Chapter Notes: Puerperium and lactation


Introduction
- The puerperium is the period that begins after the delivery of the placenta and lasts until 6 to 12 weeks post-delivery.
- This phase is crucial for both the mother and the baby, yet it often receives less attention than pregnancy and childbirth. During the puerperium, the pelvic organs return to their pre-pregnancy state, the changes brought about by pregnancy are reversed, and breastfeeding is initiated.
- f breastfeeding does not take place, the reproductive cycle can resume within a few weeks.
- This period is also characterized by various cultural customs and rituals across the globe, with many medical guidelines rooted in these accepted traditions rather than scientific evidence.
- The puerperium is a time of significant psychological adjustment for mothers. While many visibly express joy at the arrival of their newborn, the transition to responsible parenting comes with concerns about the child's well-being, which can affect their coping ability. These worries may be exacerbated if the mother is fatigued from labor or experiences medical complications.
- Furthermore, new mothers often face an overwhelming influx of advice from healthcare professionals, family, and friends, which may conflict with their personal beliefs. Creating an environment that fosters confidence in mothers' abilities to care for their babies is essential.
- Support from midwives and obstetric staff plays a crucial role in establishing routines that will become integral to their lives.
Roles of Healthcare Providers
- During the early puerperium, obstetricians and midwives have several important responsibilities, including:
- Monitoring the physiological changes that occur during this period.
- Diagnosing and treating any postnatal complications that may arise.
- Helping establish infant feeding methods, such as breastfeeding or formula feeding.
- Providing emotional support to the mother as she adjusts to her new role.
- Offering advice on contraception and measures for ongoing health and well-being.
It is crucial to recognize that maternal death, although rare, can still occur during the puerperium, underscoring the importance of attentive care during this period.
Physiology of the Puerperium
During the puerperium, two main physiological changes occur:
- The establishment of lactation.
- The return of the body to its non-pregnant state after the physiological changes of pregnancy.
In the first two weeks after childbirth, these changes happen quickly, but some can take between 6 to 12 weeks to complete.
The Uterus
The weight of the uterus at full term is about 1000 g, while the non-pregnant uterus weighs between 50 g and 100 g. By six weeks after giving birth, the uterus returns to its normal size, and by ten days post-partum, the uterine fundus cannot be felt in the abdomen.
- After delivery, the cervix is very flaccid but returns to its normal state within a few days.
- The area where the placenta was attached is filled with granulocytes and mononuclear cells in the first three days after delivery, which extends into the endometrium and superficial myometrium.
- By the seventh day, the endometrial glands show signs of regeneration, and by day 16, the endometrium is fully restored.
- Decidual necrosis starts on the first day, and by day seven, there is a clear boundary between necrotic and healthy tissue.
- Mononuclear cells and lymphocytes are present for about ten days, likely serving as an antibacterial barrier.
- After birth, bleeding occurs due to the contraction of arterial smooth muscles and compression of blood vessels by the uterine muscles.
- In the first eight days, the vessels at the placental site show signs of:
- Thrombosis
- Hyalinization
- Obliterative fibrinoid endarteritis
- Initially, bleeding lasts a few hours and then quickly reduces to a red-brown discharge, known as lochia, by the third or fourth day post-partum.
- After that, it changes to a mucopurulent discharge that can sometimes have an unpleasant smell, referred to as lochia serosa, lasting on average 22-27 days. However, about 10-15% of women may experience lochia serosa for at least six weeks.
- Sometimes, there is a sudden but temporary increase in uterine bleeding between seven and fourteen days post-partum, which relates to the shedding of tissue over the placental site.
- This occurs because the myometrial blood vessels are still larger than normal, leading to significant bleeding, but this is usually self-limiting and subsides within 1 to 2 hours.
- A new endometrium will develop from the basal layers of the decidua.
- The uterine cavity can be lined with new endometrium within 3-4 weeks, but if lactation is established, the growth of the endometrium may be delayed for several months.
Ovarian Function
- Women who breastfeed their infants typically experience a prolonged period of amenorrhea, which usually lasts until the child is weaned.
- In women who do not breastfeed, ovulation can occur as early as 27 days after giving birth, but on average, it happens around 70 to 75 days later.
- For breastfeeding women, the average time to ovulation is approximately six months.
- About 70% of non-lactating women find that their menstruation returns by 12 weeks after giving birth.
- The average time until the first menstrual period after childbirth is between 7 and 9 weeks.
- The likelihood of ovulation within the first six months postpartum for women who exclusively breastfeed is between 1% and 5%.
Hormonal Factors
- The temporary suspension of ovulation following childbirth in breastfeeding women is primarily due to the sustained high levels of serum prolactin.
- In women who are not breastfeeding, prolactin levels return to normal by the third week after delivery.
- In breastfeeding women, prolactin levels remain elevated until about six weeks postpartum.
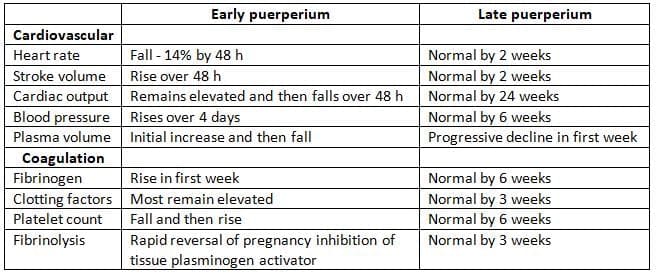
Cardiovascular and Coagulation System
- Changes take place in the cardiovascular and coagulation systems, which have practical and clinical implications.
- Heart rate and cardiac output decrease during the early puerperium, but there might be a temporary increase in stroke volume.
- Blood pressure increases during this period due to higher peripheral resistance, posing a high risk for mothers with heart disease, requiring closer monitoring.
- Although it is believed that a woman's body returns to the non-pregnant state by six weeks, cardiac output can remain elevated for up to 24 weeks postnatally.
- Fibrinolytic activity increases immediately after birth for 1-4 days, returning to normal within a week.
- Platelet counts may be normal during pregnancy, but there is a significant increase in platelets after delivery, raising the risk of thromboembolic disease.
Changes in the cardiovascular and coagulation systems during the puerperium:
Urinary Tract
- Mild Trauma: In the initial days following delivery, the bladder and urethra may experience mild trauma due to the birthing process.
- Localised Swelling: This trauma is often associated with localized swelling, known as edema.
- Temporary Changes: These changes are temporary and usually resolve quickly.
- Reversion to Normal: The alterations in the urinary tract that occur during pregnancy gradually fade away, similar to other bodily changes.
- Post-Delivery Recovery: Within 2-3 weeks after delivery, conditions such as hydroureter and kidney swelling begin to diminish. By 6 to 8 weeks post-delivery, the urinary tract typically returns to its normal state.
Weight loss
- After giving birth, there is an immediate weight loss of about 4.5 to 6 kg due to the expulsion of the placenta, amniotic fluid, and blood loss during delivery.
- By six weeks postpartum, approximately 28% of women will have returned to their pre-pregnancy weight.
- Women who did not gain excessive weight during pregnancy are expected to reach their normal weight by six months after giving birth.
- On the other hand, women who gained more than 15 kg during pregnancy may still have a net gain of 5 kg at six months postpartum, and this could persist indefinitely.
- Breastfeeding typically does not impact postpartum weight loss unless it continues for six months or more.
- While diet and exercise do not directly influence the growth of breastfed infants, maternal nutrition is crucial for the health of both mother and child.
- Women are encouraged to resume their normal activities while focusing on healthy weight management.
Thyroid Function
- Increase in Thyroid Volume: During pregnancy, the volume of the thyroid gland increases by approximately 30%.
- Return to Normal Size: This enlarged thyroid volume typically returns to normal within 12 weeks after childbirth.
- Hormone Levels Postpartum: Levels of thyroid hormones, specifically thyroxine (T4) and triiodothyronine (T3), normalize within 4 weeks after giving birth.
Hair Loss
Understanding Changes in Hair Growth
- Slowed Hair Growth: During the puerperium (the period after childbirth), hair growth tends to slow down.
- Temporary Hair Loss: Women may notice an increase in hair loss during this time, as more hair is shed temporarily compared to how much is being regrown.
- Duration for Normalcy: This condition is temporary, but it is important for women to understand that it usually takes between 6 months and 1 year for hair growth to return to normal levels.
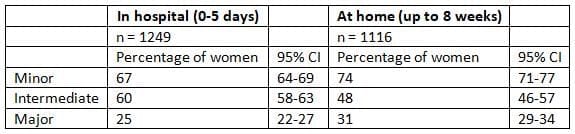
Management of Puerperium
The health concerns associated with the puerperium are frequently underestimated. A significant review (refer to Table) reveals that many mothers face substantial post-partum challenges. Approximately 31% of women reported experiencing major issues for up to 8 weeks following childbirth. To mitigate the impact of these health problems, several guiding principles for post-natal care should be considered:
- Continuity of care: The best care involves a consistent team from the antenatal period through childbirth and into the puerperium, allowing the mother to connect with a small group of health professionals.
- Mother/infant bonding: It's crucial for mothers and their partners to hold and touch their babies as soon as possible after delivery.
Health Issues Post-Childbirth
- Flexible discharge policies: The ideal length of stay after birth varies based on the needs of the mother and her baby. Some may choose home confinement or early discharge after 6 hours, while others may need more time, especially those with complicated deliveries or who want to establish breastfeeding. Current pressures on maternity services due to rising birth rates and limited resources often restrict this flexibility. While this has not significantly affected breastfeeding success, it may lead to increased psychological stress.
- Emotional and physical support: Mothers need support after childbirth, which can come from partners, family, and friends. Professional support and effective communication among hospital staff, community midwives, general practitioners, and health visitors are also essential.
Routine Observations After Childbirth
- During the patient's hospital stay, staff will regularly inquire about any complaints or concerns.
- Routine checks will be conducted on vital signs, including pulse, temperature, blood pressure, fundal height, and vaginal discharge following childbirth.
- If there is any trauma, the perineum will be examined daily.
- Surgical wounds, such as those from an episiotomy, will be monitored for signs of infection.
- It is crucial to ensure satisfactory urinary output and that the bladder is fully emptied.
- These observations are essential for providing early warnings of potential complications.
Ambulation in the Puerperium
- Early mobilization after childbirth is crucial.
- Once the mother has recovered from the physical challenges of labor, she is encouraged to start moving as soon as possible.
- The physiotherapist plays a vital role in assisting the patient in returning to normal health during the puerperium.
- Limb exercises are particularly important to promote venous flow in the leg veins of mothers who have been immobilized in bed for any reason.
- Exercises targeting the abdominal and pelvic floor muscles are valuable for restoring normal tone, which may have been lost during pregnancy.
Complications of the Puerperium
During the puerperium period, there is a risk of serious and potentially life-threatening complications.
The most severe among these complications include:
- Thromboembolism
- Infection
- Haemorrhage
- Mental Disorders
- Breast-Related Complications
Presents data on deaths caused by pulmonary embolism as reported by the Confidential Enquiry into Maternal and Child Health.

Thrombosis and Embolism
- According to the Confidential Enquiry into Maternal and Child Health conducted between 2000 and 2002, pulmonary embolism continues to be a major cause of death during the puerperium period.
- Out of 25 recorded deaths, 16 occurred in the post-natal phase.
- The data shows that the rate of pulmonary embolism as a cause of death has remained consistent since 1985.
- Three key factors that increase the risk of pulmonary embolism are:
- Increased maternal age
- A family history of thromboembolism
- Obesity, which is associated with reduced mobility
- Among the 16 deaths, 7 occurred within the first 7 days after delivery, 6 in the subsequent 2 weeks, and 3 after that period.
- Currently, prophylactic subcutaneous low molecular weight heparin is given only to women undergoing Caesarean sections.
- There is a need to also consider administering this treatment to women at higher risk after vaginal delivery.
Puerperal Infection
Puerperal pyrexia can result from various causes, but it is an important clinical sign that necessitates careful investigation. Infections can develop in different areas, and each must be assessed when a high temperature is observed.
Genital Tract Infection
- Genital tract infections continue to pose a serious risk to women's health.
- Over the past 17 years, the risks of puerperal sepsis and maternal death have been significant.
- The most dangerous organism is beta-haemolytic streptococcus, while more commonly, Chlamydia, Escherichia coli, and other gram-negative bacteria are the usual causes.
- Early diagnosis and treatment are crucial for improving patient outcomes.
Deaths from Puerperal Sepsis as Reported in Confidential Enquiry into Maternal and Child Health

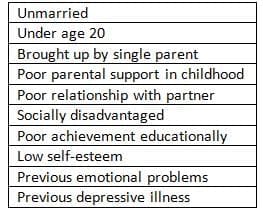
Risk factors for post-natal depression
- It is essential to prevent long-term complications of the five deaths reported between 2000 and 2002, four occurred in the community.
- Healthcare professionals caring for women after hospital discharge must be aware of the risks of puerperal sepsis and the need for prompt treatment.
Urinary Tract Infection
- Urinary tract infections (UTIs) are common during the puerperium for several reasons, including catheterization.
- Some women may experience urinary retention and require indwelling catheters.
- The most frequent pathogen involved in UTIs during this period is E. coli.
- Early treatment of UTIs is recommended.
Respiratory Infection
- Respiratory infections are currently less common during the puerperium because fewer women are receiving general anaesthesia for delivery.
- However, chest symptoms in postpartum women may indicate pulmonary embolism, so any woman presenting with chest issues should be evaluated for this condition.
Other Causes of Puerperal Pyrexia
- Surgical Wound Infection: After a Caesarean section, it's crucial to check for signs of infection in any surgical wound.
- Signs of Infection: Wound infection may present as a reddened and sore area beneath the incision, accompanied by surrounding swelling.
- Treatment Options:
- Contained Infection: May drain on its own.
- Abscess Formation: If an abscess forms, it may require surgical intervention to cut open and drain.
- Antibiotic Treatment: Broad-spectrum antibiotics are necessary, and samples should be sent for testing.
- Wound Resuturing: In some cases, re-suturing of wounds after infection is needed, but often they can heal from the bottom up.
- Legs Examination: If puerperal pyrexia is present, the legs should be checked for thrombophlebitis or deep venous thrombosis.
- Breasts Examination: The breasts should be examined for signs of infection, as breast abscesses can develop early, particularly with untreated mastitis, although this is rare before the fourteenth post-natal day.
Urination Complications
- Urinary retention is a common issue after childbirth, especially if there has been any injury to the urethra or swelling around the bladder neck.
- A painful episiotomy can make it difficult for women to urinate naturally, increasing the risk of urinary retention.
- Additionally, epidural anaesthesia can temporarily disrupt normal bladder sensations, leading to an overly full bladder.
Urinary Retention After Birth
- It is crucial to prevent urinary retention in the early post-natal period because an excessively full bladder can become atonic and fail to empty on its own.
- A distended bladder may be detectable in the abdomen. If it is not apparent or if there is uncertainty, an ultrasound scan should be performed to assess the urine volume in the bladder.
- Treatment for urinary retention involves the placement of an indwelling catheter for continuous drainage over 48 hours.
- Patients can move around during this period, and the catheter can be removed once the bladder has been emptied continuously.
- After catheter removal, the volume of urine passed should be monitored.
- If there are concerns about recurrent retention, a suprapubic catheter may be inserted for continuous drainage, followed by intermittent clamping until normal bladder function is restored.
Urinary Incontinence
- Urinary incontinence is a common issue for many women immediately after childbirth.
- Around 15% of women continue to experience urinary incontinence three months after giving birth.
- A study by Glazener and colleagues found that three-quarters of women who had urinary incontinence at three months postpartum still faced this issue six years later.
- Urinary incontinence is more likely to occur after instrumental deliveries and is less common following elective Caesarean sections.
- While urinary fistulae are uncommon in modern obstetric practice, injuries from obstetric forceps can happen occasionally.
- Complications involving the ureter are most often seen during complex Caesarean sections, where injuries can result in either a ureteric fistula or blockage.
- Women experiencing these urinary issues should be referred to a urological specialist for appropriate management.
Fecal Incontinence
- Recent studies show that 35% of women experience anal sphincter injury during their first vaginal delivery.
- About 10% of these women will continue to have anal symptoms such as urgency or incontinence three months after childbirth.
- A six-year follow-up study by Glazener et al. found no improvement in the rate of anal incontinence over time, with the rate increasing to 13% at six years.
- The causes of anal sphincter trauma and the mechanisms that maintain continence are complex and not fully understood.
- Instrumental delivery, particularly the use of forceps, is a known cause of anal sphincter trauma.
- Randomized trials have shown that using a vacuum extractor is associated with less perineal trauma compared to forceps delivery.
- The incidence of anal incontinence varies by the type of delivery:
- Forceps delivery: 32%
- Vacuum extraction: 16%
- The rates of third and fourth degree tears vary significantly between different medical centers, indicating that the ability to recognize this type of trauma may differ among practitioners.
- In women with a confirmed anal sphincter rupture, 37% continue to experience anal incontinence despite undergoing primary sphincter repair surgery.
Secondary Post-Partum Hemorrhage
- Secondary post-partum hemorrhage occurs in 1-2% of patients.
- This type of bleeding is most frequently seen between 8 and 14 days after childbirth.
- It typically results from the sloughing of the placental site.
- If the bleeding does not resolve on its own, further investigation is necessary.
- An ultrasound of the uterine cavity can usually indicate if there are significant retained products.
- Differentiating between a blood clot and retained placental tissue can be challenging.
- The preferred treatment is suction evacuation of the uterus.
- Antibiotic coverage is crucial if needed.
- If curettage is not immediately required to stop the bleeding, it is advisable to start antibiotics at least 12 hours before the procedure.
- This practice helps reduce the risk of endometritis, which can lead to uterine synechiae.
- A combination of metronidazole and Augmentin can be used for patients with endometritis without retained products.
- For individuals with retained products requiring curettage, intravenous antibiotics such as metronidazole combined with a cephalosporin or clindamycin are recommended.
- It is vital to exercise extreme caution during curettage, as an infected uterus is soft and susceptible to perforation.
- In rare instances where these methods fail to control the bleeding, embolization of the uterine arteries may be beneficial.
- Alternatively, using a Foley catheter balloon for uterine tamponade can be an effective approach.
Puerperal Psychological Disorders
- Mild Psychological Issues: It's common for new mothers to experience mild psychological issues and temporary depression in the first few days after childbirth.
- The Blues: This temporary state, characterized by feelings of being tearful, anxious, irritable, and restless, is often referred to as 'the blues.' It can affect up to 70% of women.
- Duration: The blues usually resolve by around day 10 after giving birth. It is likely linked to disrupted sleep and the stress of caring for a newborn.
- Hormonal Changes: The changes in steroid hormone levels that occur right after delivery are not connected to this brief depressive state.
- Treatment: Since it is a short-term issue, no treatment is generally required for the blues.
Post-Partum Depression
- Prevalence: Post-partum depression affects about 8-15% of women and can vary from mild to severe, with some cases leading to suicidal thoughts.
- Symptoms: The signs of post-natal depression are similar to those seen in non-pregnant women.
- Risk Factors: Certain factors present before giving birth can increase the likelihood of experiencing major post-partum depression.
- Recurrence: There is a high chance of recurrence in future pregnancies, estimated at around 50%.
- Delivery Method: The method of delivery is not associated with a higher risk of post-partum depression.
- Importance of Early Detection: Early detection and treatment of post-partum depression are crucial for a positive outcome, although symptoms can persist for up to a year.
- Diagnosis Challenges: Diagnosis can be delayed since this type of depression often occurs after the mother has returned home.
- Maternal Deaths: Alarmingly, suicide has become the leading cause of maternal deaths.
- Psychiatric Disorder-Related Deaths: From the Confidential Enquiry into Maternal and Child Health 2000-2002, there were 30 deaths in the post-natal period linked to psychiatric disorders.
- Methods of Death: These deaths resulted from methods such as hanging, jumping from heights, cutting the throat, or overdose.
- Risk Identification: Identifying at-risk patients during pregnancy is crucial to prevent post-partum depression.
- Communication Improvement: Better communication among hospitals, obstetricians, midwives, general practitioners (GPs), healthcare workers, and psychiatric services is necessary to reduce suicide rates associated with post-partum depression.
Post-natal Psychosis
- About 0.1% of women may experience signs of psychosis after childbirth.
- Post-partum psychosis is usually characterized by:
- Elevated levels of anxiety
- A combination of mania and depression
- Suicidal thoughts
- Delusions
- Impulses to self-harm or harm the baby
- Women showing symptoms of post-partum psychosis should be referred to a psychiatrist with compassion as soon as possible.
- They should be transferred to a mother and baby unit for appropriate care.
- If left untreated, there is a 5% risk of suicide and a 5% risk of infanticide.
Counselling of Patients after Perinatal Death
- Understanding Grief: When a woman and her family experience a loss related to pregnancy, it is crucial to pay attention to their grieving process.
- Mourning is an essential part of coping with such a loss. Healthcare professionals need to recognize the clinical signs and symptoms of grief to provide compassionatesupport.
- Sleeplessness
- Fatigue
- Poor eating habits
- Constant thoughts about the baby
- Feelings of guilt
- Hostility and anger
- Disruption to daily routines
- If clinicians fail to notice these changes, it can lead to misunderstandings and hinder their ability to assist with the grieving process. Families need someone who can listen and allow them to express and discuss their feelings openly.
- Professional Support: It is crucial to have trained professionals available to support families dealing with perinatal death. This includes doctors, midwives, and counselors who can provide the necessary emotional support and guidance.
- Legal and Administrative Assistance: In addition to emotional support, these professionals can help families navigate the legal and administrative tasks that arise following the death, alleviating some of their burdens during this difficult time.
- Ongoing Support: Support and counseling for these families may be required for several weeks or months after the event. It is essential to have suitable staff available to assist them during this extended period of grief.
Drugs During Lactation
- When a breastfeeding mother takes medications, these drugs can transfer to the infant through breast milk.
- Therefore, it is essential to evaluate whether specific medications could potentially affect the baby.
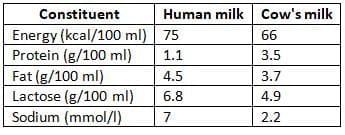
Comparison of Human and Cow's Milk Constituents
Infant Feeding
- The primary physiological change during the puerperium is the onset of lactation. In some developed countries, certain mothers choose artificial feeding over breastfeeding.
- However, there is increasing evidence highlighting the substantial short-term and long-term benefits of breastfeeding for both infants and mothers.
Advantages of breastfeeding
Nutritional Value of Breast Milk
- Breast milk changes over time, with colostrum being different from mature milk.
- The composition of milk can also change during a single feeding.
- Human milk has less protein but more fat and lactose compared to cow's milk.
- Breast milk contains important components like long-chain polyunsaturated fatty acids, which are vital for a baby's brain development.
- Experts generally agree that breast milk provides the best nutrition for infants.
Protection from Infections
- Breastfeeding offers significant protection to infants against infections, particularly in developing countries where diarrhoea is common.
- In developed countries, babies breastfed for at least 3 months experience lower rates of vomiting and diarrhoea compared to those fed from a bottle.
- Even after weaning, breastfed infants retain some protection against gastrointestinal problems.
- Breast milk contains lactoferrin, which binds iron and inhibits the growth of harmful bacteria such as E. coli.
- It also promotes the growth of beneficial gut bacteria that prevent harmful strains from proliferating.
- Bacteriocidal enzymes like lysozyme in breast milk enhance its protective properties.
- When a mother is exposed to a pathogen, her body produces specific immunoglobulin A antibodies that are transferred to her milk, providing targeted protection to the infant.
- This immunoglobulin helps the infant fight off common infections that the mother is immune to.
- Breast milk also contains live cells that may help in combating infections.
Breastfeeding and Brain Development
- Studies suggest that breastfeeding is associated with better cognitive development in children, including higher IQ scores.
- For instance, research has shown that children breastfed for more than 4 months scored 9.1 points higher on the Bayley scale at the age of 2.
- Preterm infants also experience improved neurological development when given breast milk.
- The exact reason for these benefits is not yet clear, but the presence of long-chain ω-3 fatty acids, such as docosahexaenoic acid, in breast milk may contribute to these positive outcomes.
 Pathways involved in the secretion of immunoglobulin A in breast milk by the Enteromammary circulation. (Courtesy of Professor R.V. Short, Melbourne, Australia)
Pathways involved in the secretion of immunoglobulin A in breast milk by the Enteromammary circulation. (Courtesy of Professor R.V. Short, Melbourne, Australia)
- Although diet influences the brain's composition, further research is needed to understand the relationship between brain fats and cognitive abilities.
Breastfeeding and Allergic Conditions
- Research indicates that infants who are breastfed have lower incidences of allergic conditions such as eczema and asthma.
- This protective effect is more significant in families with a history of allergic diseases.
- Allergic conditions are often associated with elevated levels of immunoglobulin E, particularly in relation to cow's milk protein.
Breastfeeding and Atopic illness
- According to Oddy et al. [22], a positive family history is important, but the timing of introducing weaning foods is even more crucial for atopic illnesses.
- They propose that the protective role of breastfeeding against these conditions might be secondary.
- This is because breastfeeding mothers typically introduce supplementary foods later.
- However, mothers with a family history of atopic illnesses should be informed about the advantages of breastfeeding and the potential risks of introducing supplements too early.
Breastfeeding and Disease in later life
- Breastfeeding may reduce the risk of juvenile-onset diabetes mellitus and neoplastic diseases in childhood.
- Some benefits might come from avoiding cow's milk early rather than breastfeeding itself. For example, early exposure to bovine serum albumin could trigger an autoimmune response leading to diabetes.
- Breast milk is crucial for preterm infants, helping to prevent necrotizing enterocolitis in these vulnerable babies.
Breast feeding and Breast Cancer
- There is an increasing incidence of breast cancer among women in developed countries.
- Recent research suggests that women who breastfeed their infants have a lower risk of developing breast cancer.
- While breastfeeding does not have a significant impact on postmenopausal breast cancer rates, it does offer some level of protection.
- Although this protective effect is small, it remains an important benefit against a common disease.
Breastfeeding and Fertility
- The natural contraceptive effects of breastfeeding are often overlooked in the Western world, where it is not considered a reliable family planning method.
- However, breastfeeding has a significant antifertility impact, particularly in developing countries. Many women in these regions depend on natural methods of contraception instead of artificial means.
- Breastfeeding typically lasts for 2 years or more in these areas, spacing births approximately every 3 years.
- In fact, breastfeeding in developing countries prevents more pregnancies than all other family planning methods combined.
- The declining rates of breastfeeding in these regions are concerning, as it may lead to increased population growth without improved use of contraceptive methods.
Breastfeeding and Obesity
- Children who are fed artificially have double the risk of childhood obesity compared to those who are breastfed.
- Breastfed children also tend to have lower blood pressure.
- These children are less likely to become obese in adulthood and have a reduced risk of dying prematurely from cardiovascular diseases.
Mechanisms of lactational Amenorrhoea
- The mechanisms behind lactational amenorrhoea are complex and not fully understood. The main factor is a change in the hypothalamus's response to ovarian steroids due to suckling.
- During lactation:
- The hypothalamus becomes more sensitive to negative feedback from oestrogen.
- This sensitivity means that when enough follicle-stimulating hormone and luteinizing hormone are released, oestrogen will inhibit gonadotrophin production, preventing follicle maturation.
- There is also a reduction in the normal release of luteinizing hormone during lactation, supporting this explanation.
Factors Influencing Lactational Amenorrhoea
- The primary factor influencing lactational amenorrhoea is the frequency and duration of suckling.
- Other factors, such as maternal weight and diet, may also play a role.
- If supplementary foods are introduced too early, the suckling stimulus will decrease, leading to early ovulation and a return to fertility.
Trends in Infant Feeding in the UK
- Breastfeeding offers numerous benefits, making it crucial for mothers to receive accurate information and support to breastfeed successfully whenever possible.
- Conversely, mothers who choose bottle feeding should be guided on best practices and supported in their decision.\
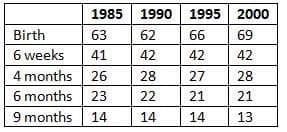
In the UK, approximately 69% of mothers initiate breastfeeding, but many discontinue after a short period. - The prevalence of breastfeeding in the UK in 2002, as , has not significantly changed over the past decade, although there is a slight increase in breastfeeding at birth.
- Factors associated with higher breastfeeding rates include:
- Higher social class
- Primiparity (first-time mothers)
- Older maternal age
- Geographical location: Mothers in the southern part of the country tend to have higher prevalence.
Prevalence of breastfeeding from birth until 9 months from 1985-2000
- To enhance these disappointingly low rates of successful breastfeeding, it is essential for health professionals to comprehend the physiology of lactation.
Physiology of Lactation
- At puberty, the milk ducts from the nipple to the secretory alveoli are stimulated by Oestrogen to sprout, branch, and form glandular tissue buds that develop into milk-secreting glands.
- During pregnancy, the breast tissue is further stimulated, causing existing alveolar-lobular structures to enlarge and new ones to form.
- Milk-collecting ducts also branch and grow during this time.
- Oestrogen and progesterone are essential for mammary development in pregnancy, along with prolactin, growth hormone, and adrenal steroids.
- In late pregnancy, only small amounts of milk are produced, despite high levels of lactogenic hormones like prolactin and placental lactogen.
- This limited milk production occurs because high levels of oestrogen and progesterone from the placenta inhibit the action of lactogenic hormones.
- Copious milk production begins only after delivery.
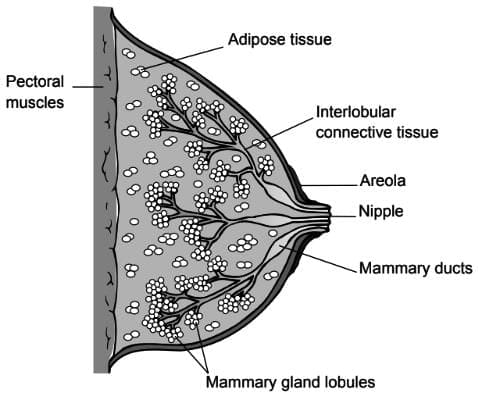
Structure of thelactating breast
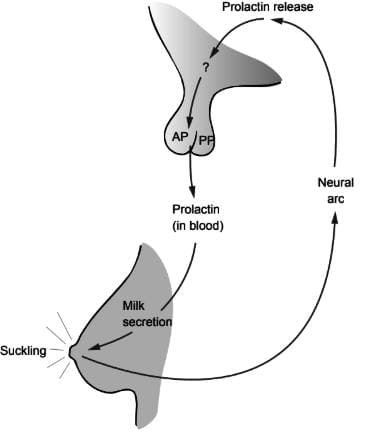
Pathway of prolactin release from the anterior pituitary gland
Milk Production
- Lactation involves two similar but independent mechanisms called lactogenesis.
- The first mechanism releases prolactin, which stimulates milk production in the glandular cells of the breast.
- The second mechanism releases oxytocin, triggering the milk ejection reflex by acting on the myoepithelial cells.
- Both mechanisms can be activated by suckling but operate through different neuroendocrine pathways.
- Suckling is crucial for lactogenesis, and the breast becomes more sensitive to this activity.
- During pregnancy, the areola skin is not very sensitive to touch but becomes more sensitive immediately after delivery.
- This change is important for sending enough neurological signals from the nipple to the hypothalamus.
These signals help maintain the release of prolactin and oxytocin, which are essential for successful lactation.
Milk-ejection Reflex
- Oxytocin plays a crucial role in the milk-ejection reflex, which is essential for successful breastfeeding.
- This reflex involves the transfer of milk from the breast to the baby and the production of sufficient milk.
- Oxytocin is released from the posterior pituitary gland and causes the contraction of special cells around the milk-producing glands. It also helps widen the ducts by acting on the muscle cells in the duct walls.
- Prolactin is released only when the baby suckles, while oxytocin can be triggered by sensory cues like seeing or hearing the baby.
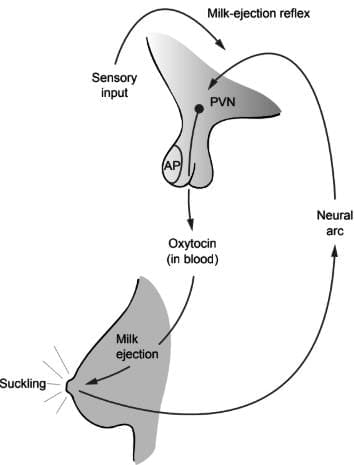
Pathway of oxytocin release from the posterior pituitary gland
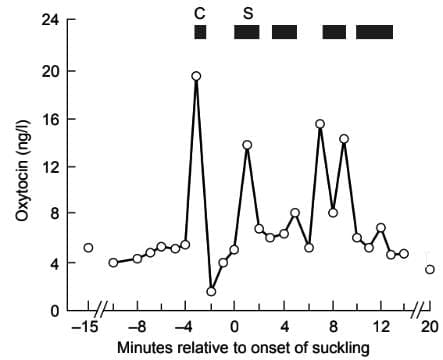
Pattern of oxytocin release in response to the infant's cry (C) and to suckling (S). Redrawn from McNeilly et al. (1982) with permission
- Oxytocin is released in bursts and has a short lifespan in the bloodstream.
- Emotional stress can inhibit the milk-ejection reflex, making it difficult for mothers to breastfeed.
- Boosting the mother's confidence and ensuring correct positioning and suckling at the breast are crucial for successful breastfeeding.
Volumes of Breast Milk
- Colostrum is produced in small amounts during the first 24 hours after birth, which is very nutritious, before transitioning to mature milk. With regular suckling, milk production increases gradually, and by day six, an average of 500 ml will be consumed by the baby.
- Once breastfeeding is fully established, mothers typically produce about 800 ml of milk daily.
- Well-established breastfeeding can sustain a baby on breast milk alone for 4-6 months.
Management of Breastfeeding
- Breastfeeding, while natural, can be challenging for many women at the outset. Support from an experienced and empathetic counsellor, whether a midwife, health visitor, or a caring friend, is crucial.
- Creating a calm and confident environment is vital for successful breastfeeding.
- Each baby is different, and there is no universal method; mothers should be encouraged to be responsive to their babies' individual needs. Unfortunately, mothers often receive mixed messages, which can be disheartening.
- The best approach is to offer mothers a range of options and allow them to make their own decisions, learning through experience what works best for their babies.
- To promote effective breastfeeding, the following practices are essential:
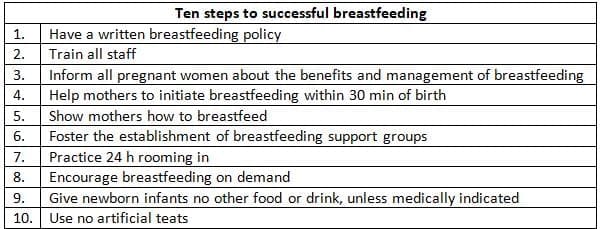
These practices are part of the UNICEF UK Baby Friendly Initiative and aim to create 'baby-friendly hospitals' where breastfeeding is a key focus.
FAQs on Chapter Notes: Puerperium and lactation
| 1. What physiological changes occur in the uterus during the puerperium? |  |
| 2. How does ovarian function change during the puerperium? | |
| 3. What urinary tract complications can arise during the puerperium? | |
| 4. What are the common causes and management of hair loss in the puerperium? | |
| 5. How can genital tract infections be prevented during the puerperium? | |



