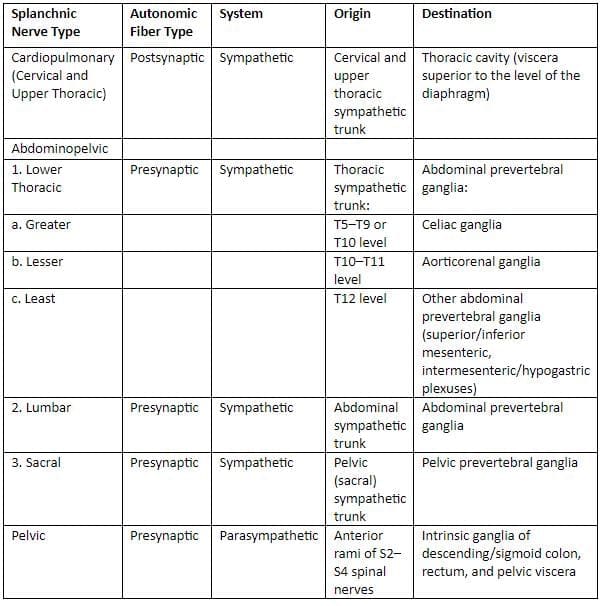
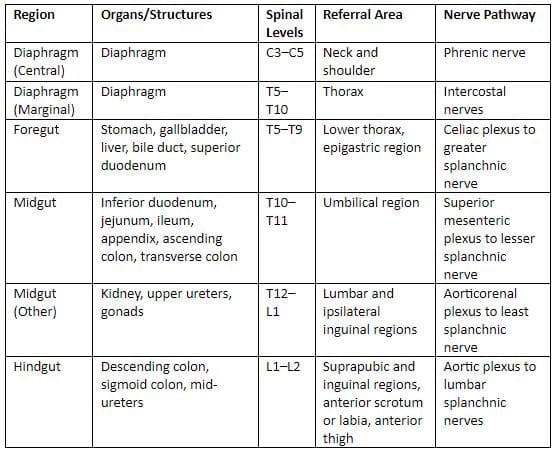
Pain referral from abdominal viscera
Pain referral from pelvic viscera
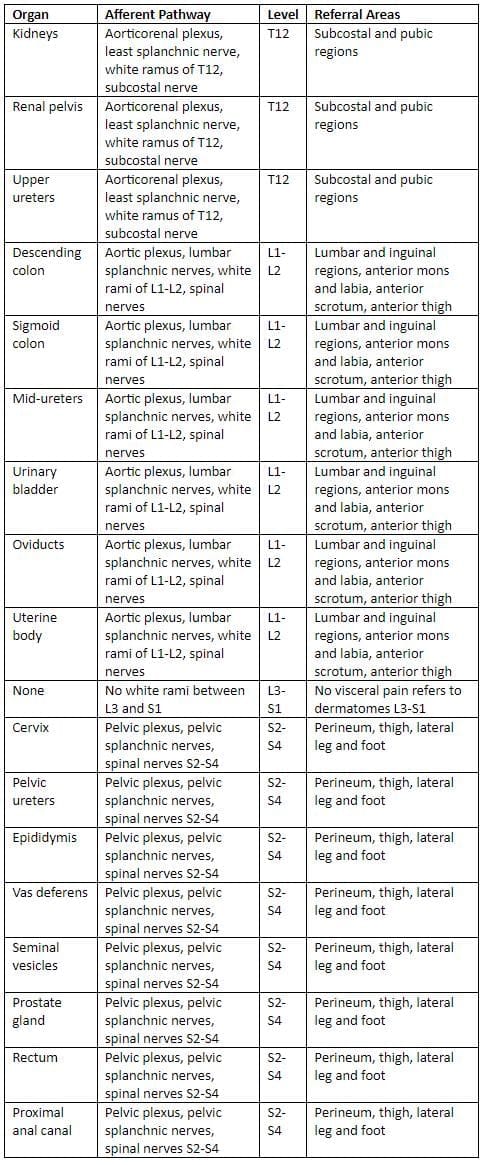
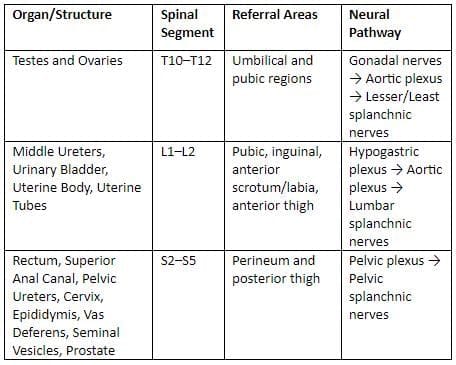 Pelvic visceral afferent innervation
Pelvic visceral afferent innervation
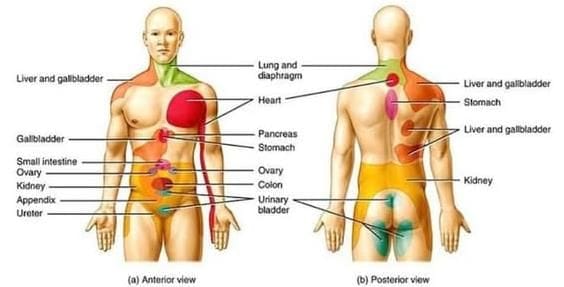 Referred pain of various on the body surface.
Referred pain of various on the body surface.
Applied Anatomy
- Visceral Pain: Visceral organs do not perceive sensations like cutting, crushing, or burning. However, they can experience pain when they are overstretched, when there is a spasm of smooth muscles, or when blood flow is restricted. This type of pain is often felt as if it is originating from the skin that shares the same nerve supply, a phenomenon known as referred pain.
- Lumbar Sympathectomy: Lumbar sympathectomy is a surgical procedure aimed at addressing blood flow issues in the lower limb, such as in conditions like Buerger's disease. During this surgery, the second, third, and fourth lumbar ganglia, along with a portion of the sympathetic chain, are excised. This intervention enhances blood circulation in the lower limb, resulting in the skin of the affected area becoming warm, pink, and dry, which is a common postoperative outcome. The first lumbar ganglion is preserved during this procedure because it plays a crucial role in ejaculation by helping to maintain the closure of the bladder sphincter during this process.
- Consequences of Removing the First Lumbar Sympathetic Ganglion: The removal of the first lumbar sympathetic ganglion can lead to a condition known as dry coitus. This occurs due to the alterations in bodily functions following the surgical intervention.
Vasculature - Arteries
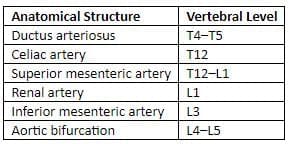
Key anatomical reference points
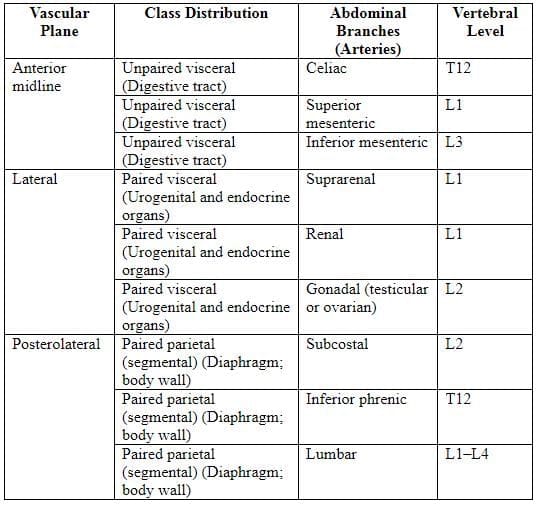
Branches of abdominal aorta
 The abdominal aorta starts at the T12 vertebra, passing through the aortic hiatus, and descends to bifurcate at the L4 vertebra, slightly left of the midline. The inferior vena cava (IVC) is associated with the L5 vertebra.
The abdominal aorta starts at the T12 vertebra, passing through the aortic hiatus, and descends to bifurcate at the L4 vertebra, slightly left of the midline. The inferior vena cava (IVC) is associated with the L5 vertebra.
Abdominal Aorta
Major Branches
The celiac trunk is located at the T12 vertebral level and supplies organs that develop from the foregut, including the intra-abdominal part of the esophagus, stomach, upper part of the duodenum, liver, gallbladder, and pancreas. It branches into the left gastric artery, splenic artery, and common hepatic artery.
The superior mesenteric artery is situated at the L1 vertebral level and supplies organs from the midgut, such as the lower part of the duodenum, jejunum, ileum, cecum, appendix, ascending colon, and proximal two-thirds of the transverse colon.
- Renal arteries supply the kidneys.
- Gonadal arteries supply the testes or ovary.
The inferior mesenteric artery is located at the L3 vertebral level and supplies organs from the hindgut, including the distal one-third of the transverse colon, descending colon, sigmoid colon, and upper part of the rectum.
The common iliac arteries are the final branches of the abdominal aorta.
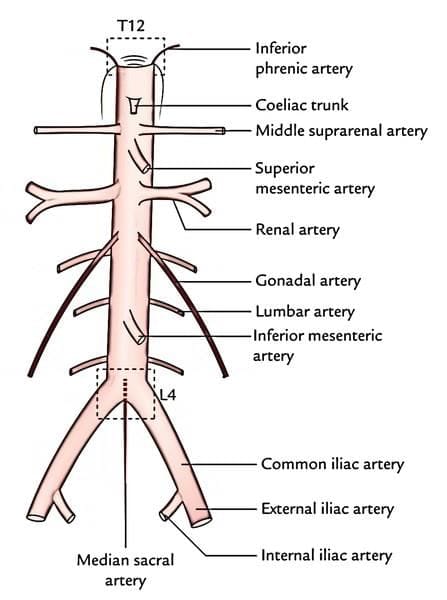 Course and branches of the abdominal aorta
Course and branches of the abdominal aorta
Collateral Circulation
The abdominal blood vessels exhibit robust collateral circulation. In cases of blockage between the superior mesenteric artery at L1 and the inferior mesenteric artery at L3, blood can reroute through two pathways:
- The first pathway involves the middle colic artery (a branch of the superior mesenteric artery) connecting with the left colic artery (a branch of the inferior mesenteric artery).
- The second pathway utilizes the marginal artery.
Arterial Supply to Abdominal Foregut Derivatives
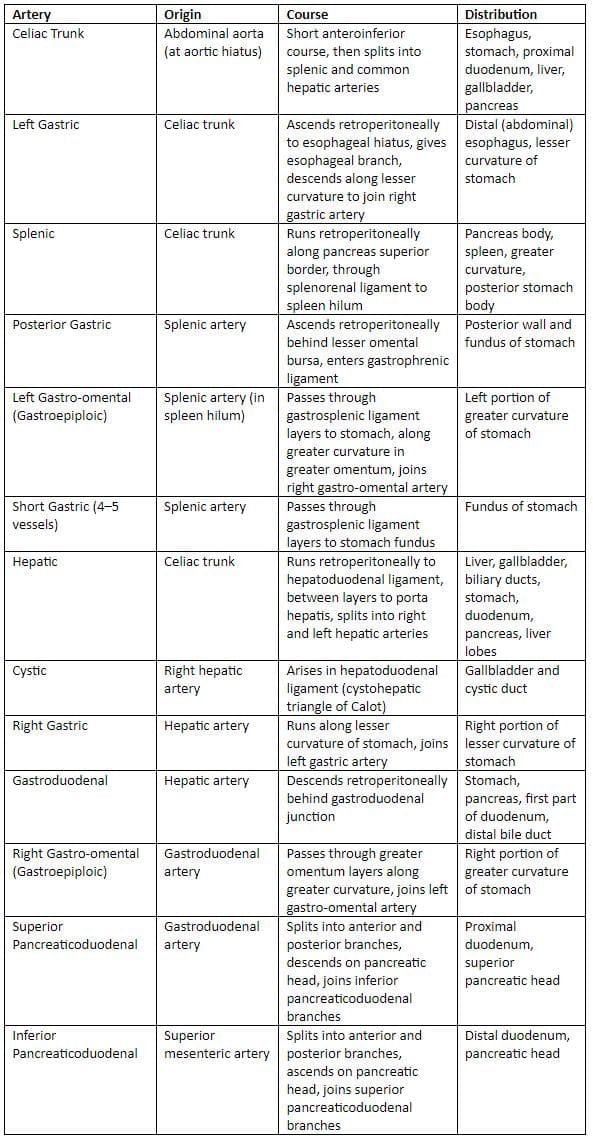
Note: The hepatic artery is divided into the common hepatic artery (from origin to gastroduodenal artery origin) and the hepatic artery proper (remainder of the vessel).
Venous Drainage of the Abdomen
Inferior Vena Cava (IVC)
The IVC is formed when the right and left common iliac veins merge at the level of the L5 vertebra. It is responsible for carrying blood from below the diaphragm, including blood from the gastrointestinal tract after it has passed through the liver, to the right atrium of the heart.
During surgeries to repair a herniated intervertebral disc, the IVC can be at risk. The section of the IVC above the kidneys (suprarenal) should never be tied off due to the high risk of mortality. The section below the kidneys (infrarenal) can be tied off, but there is a 50% chance of death associated with this procedure.
The right gonadal vein drains directly into the IVC, while the left gonadal vein connects to the left renal vein. This distinction is important for females, as a right-sided hydronephrosis may indicate a blockage in the right ovarian vein, which compresses the ureter as it drains into the IVC. In males, a left-sided testicular varicocele may suggest a blockage of the left testicular and/or renal vein, possibly due to kidney cancer.
If the IVC is obstructed by a malignant retroperitoneal tumour or a large blood clot (thrombus), alternative routes for blood return include:
- Azygos vein → Superior vena cava (SVC) → right atrium
- Lumbar veins → external and internal vertebral venous plexuses → cranial dural sinuses → internal jugular vein → right atrium
The left inferior phrenic, suprarenal, and gonadal veins do not drain into the inferior vena cava.
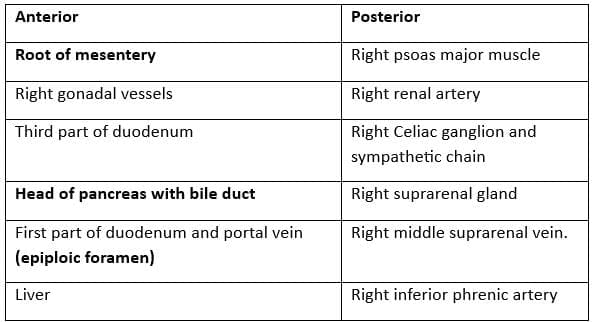
Relations of the Inferior Vena Cava (IVC)
Portal Vein
- The superior mesenteric vein merges with the splenic vein to create the portal vein behind the neck of the pancreas, at the level of the L1/2 intervertebral disc, which is also known as the transpyloric plane.
- In adults, the portal vein measures approximately 8 cm in length. It ascends obliquely to the right, positioned behind the first part of the duodenum, the common bile duct, and the gastroduodenal artery. At this stage, it is located directly anterior to the inferior vena cava.
- The portal vein enters the lesser omentum at its right border, ascending anterior to the epiploic foramen. It reaches the right end of the porta hepatis, where it bifurcates into right and left main branches. These branches accompany the corresponding branches of the hepatic artery as they enter the liver.
- Within the lesser omentum, the portal vein is situated behind both the common bile duct and the hepatic artery.
- The primary extrahepatic tributaries of the portal vein include the left gastric (coronary) vein and the posterior superior pancreaticoduodenal vein. Inside the liver, the left branch of the portal vein receives the obliterated umbilical vein through the ligamentum teres, which connects to its vertical portion.
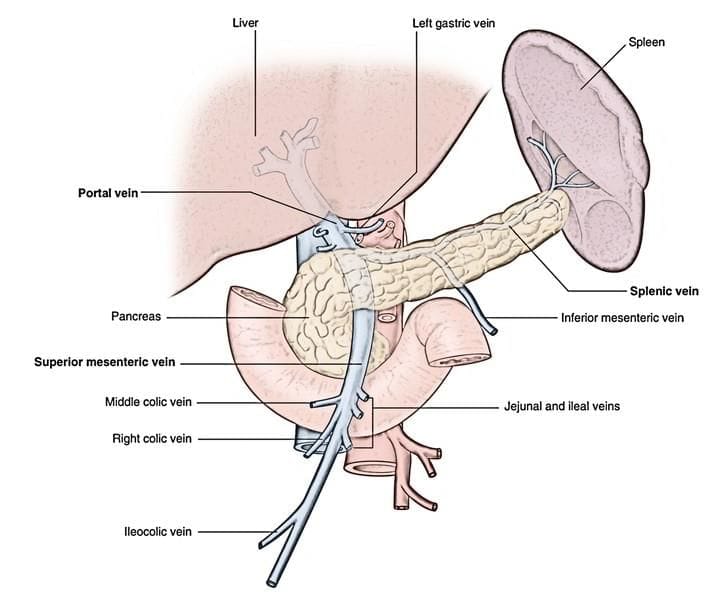 Portal vein formation
Portal vein formation
Hepatic Portal System
The term "portal" generally describes a vein situated between two capillary beds, following the pattern: capillary bed → vein → capillary bed. The hepatic portal system specifically includes the vascular pathway: capillaries of the gastrointestinal (GI) tract → portal vein → hepatic sinusoids. The portal vein forms behind the pancreas neck through the convergence of the splenic vein and superior mesenteric vein, with the inferior mesenteric vein typically joining the splenic vein. Blood in the portal vein carries nutrient-rich blood from the GI tract and waste products from red blood cell breakdown in the spleen.
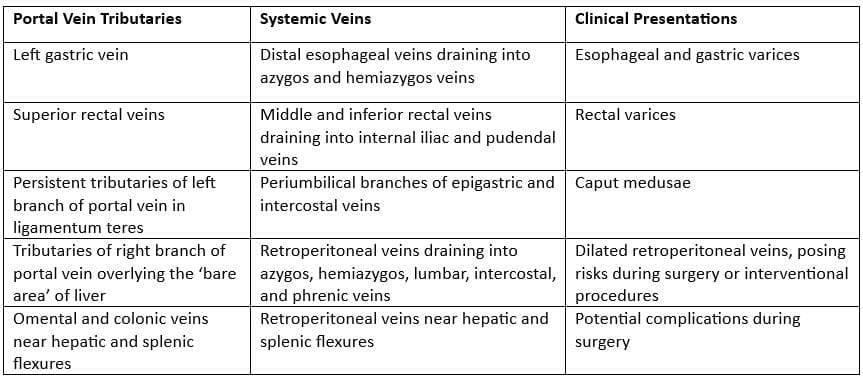
The hepatic portal system features robust collateral circulation. In cases of reduced liver blood flow, such as portal hypertension from liver cirrhosis, portal blood diverts through three collateral routes:
- Esophagus: The left gastric vein (portal system) connects with the esophageal vein (inferior vena cava [IVC] system), forming esophageal varices.
- Umbilicus: The paraumbilical vein (portal system) links with the superficial and inferior epigastric veins (IVC system), creating caput medusae.
- Rectum: The superior rectal vein (portal system) anastomoses with the middle and inferior rectal veins (IVC system), leading to anorectal varices.
Clinical relevance: Portal hypertension. This condition causes blood in the portal vein to reverse flow, entering the IVC to return to the heart. Key sites of portal-IVC anastomosis are the esophagus, umbilicus, and rectum. Symptoms include vomiting large amounts of blood, abdominal swelling from ascites, and splenomegaly. Causes include alcoholism, liver cirrhosis, and schistosomiasis. An image depicts an elderly man with portal hypertension showing caput medusae.
Common sites of porto-systemic anastomoses in portal hypertension and associated clinical implications
 Lymphatics
Lymphatics
- Aortic lymph nodes, located on the posterior abdominal wall, are categorized into preaortic, lateral aortic, and retroaortic groups.
- Preaortic lymph nodes, situated in front of the abdominal aorta, are subdivided into celiac, superior mesenteric, and inferior mesenteric nodes. They receive lymph from intermediate nodes, and their efferent vessels form the intestinal trunks that drain into the cisterna chyli.
- Lateral aortic lymph nodes, positioned on both sides of the abdominal aorta, primarily receive lymph from the common iliac lymph nodes. Their efferent vessels form the lumbar trunks, which drain into the cisterna chyli, with some efferents connecting to the preaortic or retroaortic nodes.
- Retroaortic lymph nodes are considered an extension of the lateral aortic lymph nodes.
- Lymph from the pelvic region flows as follows: sacral, external iliac, and internal iliac nodes → common iliac nodes → lateral aortic nodes → lumbar trunks → cisterna chyli. Lateral sacral nodes drain into the common iliac nodes.
- Paracolic lymph nodes (associated with the midgut and hindgut) drain into the superior or inferior mesenteric lymph nodes, which are part of the preaortic group. Their efferent vessels form the intestinal trunks, which lead to the cisterna chyli.
Inguinal Region and External Genitalia
Inguinal Region
- The inguinal region refers to a vulnerable area in the front wall of the abdomen. This vulnerability arises from the developmental processes where, in males, the testes descend, and in females, the round ligament of the uterus is formed.
- The deep inguinal ring is an opening found in the transversalis fascia. This ring serves as an entrance into the inguinal canal and acts as the internal layer for the structures that pass through it.
- The superficial inguinal ring is a gap located in the aponeurosis of the external oblique muscle. This gap is situated to the side of the pubic tubercle.
- The inguinal canal is an oblique passage that extends from the deep inguinal ring to the superficial inguinal ring.
- In males, this canal carries the spermatic cord, while in females, it carries the round ligament. It is important to note that both structures are not present simultaneously in the canal.
- Additionally, the inguinal canal also accommodates blood vessels, lymphatic vessels, and the genital branch of the genitofemoral nerve in both males and females.
Deep Inguinal Ring
- The deep inguinal ring is an oval-shaped opening located in the transversalis fascia.
- It is positioned approximately halfway between the anterior superior iliac spine and the pubic symphysis, about 1 cm above the inguinal ligament.
- This opening is found above the lower arched margin of the transversus abdominis muscle and is in close proximity to the interfoveolar ligament.
- Medially to the deep inguinal ring are the inferior epigastric vessels.
- These vessels run along the transversalis fascia, moving obliquely behind the conjoint tendon before entering the rectus sheath.
- The length of the inguinal canal is approximately 4 cm, according to the National Board of Examinations in Medical Sciences (2013).
Inguinal Ligament (Poupart Ligament)
- The inguinal ligament is the curved lower edge of the aponeurosis of the external oblique muscle.
- It stretches from the anterior superior iliac spine to the pubic tubercle.
- This ligament forms the floor of the inguinal canal.
- Modifications of the external oblique muscle include the inguinal ligament, lacunar ligament, and pectineal (Cooper's) ligament.
Reflected Inguinal Ligament
- The reflected inguinal ligament runs upwards over the conjoint tendon.
- It ends at the linea alba.
Falx Inguinalis (Conjoint Tendon)
- The falx inguinalis is formed from the connective tissues of the internal oblique and transverse abdominal muscles.
- It attaches to the pubic tubercle and crest.
- This structure descends behind the superficial inguinal ring.
- It plays a role in strengthening the posterior wall of the medial half of the inguinal canal.
Lacunar Ligament (Gimbernat Ligament)
- The lacunar ligament is a triangular extension of the inguinal ligament.
- It runs from the external oblique aponeurosis to the pectineal line of the pubis.
- This ligament forms the inner border of the femoral ring and the base of the inguinal canal.
Pectineal (Cooper) Ligament
- The pectineal ligament is a strong fibrous band that extends sideways from the lacunar ligament along the pectineal line of the pubis.
The Scrotum
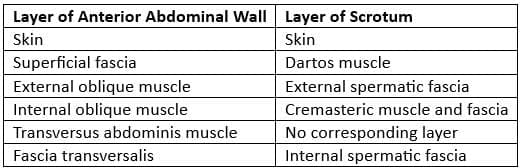
The scrotum is an extension of the lower abdominal wall, with its layers extending into the scrotal region to envelop the spermatic cord and testes.
Comparison between the layers of the anterior abdominal wall and the scrotum
 Inguinal Canal
Inguinal Canal
The inguinal canal is a passage in the lower part of the anterior abdominal wall. It is located just above the middle section of the inguinal ligament and is about 3.75 cm long, although this can vary among individuals. The canal runs from the deep inguinal ring to the superficial inguinal ring.
Boundaries of the Inguinal Canal:
- Front Wall: Made up of skin, superficial fascia, and the external oblique aponeurosis, with contributions from the internal oblique muscle in the outer third.
- Back Wall: Consists of fascia transversalis, extraperitoneal tissue, and parietal peritoneum, with the conjoint tendon in the medial two-thirds.
- Roof: Formed by the arched fibres of the internal oblique and transversus abdominis muscles.
- Floor: Composed of the grooved upper surface of the inguinal ligament, with the lacunar ligament at the inner end.
Openings:
- Triangular aperture in the external oblique aponeurosis above and lateral to the pubic crest.
- Oval aperture in the fascia transversalis, located 1.25 cm above the midinguinal point.
Contents of the Inguinal Canal
- In males. Spermatic cordIn females. Round ligament of the uterus
- Ilioinguinal nerve: This nerve enters the inguinal canal through the space between the external and internal oblique muscles.
- Genital branch of the genitofemoral nerve: This nerve is part of the spermatic cord.
Integrity of the Inguinal Canal
- Flap-valve Mechanism: The inguinal canal's oblique orientation allows its anterior and posterior walls to close together like a flap during increased intra-abdominal pressure, maintaining its integrity.
- Guarding of the Inguinal Rings: The deep inguinal ring is protected in front by the internal oblique muscle. The superficial inguinal ring is safeguarded behind by the conjoint tendon and the reflected part of the inguinal ligament.
- Shutter Mechanism: The internal oblique muscle forms a flexible arch around the canal. When it contracts, it pulls the roof down towards the floor, similar to a shutter. The conjoint tendon, which is formed by the merging fibres of the internal oblique and transversus abdominis muscles, plays a crucial role in this mechanism.
- Slit-valve Mechanism: Contraction of the external oblique muscle brings the two crura (medial and lateral) of the superficial inguinal ring together, functioning like a slit valve.
- Ball-valve Mechanism: The cremaster muscle pulls the testis upwards, and the spermatic cord blocks the superficial inguinal ring, acting like a ball valve.
Structures Passing Through the Deep and Superficial Inguinal Rings
- In males:
- Ductus deferens and its artery
- Testicular artery and accompanying veins
- Obliterated remains of processus vaginalis
- Autonomic nerves and lymphatics
- In females:
- Round ligament of uterus
- Lymphatics from the uterus
- Ilioinguinal nerve: This nerve enters the inguinal canal by piercing the wall, not through the deep inguinal ring.
Iliopubic Tract
The iliopubic tract is a reinforced lower edge of the fascia transversalis. It appears as a fibrous band that runs parallel to and behind the inguinal ligament. When viewed from the back in the inguinal region, the iliopubic tract is situated behind the inguinal ligament.
Iliopectineal Arcus or Ligament in the Pelvic-femoral Space
The iliopectineal arcus, also known as the iliopectineal ligament, is a fascial partition located in the pelvic-femoral space. It plays a crucial role in dividing the muscular (lateral) and vascular (medial) lacunae beneath the inguinal ligament.
- Muscular Lacuna: This compartment is responsible for housing the iliopsoas muscle, which is a major muscle involved in hip flexion and stability.
- Vascular Lacuna: This compartment contains the femoral sheath and its associated structures, including the femoral vessels, the femoral branch of the genitofemoral nerve, and the femoral canal.
The femoral sheath is a funnel-shaped fascial covering that encases the upper portion of the femoral vessels. It extends from the inguinal ligament down to the adductor canal and is divided into three compartments:
- Lateral Compartment: This section contains the femoral artery and the femoral branch of the genitofemoral nerve.
- Intermediate Compartment: This compartment is occupied by the femoral vein.
- Medial Compartment (Femoral Canal): This area houses deep inguinal lymph nodes and lymphatic vessels.
Triangles
Inguinal Triangle (of Hesselbach)
- Inferiorly: by the medial third of the inguinal ligament.
- Medially: by the lower lateral edge of the rectus abdominis.
- Laterally: by the inferior epigastric vessels.
The inguinal triangle, also known as Hesselbach's triangle, is located next to the back wall of the inguinal canal.
Inguinal Triangle (Hesselbach's Triangle)
The inguinal triangle is situated beneath the back wall of the inguinal canal, visible on the inside of the lower front part of the abdominal wall.
Boundaries of the Inguinal Triangle
- Medial: Lower 5 cm of the lateral edge of the rectus abdominis muscle.
- Lateral: Inferior epigastric artery.
- Inferior: Medial half of the inguinal ligament.
Floor Coverage
- Peritoneum
- Extra-peritoneal tissue
- Fascia transversalis
The medial umbilical ligament, which is the obliterated umbilical artery, crosses the inguinal triangle, dividing it into medial and lateral sections. Medial Section. Reinforced by the conjoint tendon. Lateral Section. Weaker, making it prone to direct inguinal hernias.
Inguinal Hernia
The inguinal canal, which is meant to reinforce the front abdominal wall, particularly through the deep and superficial inguinal rings, is prone to hernias, especially in males. An inguinal hernia happens when an organ pushes through the abdominal wall tissues in the inguinal area.
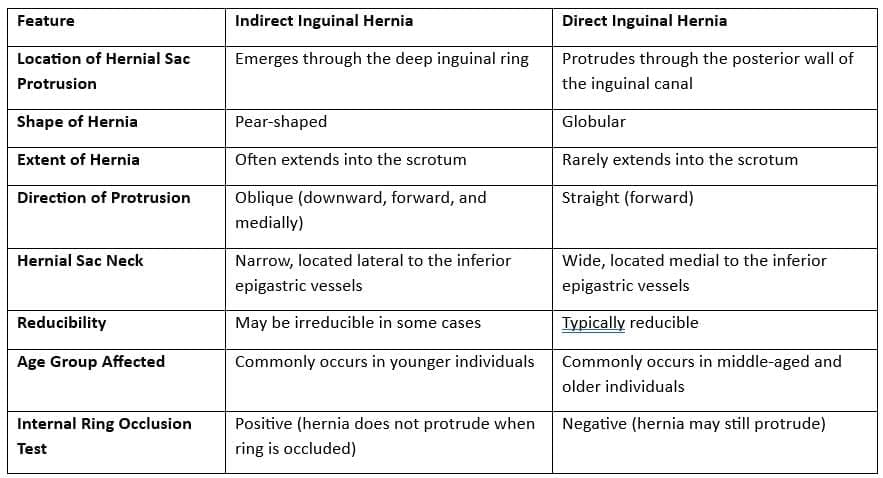
Indirect Inguinal Hernia
An indirect inguinal hernia occurs when tissue protrudes through the deep inguinal ring, situated next to the inferior epigastric vessels.
- Many indirect hernias are associated with the abnormal persistence of a patent processus vaginalis, a tubular extension of the peritoneum that usually closes after birth.
- Others are acquired due to the gradual weakening of the posterior wall of the inguinal canal near the deep inguinal ring, often due to aging or heavy lifting.
- The hernia may either pass through the deep ring or stretch it, making the ring less distinct.
- Small indirect hernias typically appear below and to the side of the conjoint tendon, while larger ones can distort and thin the tendon above.
- Small indirect hernias that do not extend beyond the inguinal canal are covered by the same inner layers as the spermatic cord: the internal spermatic fascia and cremaster.
- If the hernia protrudes through the superficial inguinal ring, it is also covered by external spermatic fascia.
- In cases involving a fully patent processus vaginalis, hernia contents can descend as far as the tunica vaginalis in front of the testis.
- Many individuals with a partial or fully open processus vaginalis may develop an indirect hernia during childhood, while in others, it may not occur until adulthood, often triggered by increased intra-abdominal pressure or sudden muscle strain.
Direct Inguinal Hernia
- A direct inguinal hernia forms medial to the inferior epigastric vessels.
- It is always caused by an acquired weakness in the posterior wall of the inguinal canal.
- As this type of hernia grows, it can push through the front wall of the inguinal canal or the superficial inguinal ring.
- During this process, it becomes covered by external spermatic fascia.
- A direct inguinal hernia may resemble an indirect hernia, making it difficult to distinguish between the two during a clinical examination.
- These hernias usually occur in older adults due to age-related tissue weakening.
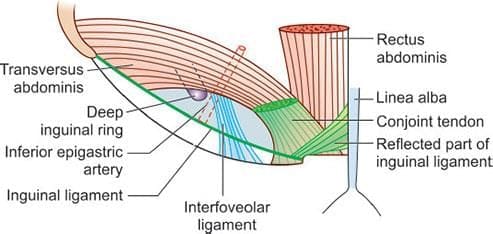 Interfoveolar ligament
Interfoveolar ligament
Clinical Characteristics of Inguinal Hernias
- Indirect inguinal hernias generally move from the side towards the middle, following the path of the inguinal canal.
- Direct inguinal hernias usually protrude more directly towards the front.
- When a hernia is pushed back in, applying pressure to the deep inguinal ring can prevent an indirect hernia from becoming visible while standing or straining.
- Distinguishing between an indirect and a direct hernia through a clinical examination alone can be challenging, but the examination can provide initial indications.
- Direct hernias typically have a wide neck, which reduces the risk of strangulation.
Types of Hernias
- Direct Inguinal Hernia
- Indirect Inguinal Hernia
- Femoral Hernia
Note: Surgical repair of a hernia may injure the iliohypogastric nerve, leading to numbness in the corresponding abdominal wall and inguinal area, or the ilioinguinal nerve, resulting in numbness in the corresponding penis, scrotum, and medial thigh.
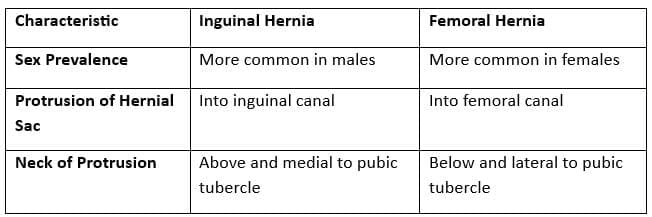
Differences between inguinal and femoral hernias
Differences between the indirect and direct inguinal hernia
After reducing the hernia, pressure is applied to the deep inguinal ring, and the patient is asked to cough. If the hernia does not reappear, it is an indirect inguinal hernia (as it protrudes through the deep inguinal ring). If the hernia reappears, it is a direct inguinal hernia (as it protrudes through Hesselbach's triangle).
Femoral Hernia
- A femoral hernia happens when tissue pushes through the femoral ring into the femoral canal, which is located beside the femoral vein.
- These hernias occur just below the inguinal ligament, in an area of natural weakness known as the femoral canal.
- The femoral canal is a potential space beneath the inguinal ligament, near the pubic tubercle, where herniated tissue can take up space.
- For a hernia to enter the femoral canal, it must first pass through the femoral ring.
- The femoral ring is bordered by:
- The inguinal ligament at the front
- The pectineal ligament at the back
- The lacunar ligament on the inside
- The femoral vein on the outside
- The femoral sheath contains three compartments, organized from outside to inside:
- The femoral artery and its branches
- The femoral vein and its tributaries
- The femoral canal, which houses lymphatic vessels and deep inguinal lymph nodes
Spermatic Cord
The spermatic cord is made up of the vas deferens and the tissues around it. It runs from the deep inguinal ring to the testis.
Tunica Vaginalis
- The spermatic cord is covered by a serosal layer called the tunica vaginalis. This layer is part of the peritoneum and passes through the transversalis fascia.
Layers of the Spermatic Cord
- External Spermatic Fascia: This layer comes from the aponeurosis of the external oblique muscle.
- Cremasteric Muscle and Fascia: This is a continuation of the internal oblique muscle and its fascia.
- Internal Spermatic Fascia: This layer is a continuation of the transversalis fascia.
Contents of the Spermatic Cord
- Tunica Vaginalis: This is derived from the remnants of the processus vaginalis.
- Arteries: The spermatic cord contains several arteries, including the testicular artery, the artery to the ductus deferens, and the cremasteric artery.
- Nerves: Nerves present in the spermatic cord include the nerve to the cremaster and sympathetic and parasympathetic nerves.
- Pampiniform Venous Plexus: This is a network of veins in the spermatic cord.
- Lymphatic Vessels: These vessels are also part of the contents of the spermatic cord.
Note: The ilio-inguinal nerve is not located inside the spermatic cord. Instead, it runs along the outside of the cord in the inguinal canal, specifically on the superficial surface of the external spermatic fascia.
Testis, Epididymis, and Scrotum
The testis develops in the abdomen and descends into the pelvis before finally settling in the scrotum. It is partially encased by a pouch of peritoneum known as the tunica vaginalis, which covers the testis on the sides and front but leaves the back exposed.
Beneath the tunica vaginalis lies a thick layer of connective tissue called the tunica albuginea, which is white in color. Below this layer is the tunica vasculosa, a layer of connective tissue rich in blood vessels.
The tunica albuginea extends inward, creating connective tissue septa that divide the testis into approximately 250 small sections called lobules. Each lobule contains one to four coiled seminiferous tubules. These septa converge at the back of the testis to form a structure known as the mediastinum.
The testis comprises the seminiferous tubules, which house Leydig cells, also known as interstitial cells.
Spermatogenesis
- Inside the seminiferous tubules, spermatogonial stem cells located near the inner wall divide towards the centre to produce sperm.
- The process of spermatogenesis takes around 74 days, during which approximately 200 to 300 million spermatozoa are produced daily, with roughly half maturing into viable sperm.
- Leydig cells secrete hormones such as testosterone, androstenedione, and dehydro-epiandrosterone (DHEA) when stimulated by luteinising hormone (LH) from the pituitary gland.
The path of sperm movement in the testis includes:
- Seminiferous tubules
- Straight tubules
- Rete testis
- Efferent ductules in the testis
The tunica vaginalis, a serous membrane covering the testis, originates from the process vaginalis of the peritoneum. This process allows the testis to descend from the abdomen into the scrotum during fetal development. The tunica vaginalis covers the front and sides of both the testis and the epididymis.
The tunica vaginalis consists of two layers:
- The parietal layer, which forms the inner layer of the scrotum.
- The visceral layer, which is attached to the testis and epididymis.
The processus vaginalis is an embryonic extension of the peritoneum that accompanies the testis through the inguinal canal during its descent into the scrotum. This process closes off to form the tunica vaginalis in males. If the processus vaginalis remains open, it can lead to conditions such as a congenital indirect inguinal hernia or a congenital hydrocele.
Blood supply
- The testicular arteries, which are branches of the abdominal aorta located just below the renal arteries, provide the primary arterial supply.
- There is also a rich collateral arterial supply from several sources, including:
- The internal iliac artery, through the artery of the ductus deferens.
- The inferior epigastric artery, via the cremasteric artery.
- The femoral artery, through the external pudendal artery.
- This collateral circulation is usually sufficient to allow for the ligation of the testicular artery during surgery without causing complications.
Venous Drainage
- The pampiniform plexus is a network of spermatic veins located on the surface of the epididymis, running alongside the spermatic arteries.
- This plexus facilitates a countercurrent exchange of heat and testosterone between the spermatic arteries and veins.
- The testicular veins are formed by the merging of veins from the pampiniform plexus around the testis.
- The right testicular vein drains into the inferior vena cava, while the left testicular vein drains into the left renal vein.
Lymphatic Drainage
- Testicular lymphatics drain into the para (lateral) and pre (anterior) aortic lymph nodes.
- The epididymis is a tightly coiled duct, measuring about 6 metres in length when uncoiled, responsible for propelling sperm into the ductus deferens.
- It comprises a head, body, and tail, with the tail connecting to the ductus deferens.
- Sperm undergo maturation and gain motility in the epididymis, where they are stored until ejaculation.
- The principal cells lining the epididymis carry out several important functions, including:
- Resorbing testicular fluid that originated in the efferent ductules.
- Phagocytosing dying sperm or residual spermatids not cleared by Sertoli cells.
- Secreting glycoproteins that bind to the sperm cell membrane, along with sialic acid and glycerophosphocholine, which prevent premature fertilisation until the sperm enters the female reproductive tract.
- The tail of the epididymis features a muscular coat with three layers: an inner longitudinal layer, a middle circular layer, and an outer longitudinal layer of smooth muscle. These layers contract to propel sperm from the tail into the ductus deferens, a process known as sperm emission.
- After residing in the epididymis for 18 to 24 hours, sperm develop motility, although certain proteins in the epididymal fluid inhibit full motility until ejaculation.
- Sperm may take up to 12 days to traverse the epididymis, but they can be stored there for several weeks.
- Following ejaculation into the female reproductive tract, sperm ascend the uterus to the isthmus of the uterine tubes, where they undergo capacitation. This maturation process involves:
- Enhancing sperm motility.
- Preparing for the acrosome reaction.
- Capacitation typically lasts from 1 to 10 hours (averaging 7 hours). During this period, sperm lose excess cholesterol, the acrosome membrane weakens, and the sperm membrane becomes more permeable to calcium ions.
- Capacitated sperm rapidly move from the isthmus to the tubal ampulla, where fertilisation occurs.
- After ovulation, the oocyte remains fertilisable for 48 hours, although the chances of fertilisation diminish significantly by 18-24 hours. Sperm can survive for 24-48 hours in the female reproductive tract if the environment is conducive.
- With appropriate estrogenic cervical mucus, sperm can remain capable of fertilisation for 3-7 days during the periovulatory period.
- After 24-48 hours of intercourse, sperm generally lose their ability to fertilise.
- The scrotum houses the testis and epididymis, playing a crucial role in regulating testicular temperature at 35°C (95°F), which is essential for spermatogenesis. This temperature is two degrees lower than the normal body temperature of 37°C (98.6°F).
- The scrotum consists of thin skin with sparse hair and no fat.
- The dartos muscle, located subcutaneously, wrinkles the skin and continues with the superficial penile and perineal fascia.
- The cremaster muscle covers the scrotum and elevates the testis upon contraction.
- Arterial supply to the scrotum comes from the external pudendal arteries and the posterior scrotal branches of the internal pudendal arteries.
- The nerve supply includes:
- Anterior scrotal branch of the ilioinguinal nerve.
- Genital branch of the genitofemoral nerve.
- Posterior scrotal branch of the perineal branch of the pudendal nerve.
- Perineal branch of the posterior femoral cutaneous nerve.
- The dartos fascia, a layer of connective tissue, is found in the penile shaft and scrotum. The penile portion is referred to as the superficial fascia of the penis, which continues as the dartos proper in the scrotum. Dartos fascia also connects with Colles fascia of the perineum and Scarpa's fascia of the abdomen. Dartos fascia is located just beneath the skin, above the external spermatic fascia in the scrotum, and above Buck's fascia in the penile shaft. It contains smooth muscles that receive signals from postganglionic sympathetic nerve fibres via the ilioinguinal nerve and the posterior scrotal nerve.
FAQs on Chapter Notes: Abdomen - 2
| 1. What is the nerve supply to the abdominal organs? |  |
| 2. What are the main arteries branching from the abdominal aorta? | |
| 3. How does venous drainage of the abdomen occur? | |
| 4. What is the difference between inguinal hernia and femoral hernia? | |
| 5. What structures are contained within the spermatic cord? | |



