NEET PG Exam > NEET PG Notes > Gynaecology and Obstetrics > Chapter Notes: Fetal monitoring during labour
Chapter Notes: Fetal monitoring during labour

What is the problem
- The goal of fetal monitoring during labor is to predict and identify fetal asphyxia before it causes harm to the fetus or newborn, especially brain damage.
- Fetal asphyxia is a condition where there is poor blood gas exchange, leading to low oxygen levels (hypoxemia) and high carbon dioxide levels (hypercapnia).
- The term progressive in this context means that the condition worsens over time.
- During labor, transient hypoxemia can happen without causing any harm, but serious asphyxia requires ongoing lack of oxygen with significant metabolic acidosis.
- To diagnose fetal asphyxia, doctors need to assess blood gas and acid-base levels.
- A critical point is when the umbilical artery base deficit is greater than 12 mmol/l, which indicates a risk of brain damage at delivery.
Relationship of fetal asphyxia to brain damage
- Over the past 50 years, researchers have studied asphyxia in various animal models.
- These studies have shown that a certain level and duration of fetal asphyxia can lead to brain damage.
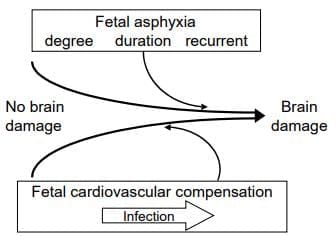
- A significant observation is that, despite a single exposure to asphyxia, some fetuses experience no brain damage, some have brain damage, and a few may die.
- The outcome of asphyxia is affected by how the fetus responds to it.
- Fetal cardiovascular compensation can include:
- Increasing arterial pressure
- Centralizing cardiac output
- Boosting cerebral blood flow
- However, if asphyxia continues, the fetus may reach a point where cardiovascular decompensation occurs, leading to cerebral hypoxia and potentially causing brain damage if it lasts too long.
- The differences in fetal cardiovascular responses are crucial to understanding the varying outcomes in laboratory studies.
The outcome, i.e. no brain damage/brain damage is a result of the characteristics of the fetal asphyxia and the quality of the fetal cardiovascular compensation.
- Our knowledge of the link between fetal asphyxia and brain damage comes mainly from these laboratory studies.
- It is clear that the connection between fetal asphyxia and brain damage is complex and can be influenced by several factors, including:
- Fetal maturity
- Level, duration, and type of asphyxia
- Quality of the fetal cardiovascular response
- The introduction of microelectrode blood gas systems has allowed us to safely examine these factors in all pregnancies at delivery.
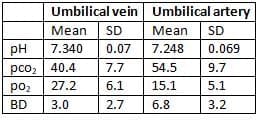
- Blood gas and acid-base measures from the umbilical vein and artery at delivery provide valuable insights into asphyxia during labor.
- The umbilical vein indicates how well maternal-fetal blood gas exchange is working, while the umbilical artery shows the acid-base status of the fetus.
- Data from 21,744 deliveries in our center regarding these measures is summarized in a table.
Mean blood gas and acid-base measures for 21,744 deliveries
- Recent studies highlight the need for quality data for accurate interpretation of these measures.
- There can be several procedural and technical errors during umbilical cord blood sampling and blood gas analysis.
- For optimal results, a sample from both the umbilical vein and artery should be taken.
- A single sample from the umbilical vein can show the metabolic state but may not rule out an arterial metabolic acidosis.
- Drawing two aliquots from the umbilical vein can indicate procedural errors if the pH difference between the vein and artery is less than 0.02.
- The accuracy of metabolic acidosis measures depends on the quality of pH and pCO2 estimations.
- If the pCO2 value is outside the normal range or if the pCO2 difference between the artery and vein is negative or less than 4 mmHg, the reliability of pCO2 results should be questioned, focusing interpretation on pH alone.
- An umbilical artery blood measure of metabolic acidosis is the best sign of the tissue oxygen debt the fetus has experienced.
- Recent findings suggest that a higher risk to the fetus begins when the umbilical artery base deficit exceeds the average.
- In studies assessing the threshold for significant complications, moderate and severe issues occurred only in fetuses with a base deficit greater than 12 mmol/l.
- The incidence of moderate to severe complications rises with a base deficit of 12-16 mmol/l to about 10%.
- When the base deficit exceeds 16 mmol/l, the incidence of moderate and severe complications can be as high as 40%.
- The aim of clinical studies using microelectrode blood gas systems has been to see if findings from research labs apply to human fetuses.
- The findings support that a fetus can experience asphyxia without immediate problems, but specific levels and durations of asphyxia can lead to cerebral dysfunction in newborns and, in some cases, brain damage that results in disabilities in surviving children.
Prevalence of Fetal Asphyxia
Prevalence of intrapartum fetal Aspyxia
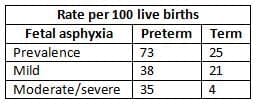
- Recent studies have provided data on the prevalence of mild, moderate, and severe fetal asphyxia during the intrapartum period.
- The prevalence and severity of fetal asphyxia at delivery in both preterm and term pregnancies have been summarised in research findings.
- Mild Fetal Asphyxia:
- There is currently no evidence linking mild fetal asphyxia to major deficits in children.
- Long-term follow-up studies have shown no association between mild asphyxia and minor disabilities later in childhood.
- These findings highlight the importance of timely clinical management during mild fetal asphyxia cases.
- Early identification and intervention can help prevent potential cerebral dysfunction and long-term deficits in affected children.
- Unknown Duration and Nature of Asphyxia:
- While the prevalence of intrapartum fetal asphyxia at delivery is known, the duration and nature of asphyxia in most cases remain unclear.
- It is uncertain when the asphyxia detected at delivery actually began-whether it occurred before the onset of labour or was part of a series of asphyxial episodes that started earlier.
Diagnosis and Prediction of Fetal Asphyxia
- Fetal asphyxia is diagnosed through blood gas and acid-base assessments.
- Continuous monitoring of fetal acid-base status in clinical settings is not yet feasible.
- Diagnosis can currently be confirmed via periodic fetal blood sampling during labor or at delivery.
- There is a need for criteria to identify fetuses at risk for fetal asphyxia to justify blood sampling during labor.
- Limitations of Clinical Risk Scoring:
- Many studies have highlighted the limitations of clinical risk scoring in predicting fetal asphyxia.
- A significant percentage of fetal asphyxia cases (23-40%) occurred in pregnancies without any clinical risk factors.
- The term 'low risk' based on clinical markers is not applicable to fetal asphyxia during labor.
- In cases with clinical risk factors, various complications influenced risk, and no single risk factor was strongly associated with intrapartum fetal asphyxia.
- The positive predictive value for both antepartum and intrapartum risk factors for intrapartum fetal asphyxia was only 3%.
- This low predictive value indicates a significant issue with false positives in predicting intrapartum fetal asphyxia.
Introduction to Electronic Fetal Heart Rate Monitoring
- Edward Hon's Publication (1958):This publication is considered the beginning of the belief that electronic fetal heart rate monitoring (EFM) could be useful in predicting intrapartum fetal asphyxia.
- Observations in the 1960s and 1970s: During this time, observations supported the idea that EFM might be a valuable screening test for predicting intrapartum fetal asphyxia.
- Clinical Experiences: Clinical experiences were similar to those of other researchers, with anecdotal evidence suggesting a link between abnormal fetal heart rate patterns and fetal asphyxia, leading to varying outcomes.
- Laboratory Studies: Laboratory studies established a connection between fetal heart rate behavior and fetal hypoxemia (low oxygen levels) and metabolic acidosis (excess acidity in the body).
- Late Decelerations: Late decelerations occur when fetal oxygen levels drop below a critical threshold. The time between the onset of a contraction and the start of a deceleration indicates how long it takes for oxygen levels to fall below this threshold.
- Mechanism of Late Decelerations: Late decelerations caused by fetal hypoxemia in a previously normal fetus are triggered by reflex bradycardia (slow heart rate) initiated by chemoreceptors. This reflex can be blocked by atropine, a medication.
- Impact on Myocardium in Hypoxic Fetuses: In fetuses that were previously hypoxic, bradycardia is likely a result of a direct effect on the myocardium (heart muscle).
- Growth of EFM in the 1970s: Due to the findings related to fetal heart rate patterns and their connection to fetal well-being, the use of electronic fetal heart rate monitoring (EFM) grew rapidly in the 1970s.
Assessing EFM as a Screening Test
- Essential Criteria for Screening Test:
- The clinical issue must require intervention. Intrapartum fetal asphyxia is a serious concern that, in certain cases, warrants intervention.
- The benefits of the test should outweigh any potential risks.
- Since the late 1970s, it has been recognized that this balance has not been adequately evaluated.
- Impact of EFM:
- The introduction of Electronic Fetal Monitoring (EFM) contributed to a decrease in intrapartum fetal deaths.
- However, instances of intrapartum fetal deaths continue to be reported.
- UK Confidential Enquiry Findings:
- 9% of all deaths between 20 and 44 weeks of gestation were associated with labour.
- Among normally formed babies weighing at least 2500 g, 4.3% were linked to intrapartum events.
- Need for Rigorous Trials: Well-designed, randomized controlled trials are necessary to accurately evaluate the true risks and benefits of medical interventions.
- Lack of Comparative Trials: No randomized clinical trials have directly compared fetal heart rate surveillance with intermittent fetal heart rate auscultation.
- Review of Randomized Clinical Trials: Nine randomized clinical trials were reviewed, with findings indicating that EFM did not consistently lead to reduced fetal and newborn complications.
- False Positives and Misinterpretation: These trials have enhanced understanding of false positives in electronic fetal heart rate monitoring, which can result in unnecessary interventions.
- Increased Intervention Rates:
- Evidence suggests that electronic fetal heart rate monitoring, compared to intermittent auscultation, is associated with higher rates of:
- Caesarean sections due to fetal distress and dystocia.
- Operative delivery and general anaesthesia.
- Misinterpretation Issue: It is crucial to note that these outcomes are a result of misinterpretation of fetal heart rate data rather than the monitoring method itself.
Clinical Management Guidelines for Electronic Fetal Monitoring
- National organizations have established consensus documents on fetal monitoring during labor, grounded in the available evidence.
- Recent clinical guidelines encompass:
- ACOG Technical Bulletin Number 207, 1995 (USA)
- SOGC Clinical Practice Guideline Number 112, 2001 (Canada)
- RCOG Evidence-based Clinical Guideline Number 8, 2001 (UK).
- These guidelines were formulated by experts to mirror the best available evidence at the time.
- Absence of Specific Algorithms:
- Current guidelines lack a specific algorithm for interpreting fetal heart rate patterns.
- The ACOG and SOGC guidelines categorize fetal heart rate patterns as:
- Reassuring
- Non-reassuring
- However, they do not provide detailed criteria or timelines.
RCOG Guidelines on Fetal Heart Rate Traces
- The RCOG guidelines categorize fetal heart rate traces as:
- Normal
- Suspicious
- Pathological
- Nevertheless, no guidelines have offered data on the sensitivity, specificity, and predictive value of these defined patterns.
NIH Research-Planning Workshop, 1997:
- The lack of clear definitions for fetal heart rate tracings was addressed by a NIH research-planning workshop in 1997.
- The workshop aimed to establish clear definitions for fetal heart rate tracings to guide future research.
- Despite a general consensus on the utility of electronic fetal monitoring, there was no agreement on strict clinical management guidelines based on fetal heart rate patterns.
- Many fetuses exhibit fetal heart rate tracings that fall between normal and critical extremes.
- The workshop concluded that evidence-based algorithms for management require further investigation.
- This perspective has been reaffirmed in recent discussions.
An Algorithm for Predicting Fetal Asphyxia Based on Fetal Heart Rate
Understanding Fetal Heart Rate (FHR) Records
- When looking at an FHR record, there are two main concerns: how to classify FHR variables and how consistently different observers interpret these variables.
- There are various definitions for individual FHR variables, such as baseline FHR, baseline FHR variability, accelerations, and decelerations. A good reference for these definitions is the RCOG Evidence-based Clinical Guideline Number 8. However, there are still differences in how decelerations are classified. Some clinicians focus on the timing of the lowest point of the deceleration, while others emphasize the shape of the waveform. Until a consensus is reached, it is crucial to define and use criteria consistently.
- Despite improvements in computer-based FHR interpretation, most clinical records are still assessed visually. The inconsistency between observers in interpreting FHR variables is well-documented.
- Our findings show the following inter-observer Kappa values:
- Baseline FHR: 0.70
- Baseline FHR variability: 0.55
- FHR accelerations: 0.57
- Variable decelerations: 0.46
- Late and prolonged decelerations: 0.57
- Scoring FHR patterns over time can help improve observer reliability. Records should be scored in 10-minute segments, and careful scoring of several cycles is needed to determine the overall pattern, typically represented by six cycles over 1 hour. Our experience suggests a high level of reliability in classifying FHR patterns within a 1-hour recording [29].
An FHR algorithm to predict fetal asphyxia
- A matched case-control study in term pregnancies aimed to define a threshold of FHR patterns for intrapartum fetal asphyxia, identifying intermediate patterns. FHR records were assessed for each variable over six 10-minute cycles in each hour.
- The FHR variables linked to fetal asphyxia included the absence of baseline variability and the presence of late and prolonged decelerations. Three FHR patterns were identified based on these variables across six 10-minute cycles within 1 hour. The proposed patterns for interpreting electronic FHR records are summarized in Table 8.3.
- Key Observations from the Study:
- The predictive FHR patterns had a sensitivity of 75% in identifying cases of fetal asphyxia.
- In the 25% of cases not identified, the asphyxia was mild.
- The positive predictive value of a predictive FHR pattern was strong, indicating moderate or severe asphyxia.
- However, the positive predictive value of potentially predictive patterns was poor, at 10% and 5% respectively.
- These potentially predictive patterns accounted for over 50% of fetal asphyxia cases, ranging from mild to moderate.
- Clinical Challenge:
- The challenge for clinicians with potentially predictive patterns is significant.
- Ignoring the pattern may lead to missing severe fetal asphyxia in one out of ten cases, while acting on the pattern could result in unnecessary interventions in nine out of ten cases.
Predictive and Potentially Predictive Fetal Heart Rate Patterns for Intrapartum Fetal Asphyxia

Can Predictive FHR Patterns Prevent Moderate to Severe Fetal Asphyxia?
- Electronic Fetal Monitoring (EFM) is not definitively proven to be better than its drawbacks, according to Grade 1 evidence.
- However, our research suggests that the EFM algorithm can be beneficial in certain cases when used as a screening tool.
- The benefits of EFM in predicting and preventing intrapartum fetal asphyxia were assessed over a decade in both term and preterm pregnancies.
- A predictive or potentially predictive fetal heart rate (FHR) pattern was observed in most cases.
- Interventions and deliveries occurred in 98 out of 166 term pregnancies and 21 out of 24 preterm pregnancies, largely based on predictive FHR patterns.
- This evaluation method did not eliminate all cases of moderate or severe fetal asphyxia.
- However, in some instances, accurate prediction and diagnosis led to timely interventions during the first or second stage of labor, potentially preventing the escalation of mild to moderate or severe asphyxia.
- This approach also contributed to reducing the severity of moderate asphyxia.
Supplementary Assessments in Fetal Monitoring
Vibroacoustic Stimulation
- Vibroacoustic stimulation (VAS) involves using sound and vibration to stimulate the fetus and assess its response. The acceleration response to VAS has been investigated as a potential indicator to rule out fetal acidosis. However, the predictive value of this method remains unclear.
- Amnioinfusion:
- Amnioinfusion is a procedure where fluid is infused into the amniotic cavity, often used in cases of oligohydramnios (low amniotic fluid). Several trials have shown that amnioinfusion can have a positive effect by reducing variable decelerations and the rate of Caesarean sections for fetal distress.
- Fetal ECG Waveform Analysis:
- Fetal electrocardiographic (ECG) waveform analysis is an appealing method because the ECG signal can be obtained from the same fetal scalp electrode used for recording the fetal heart rate (FHR).
- Laboratory studies have investigated the effects of hypoxemia and acidosis on the ST segment of the fetal ECG. In research on acute hypoxemia, it was observed that the ratio of T-wave height to QRS height increased, although this finding has not been consistent across all studies.
- Initial clinical observations have suggested a need for caution in interpreting ST waveforms. Recent advancements in FHR analysis have led to monitoring systems that include automated fetal ECG ST segment analysis alongside standard FHR and uterine contraction data.
- A meta-analysis of two randomized clinical trials indicated that using ST waveform analysis could reduce the incidence of metabolic acidosis in newborns at delivery and decrease operative deliveries for fetal distress. However, later reports have highlighted limitations in the sensitivity of ST waveform analysis for identifying fetal asphyxia with significant metabolic acidosis.
- Fetal Pulse Oximetry:
- Fetal pulse oximetry was introduced as a non-invasive method to measure fetal oxygen saturation and improve intrapartum assessment during labor. However, randomized clinical trials have not convincingly demonstrated that this supplementary test reduces unnecessary interventions.
- Near-Infrared Spectroscopy (NIRS):
- Near-infrared spectroscopy (NIRS) has been developed for continuous, non-invasive real-time measurement of changes in fetal cerebral oxygenation and blood flow during labor. Initial reports on the application of NIRS for fetal assessment during labor have been published.
- Conclusion:
- While these supplementary tests provide additional information for fetal monitoring, further research is needed to clarify their role and effectiveness in clinical practice.
Upstream Connection Error
Issue Details
- There is a problem with the connection that happens before the headers are transmitted.
- The reason for the reset is due to the termination of the connection.
The document Chapter Notes: Fetal monitoring during labour is a part of the NEET PG Course Gynaecology and Obstetrics.
All you need of NEET PG at this link: NEET PG
FAQs on Chapter Notes: Fetal monitoring during labour
| 1. What is fetal asphyxia and how is it diagnosed? |  |
Ans.Fetal asphyxia refers to a condition where a fetus does not receive enough oxygen during labor, leading to potential brain injury or other complications. Diagnosis typically involves monitoring fetal heart rate (FHR) patterns using cardiotocography, assessing maternal factors, and considering additional tests like fetal scalp blood sampling to evaluate blood pH levels.
| 2. What role does the FHR algorithm play in predicting fetal asphyxia? | |
Ans.The FHR algorithm analyzes patterns in the fetal heart rate to identify abnormalities that may indicate asphyxia. By tracking variations in heart rate and response to contractions, healthcare professionals can use the algorithm to make timely decisions regarding interventions, potentially improving outcomes for the fetus.
| 3. What supplementary assessments are used alongside fetal monitoring during labor? | |
Ans.Supplementary assessments may include ultrasound examinations to evaluate fetal growth and positioning, maternal vital signs monitoring, and blood tests to check for conditions like anemia or infection. These assessments provide a comprehensive view of both fetal and maternal health, aiding in the management of labor.
| 4. What are the current challenges in fetal monitoring during labor? | |
Ans.Current challenges in fetal monitoring include the variability in interpreting FHR patterns, the potential for false positives leading to unnecessary interventions, and the need for continuous monitoring resources. Additionally, there is a growing emphasis on balancing technology use with clinical judgment in high-stakes situations.
| 5. How can healthcare professionals enhance the prediction of fetal asphyxia? | |
Ans.Healthcare professionals can enhance prediction by integrating advanced monitoring technologies, undergoing regular training on FHR interpretation, and utilizing a multidisciplinary approach that includes obstetricians, midwives, and neonatologists. Continuous evaluation of monitoring techniques and protocols can further improve outcomes for at-risk fetuses.
About this Document

4.93/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: Chapter Notes: Fetal monitoring during labour for NEET PG 2026 is part of Gynaecology and Obstetrics preparation. The notes and questions for Chapter Notes: Fetal monitoring during labour have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Fetal monitoring during labour covers topics like and Chapter Notes: Fetal monitoring during labour Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Fetal monitoring during labour.
Introduction of Chapter Notes: Fetal monitoring during labour in English is available as part of our Gynaecology and Obstetrics for NEET PG & Chapter Notes: Fetal monitoring during labour in Hindi for Gynaecology and Obstetrics course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: Chapter Notes: Fetal monitoring during labour
Description
Chapter Notes: Fetal monitoring during labour of Gynaecology & Obstetrics with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET PG exam.
Information about Chapter Notes: Fetal monitoring during labour
In this doc you can find the meaning of Chapter Notes: Fetal monitoring during labour defined & explained in the simplest way possible. Besides explaining types of Chapter Notes: Fetal monitoring during labour theory, EduRev gives you an ample number of questions to practice Chapter Notes: Fetal monitoring during labour tests, examples and also practice NEET PG tests


Related Searches
Summary, mock tests for examination, Chapter Notes: Fetal monitoring during labour, Chapter Notes: Fetal monitoring during labour, pdf , shortcuts and tricks, Exam, Important questions, past year papers, ppt, study material, practice quizzes, Viva Questions, Previous Year Questions with Solutions, MCQs, Objective type Questions, Sample Paper, Semester Notes, Extra Questions, Chapter Notes: Fetal monitoring during labour, video lectures, Free;