Chapter Notes: Analgesia and anaesthesia


Pain in Labour
Pain during labour is defined by the International Association for the Study of Pain as an unpleasant sensory and emotional experience associated with real or potential tissue damage. In simpler terms, it refers to the pain experienced during childbirth, which can vary in intensity and nature.
- Prevalence of Severe Pain
- First-time Mothers (Nulliparous): Approximately 60-70% experience severe pain.
- Women Who Have Given Birth Before (Multiparous): About 35-40% experience severe pain.
- Potential Causes of Pain During Labour
- Physiological Causes: Such as contractions, cervical dilation, and the second stage of labour.
- Obstructed Labour: When the baby cannot pass through the birth canal.
- Fetal Position: An abnormal position of the baby can increase pain.
- Extreme Anxiety: High levels of anxiety can exacerbate pain perception.
- Uterine Hyperstimulation: Excessive uterine contractions can lead to severe pain.
- Uterine Rupture: Rare but serious condition that can cause intense pain.
- Existing Conditions: Such as fibromata, tumours, or scarring from previous surgeries.
- Effects of Severe Pain
- Physical Responses: Such as increased heart rate, raised blood pressure, and higher consumption of oxygen and glucose.
- Emotional Responses: Including exhaustion, dehydration, and overall misery.
- Impact on Mother and Baby: Reduced blood flow and oxygen to the placenta and fetus, potentially leading to hyperventilation and cramps.
- Pain Relief Options
- Physiological vs. Pathological Pain: While some differentiate between these types, any severe pain exceeding tolerance should be addressed with pain relief.
- Control During Labour: Most women desire to feel in control during childbirth, but severe pain can hinder this.
- Unpredictability of Pain: The duration, nature, and intensity of pain during labour are often unpredictable.
- Openness to Pain Management: Expectant mothers should be open to understanding pain management options, including their pros and cons.
- High-Risk Pregnancies: Analgesia or anaesthesia is usually necessary and recommended in high-risk cases.
- Consultation with Anaesthetist: If there are risks associated with anaesthetic procedures, consulting an anaesthetist during pregnancy is advisable.
Obstetric Analgesia and Anaesthesia
The ideal analgesic technique in labour should:
- Provide rapid, effective, and safe pain relief for all stages.
- Not compromise maternal vital physiology or normal activity.
- Not compromise fetal vital physiology or well-being.
- Not hamper the normal processes of labour.
- Be flexible enough to convert to anaesthesia for urgent operative delivery or other intervention, e.g., manual removal of placenta.
- Meeting such an ideal would leave the mother awake, alert, comfortable, and able to void, bear down, and, if desired, even ambulate throughout labour. Unfortunately, such ideals are rarely met in medicine; however, over the past two decades, the development of low-dose neuraxial anaesthesia and analgesia (epidural and combined spinal-epidural (CSE)) has all but achieved these.
- There are two strategies for obstetric analgesia:
- Reduction of the perception of pain, i.e., reducing the brain's perception of, and the body's and mind's response to, pain.
- Reduction of the transmission of pain, i.e., reducing the ability of the nerves to conduct pain.
Methods of Implementing Strategies:
Psychological techniques are helpful for many women with mild and moderately severe pain.
- Positive attitude
- Prenatal education
- Physical and mental relaxation
- Hypnosis
- Physical methods include:
- Massage
- Relaxation techniques
- Transcutaneous electrical nerve stimulation (TENS)
- Pharmacological techniquesmay be systemic or regional/local:
- Systemic drugs may affect uteroplacental blood flow and the fetus. Examples include gaseous drugs like nitrous oxide and sevoflurane, which act rapidly with minimal metabolism and accumulation.
- Parenterally administered analgesics like morphine and pethidine are hard to titrate and can accumulate in the fetus. Fentanyl and remifentanil are potent, short-acting opioids that can be safely given under approved guidelines.
- Ketamine is a potent non-opioid analgesic that can be useful for short-term, late-second-stage analgesia in selected patients when given in small intermittent intravenous doses (3-5 mg).
- Fentanyl and remifentanil can both be administered via patient-controlled analgesia (PCA) devices. Remifentanil shows significant potential for this application, though it has been evaluated in few controlled studies. Anesthetists typically recommend PCA with these drugs when neuraxial analgesia is not an option, provided midwives are trained to oversee this method.
- Since the 1980s, regional analgesia, particularly neuraxial techniques, has transformed obstetric anesthesia and pain management. Lumbar epidurals, a standard since the late 1960s, were advanced by the findings of Wang and Behar, who demonstrated the spinal effects of neuraxial opioids. Combining intraspinal opioids with local anesthetics (LAs) creates a synergistic effect, allowing lower doses of both to achieve effective neural blockade. Techniques like continuous subarachnoid anesthesia (CSA), epidurals, and low-dose combined spinal-epidural (CSE) are widely used for labor analgesia and can be readily adapted for operative deliveries or other procedures. In the UK, CSE and occasionally CSA have largely replaced single-shot spinal anesthesia for operative deliveries, with low-dose CSE becoming the preferred choice for labor analgesia.
- Caudal Epidural Block
- The caudal epidural block may be helpful for certain gynaecological procedures, its use in obstetrics has become rare and is generally not recommended. The trans-vaginal pudendal block is occasionally used for 'lift-out' forceps or ventouse deliveries. However, this method has a high failure rate of 30%, requires a large amount of local anaesthetic (LA), which poses a risk of acute toxicity, and there is also the potential danger of injecting into the fetal head.
- Low-Dose Spinal Anaesthetic
- In exceptional situations where the obstetrician is the sole operator or when skilled anaesthesia services are unavailable, a low-dose single-shot spinal anaesthetic administered at the L3-4 or L4-5 level might be the most suitable option for operative vaginal delivery or repairing vaginal/perineal injuries.
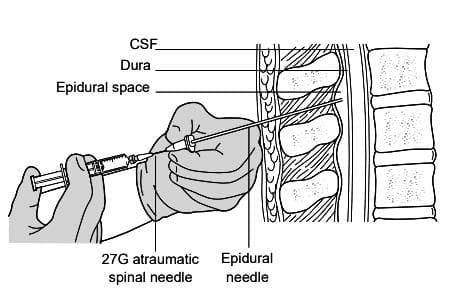 Needle-through-needle technique
Needle-through-needle technique
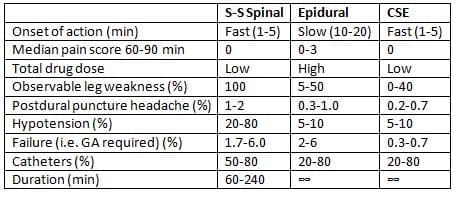
Advantages of CSE Technique
The CSE technique offers several advantages over epidural injection alone, including:
- Faster onset of action.
- Lower failure rate.
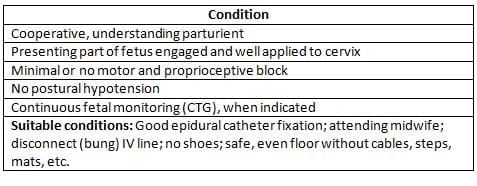
- Reduced motor block, enabling more than 90% of women to walk during labour.
While the ability to move during labour has not been shown to significantly alter delivery methods, the lighter blockade associated with CSE improves satisfaction and provides a greater sense of control for the women.
Requirements for Safe 'Walking Epidurals'
 Disadvantages of CSE
Disadvantages of CSE- Some disadvantages of CSE include:
- A slightly more complex technique, although it is relatively easy to learn.
- The dural puncture caused by the fine gauge, atraumatic spinal needle is comparable to that of using only epidurals.
- Hypotension is uncommon with low-dose techniques and can be monitored closely.
Nonetheless, neuraxial blockade is an invasive procedure that carries the risk of severe but infrequent complications.
- The actual incidence of traumatic neuropathy and infections such as epidural abscess and meningitis is not well-established, with estimates ranging from 1 in 5000 to 1 in 15,000.
- These complications can often be minimised through careful technique. Peripheral nerve injuries occurring during labour and delivery are more common, reported in approximately 1% of women receiving various forms of analgesia.
- Another significant concern is spinal epidural haematoma (SEH), particularly in patients with bleeding disorders or those on anticoagulant therapy.
- Following the administration of low molecular weight heparins (LMWHs), numerous SEH cases have been reported, especially in the USA, where LMWH doses are higher than those in Europe.
- Effective communication between anaesthetists and obstetricians, along with strict adherence to guidelines, is crucial when combining neuraxial blocks with anticoagulant therapy.
- Neuraxial anesthesia is the most commonly used method for operative delivery. However, it is not suitable for all women due to certain contraindications.
- Obstetric Indications for Neuraxial Block
- Apart from pain relief, there are various obstetric reasons that support the use of a neuraxial block during labor.
- These include:
- Breech and other abnormal presentations
- Previous operative delivery
- Large fetus
- Multiple pregnancies
In these situations, it is generally advised that mothers consider a neuraxial block during labor. This allows for a quick top-up of the epidural catheter to ensure proper anesthesia if intervention is required.
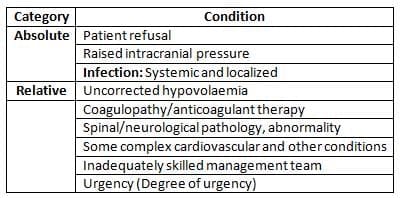
Contraindications to Neuraxial Blockade
Top-Up Block for Delivery
During instrumental delivery, where maternal effort is required, the top-up block can be adjusted to provide sensory blockade of sacral dermatomes up to the T10 level while maintaining motor function in the abdominal muscles. This allows for effective bearing down during contractions. In the case of abdominal delivery, the epidural is topped up with enough dosage to relax the abdominal muscles and block sensation up to the T4 dermatomes.
- Disadvantages of Neuraxial Anesthesia
- One disadvantage of neuraxial anesthesia for operative delivery is that it does not provide tocolysis. However, this can be managed with intravenous glyceryl trinitrate or other medications. Severe pain can increase sympathetic tone, leading to higher blood pressure, increased oxygen consumption, and reduced blood flow to the uterus, which can be harmful for at-risk mothers.
- Therefore, optimal analgesia during labor can be beneficial, especially in cases of:
- Pre-eclampsia and other hypertensive conditions
- Cardio-respiratory disorders
- In high-risk patients, neuraxial anesthesia for surgery or operative delivery is often the preferred technique. Low-dose combined spinal-epidural (CSE) can provide significant hemodynamic stability for mothers with severe aortic or mitral stenosis, obstructive cardiomyopathy, and pulmonary hypertension during elective Caesarean section. Such patients require expert management beginning early in pregnancy. Early consultation with a cardiologist and an anaesthetist is essential for establishing management plans for ongoing monitoring and care, as well as for elective or emergency delivery. Any anesthesia in these patients carries risks, and since neuraxial techniques may sometimes fail, a backup plan must be prepared with all necessary facilities and caregivers.
Informed Consent for Anaesthetic Procedures
- In developed countries during the 1990s, over 60% of women undergoing anaesthetic procedures related to pregnancy were using neuraxial analgesia.
- Factors contributing to this increase included:
- Older mothers
- Obesity
- Higher rates of Caesarean deliveries
- In vitro fertilisation procedures
- Since all expectant mothers may require pain relief or anaesthesia, it is crucial to provide detailed information about pain management and anaesthesia during the antenatal period.
- If a mother exhibits signs of anxiety, fear, or refuses treatment, it is advisable to consult an obstetric anaesthetist during the pregnancy.
- This pre-education is vital to ensure informed consent is obtained without issues.
- Such preparation is especially important in situations where analgesia or anaesthesia is needed urgently or when the mother is experiencing severe pain.
General Anaesthesia
General Anaesthesia (GA) involves the use of anaesthetic drugs to induce a state of unconsciousness and absence of sensation in the patient. This technique is used in various surgical procedures, including caesarean sections, when neuraxial anaesthesia is contraindicated or fails.
- In the early days of anaesthesia, there were concerns about the safety and efficacy of GA, especially following incidents of maternal deaths during chloroform anaesthesia.
- However, advancements in anaesthetic techniques and drugs have significantly reduced the risks associated with GA.
Current Use of General Anaesthesia
- GA is now used in less than 30% of caesarean deliveries, primarily in emergency situations.
- At some institutions, such as Queen Charlotte's Hospital in London, GA is employed in only 5% of caesarean deliveries.
- GA remains the preferred option for failed neuraxial blocks and certain surgical procedures during pregnancy and the postpartum period.
Safety and Risks
- Over the past 50 years, there has been a marked reduction in maternal mortality due to the advancement of neuraxial anaesthesia, which has become the preferred method over GA.
- GA in pregnant patients is considered more hazardous than in the general population due to potential complications such as airway difficulties, failed intubation, and pulmonary aspiration of gastric contents.
- Most direct anaesthetic deaths attributed to GA could have been prevented with better communication between obstetricians and anaesthetists, as suggested by the Confidential Maternal Mortality Reports since 1952.
Anaesthetic Risk Factors
- All pregnant women are potential candidates for anaesthesia, and it is often required in emergency situations.
- Anaesthetic risk factors should be identified during regular antenatal care and review, as expectant mothers are a 'captive' population attending for routine check-ups.
- Principal anaesthetic risk factors include patient refusal of anaesthetic procedures, previous complications with anaesthesia, proven sensitivity or allergy to anaesthetic drugs, severe medical disorders, anticoagulant therapy, thrombocytopenia, airway abnormalities, obesity, spinal abnormalities, intervertebral disc prolapse, neurological disease, complex obstetric or fetal situations, and planned surgery during pregnancy.
- Consultations for at-risk pregnant women should be arranged early in the pregnancy, and clinical judgment should guide the need for antenatal anaesthesia consultation in various cases.
Prophylactic Measures
- Pulmonary Aspiration: All parturients are at risk of pulmonary aspiration of gastric contents, so prophylactic antacid and/or H-2 blocking premedication is standard practice before both regional and GA.
- Urgent GA Avoidance: In many labours, the likelihood for operative or assisted delivery can be anticipated, and an urgent GA avoided by having neuraxial analgesia already in place, which can be used to induce anaesthesia quickly when required.
Combination Anaesthesia
- Many anaesthetists recommend a combination of general and neuraxial anaesthesia for complex procedures such as Caesarean hysterectomy, allowing the mother to be awake for delivery and then receive GA for the remainder of the operation, with the epidural catheter used for post-operative analgesia.
- Similarly, for procedures like fetal surgery or other surgeries during pregnancy, combined GA and block is frequently used to provide optimal tocolysis with volatile anaesthetic agents.
- Modern GA drugs do not increase the risk of uterine atony post-delivery, but uterine tone should be monitored closely, and appropriate oxytocics administered as needed.
Acute Tocolysis
Tocolytic medications are covered in a different section, but during surgical deliveries and fetal operations, anesthetists may need to administer acute tocolysis. Among tocolytic agents, volatile anesthetic drugs are often regarded as the most effective for acute tocolysis.
- However, these drugs induce unconsciousness, resulting in general anesthesia.
- There are intravenous alternatives available that can be used in conjunction with regional anesthesia.
- These intravenous alternatives must be used with caution and proper monitoring to prevent cardiovascular collapse.
- For complex surgeries involving uterine manipulations, such as deliveries of conjoined twins or monoamniotic twins, general anesthesia along with optimal tocolysis is usually preferred.
Modern Obstetrics
- Contemporary obstetrics involves anesthetic procedures for the majority of parturients.
- Close collaboration, consultation, and planning, along with a minimal use of general anesthesia, have significantly decreased maternal and perinatal mortality and morbidity rates.
- This positive trend is anticipated to continue.
- All expectant mothers may require analgesia or anesthesia during the process.
- It is crucial to identify and address risk factors antenatally to uphold the impressive safety record of anesthesia in obstetrics.
FAQs on Chapter Notes: Analgesia and anaesthesia
| 1. What is the difference between obstetric analgesia and anaesthesia? |  |
| 2. Why is informed consent important for anaesthetic procedures? | |
| 3. What are the common techniques used for general anaesthesia? | |
| 4. What is acute tocolysis, and when is it used? | |
| 5. What are the potential risks and complications associated with anaesthesia during obstetric procedures? | |



