Chapter Notes: Ectopic pregnancy


Introduction
- The first report of ectopic pregnancy in England came in 1731 from Gifford, who explained it as a pregnancy implanted outside the uterus cavity.
- Charles Meigs gave clear and detailed accounts of serious cases in the middle of the 1800s.
- It was viewed as uncommon but always leading to death.
- Improvements in surgery at the start of the 1900s made it possible to treat.
- It was still considered a major issue with many deaths until lately.
- Better ways to diagnose it without surgery in women with few signs have changed this view.
- The number of cases has gone up a lot in recent times.
- The death rate has dropped because of better early finding.
- Many more cases are now spotted due to better tests for pregnancy.
- In earlier times, a large number of these pregnancies ended on their own without being noticed.
- Today's medical ways make this less common.
- The rise in spotted cases can partly come from better screening methods.
- Several things raise a person's chance of this implantation.
- A link between older mothers and this pregnancy has been well noted.
Epidemiology and aetiology
- Over the last 30 years, the rate of ectopic pregnancy has risen a lot in most developed countries.
- The rate can be shown in different ways, like per number of births, pregnancies, or women who can have children.
- Because it's hard to record all pregnancies, often the number of women aged 15 to 44 is used to compare from different groups.
- Reported yearly rates vary between 100 and 175 per 1000 pregnancies.
- Rates are between 15 and 43 per 100000 women of child-bearing age.
- In recent years, rates have stayed the same or even dropped in some places like Sweden and Finland.
- In the UK, it has changed little in the last 10 years, with 9.6 per 1000 pregnancies in 1991 to 1993 and 11.0 per 1000 in 2000 to 2002.
- All ways to prevent pregnancy work well to lower both inside and outside uterus pregnancies.
- But when pregnancy happens despite prevention, the chance of it being outside is much higher after tube tying or while using IUD, but not with pill or barrier ways.
- Other linked things are past pelvic surgery, trouble getting pregnant, in utero DES contact, hard exercise, and smoking.
- The chance among black women and other minorities in the US is higher than for white women.
- In women with past ectopic, the chance of it happening again is 12 to 18 percent.
- The chance goes up more with each next time.
- The rate is three times more in women 35 to 44 years old compared to 15 to 24 years old.
- Lately, the age for first pregnancy has risen, which might add to the higher rate.
- The seen rise might also come from more risk things like infections spread by sex.
- A recent big study showed chances are much higher in women with past pelvic infection, many partners, and early start of intercourse.
- Chances are very high in women with past chlamydia infection.
- Another study from Sweden backs a link between this pregnancy and earlier chlamydia infection.
- Data showed a rise in this pregnancy came after a similar rise in acute salpingitis 15 years before.
- Lower rates of chlamydia from screening and treatment matched a drop in this pregnancy.
- But findings from these studies might be mixed up by other things and need careful reading.
- It might be that the time link between chlamydia infection and this pregnancy comes from changes in screening rules for chlamydia and ongoing better ways to spot this pregnancy.
Risk factors for ectopic pregnancy
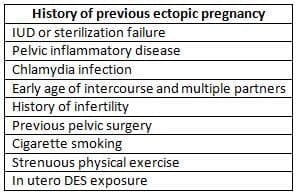
- Recently, rates stabilized or declined in places like Sweden and Finland.
- All contraception methods reduce intrauterine and extrauterine pregnancies.
- But if pregnancy occurs from failure, ectopic risk is higher after tubal sterilization or IUD use.
- Not higher with oral hormonal or barrier method failures.
- Other associated factors include previous pelvic surgery, infertility history, in utero DES exposure, strenuous exercise, and smoking.
- Risk is 1.6 times higher among black and ethnic minority women than white in US.
- In women with previous ectopic, recurrent risk is 12-18%.
- Risk increases with each successive occurrence.
Mortality
- Ectopic pregnancy is still a key reason for mother deaths around the world.
- Data from the US show the rate rose four times from 1972 to 1987.
- At the same time, deaths dropped nearly six times from 19.6 to 3.4 per 10000 cases.
- But the total deaths dropped less than half, from 47 to 30 per year.
- In the UK, both cases and deaths have stayed steady in the last 12 years, with death rate at 0.4 per 1000 guessed pregnancies.
- This has stayed the same despite big growth in services for women with suspected early pregnancy issues over the last 10 years.
- A possible reason is that women with the worst forms, like interstitial ones, have no signs until sudden break with big internal bleed.
- The lack of early signs stops women from seeking the half-elective services open to them.
Pathophysiology
- Any wrong in tube shape or work can lead to ectopic pregnancy.
- In normal pregnancy, the egg is fertilized in the Fallopian tube, then moved to the uterus.
- It is thought the main cause is damage to the tube lining, which can block the embryo move due to scars.
- Another chance is a small defect in the lining draws implantation there.
- The lining damage can come from infection or surgery hurt.
- But in many cases, no sign of tube damage is found.
- In these women, the cause might be wrong in the tube muscle action or odd signals from the endometrium.
- Thick move the embryo to the uterus cavity.
- This might explain higher rates after ovary over-stimulation and after-sex pill.
- On the other hand, drug doses of progesterone in women using only progesterone prevention can cause full tube relax, keeping the fertilized egg in the tube.
- Embryo wrongs have also been looked at to explain ectopics without tube issues.
- Though most tube pregnancies have normal genes, the rate of gene defects is higher than in inside uterus samples.
Clinical presentation
- The way ectopic pregnancy shows is very different and shows the growth potential of the pregnancy.
- This depends a lot on where it is in the tube.
- Generally, closer to uterus implantation allows more growth.
- Ampullary ectopics, which are 70 percent of all tube ones, rarely grow past very early stage.
- Signs can show as early as 5 weeks gestation.
- On the other hand, interstitial ones grow into pregnancies with live embryo seen on scan.
- These tend to have no signs until sudden break.
- Most ectopic pregnancies are a type of early pregnancy fail.
- Their main sign is usually brown vaginal discharge, which starts soon after missed period.
- However, the amount of bleed varies and in some women it can be quite heavy.
- Passage of a decid-ual cast may sometimes lead to wrong diagnosis of miscarriage.
- Abdominal pain is usually a late feature in the clinical show of ectopic pregnancy.
- The location of pain is not specific and it is not unusual for women to complain of pain on the side against the ectopic.
- Some women may complain of period-like pain or upper abdominal discomfort.
- The pain is usually caused by tubal miscarriage and bleeding through the fimbrial end of the tube into the belly cavity.
- The pain varies in strength and does not necessarily show the volume of blood lost from the tube.
- Most women with ectopic pregnancies show without bleeding.
- About 10 to 20 percent may complain of shoulder tip pain.
- In recent years, a big part of ectopic pregnancies are found before break.
- A workable embryo is spotted on scan, which raises the risk of break.
- Break tends to be more strong, with signs of peritonitis on belly palpation.
- Severe rupture sometimes presents with nausea, vomiting and diarrhea, which may confuse picture.
- Caused delay in the diagnosis was made in more than a third of women who have died from ectopic pregnancy in the United Kingdom since 1998.
- Similar to other types of ectopic pregnancy medical treatment with methotrexate or expectant management can be used in small viable ectopics.
- But the failure rates are very high and not specific, so they are not advised for pregnant women with viable ectopics.
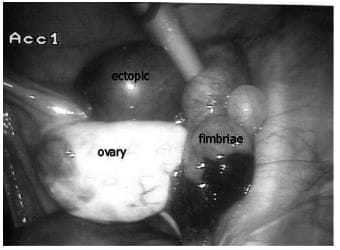
A laparoscopic image showing an isthmic tubal ectopic pregnancy with bleeding from the fimbrial end of the tube.
Diagnosis
Surgery
- Traditionally the diagnosis of ectopic pregnancy was made at surgery and then confirmed on histological examination following salpingectomy.
- At laparoscopy an unruptured ectopic pregnancy typically presents as a well-defined swelling in the Fallopian tube.
- The diagnosis may be difficult in the presence of extensive pelvic adhesions, which impact the visualization of the tubes.
- Anec dotal cases have false positive and false negative laparo-scopic findings.
- However, the accuracy of laparoscopic assessment of the pregnancy location has been published so far. Some authors have advocated the use of dilation and curettage in the diagnosis of ectopic pregnancy. The presence of chorionic villi helps to provide some reassurance since the incidence of heterotopic pregnancy is relatively low, but as men-tioned previously pregnancy a relatively low. But as men-tioned previously it does not exclude the possibility of heterotopic pregnancy.
- The clinical use of ultrasound for diagnosis of ectopic pregnancy started in the 1970s.
- It was first used to spot the lack of a gestational sac in the uterus when serum hCG was above a certain level.
- In view of this, the concept of discriminatory zone is of limited value in clinical practice and it is only useful in assessing asymptomatic women with uncertain menstrual dates.
- Abnormally slow rise in serum hCG has also been used to diagnose ectopic pregnancy.
- The doubling time in early pregnancy is 1.4 to 2.1 days, with the normal rise over 48 h being more than 66%.
- A slower rise is seen in 15% of normal intrauterine pregnancies and in 21% of ectopic pregnancies.
- The use of hCG to select patients for expectant, medi-cal and surgical management of ectopic pregnancy and to assess the efficacy of treatment at follow-up visits will be discussed later.
Ultrasound
- With the advent of diagnostic ultrasound and the increasing use of conservative treatment, the diagnosis of ectopic pregnancy is increasingly made without the help of surgery.
- The sensitivity of equipment will probably improve further in the future and it is imperative for modern practice to continue efforts to refine the selection criteria for expectant management of tubal ectopics.
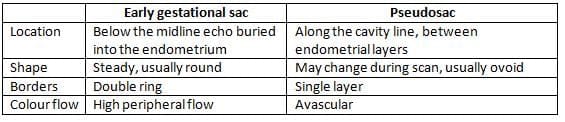
Differential diagnosis between early intrauterine gestational sac and Pseudosac
- An ultrasound equipment and the experience and skill of the operator. With the use of transabdominal ultra-sound, direct visualization of ectopic pregnancy is rarely possible.
- The only value of transabdominal ultrasound is therefore the detection of intraabdominal pregnancy in women with a clinical suspicion of ectopic. Even the diagnosis of intrauterine pregnancy is difficult to make with confidence until 6 to 7 weeks' gestation.
- In addition, it is almost impossible to differentiate between transabdomi-nal ectopics and intrauterine pregnancies on transabdominal scan.
- For these reasons transabdominal ultrasound should not be routinely used in women with a clinical suspicion of ectopic pregnancy.
- According to the current literature the success of expectant management may be determined by the serum hCG levels at the initial presentation.
- In general, if hCG is less than 1500 IU and the ectopic pregnancy is clearly visible on ultrasound scan, the addition of the serum progesterne enable further refinement in the prediction of the likely success of expectant management.
- Longterm follow up outcomes in women treated by conservative surgery or medically.
- Several studies have examined reproductive outcomes in women with ectopic pregnancies follow-ing successful expectant management compared to those who required surgery.
- Studies have found no significant differences in the intrauterine pregnancy rates and the rates of subsequent intrauterine and extrauterine pregnancies.
- The main advantage of expectant management is avoidance of any intervention, rather than an improvement in the reproductive outcomes.
Biochemical measurements
Serum Human Chorionic Gonadotropin
- Serum human chorionic gonadotropin (hCG) measure-ments have traditionally been used as a secondary investigation in women with suspected ectopic pregnancy in whom ultrasound examination has failed to identify an
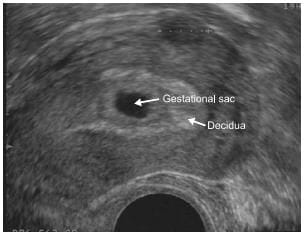
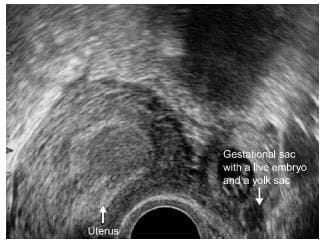
A longitudinal section through the uterus showing a normal early intrauterine pregnancy at 5 weeks' gestation. The sac is surrounded by a well-defined layer of trophoblast tissue and thick decidua.
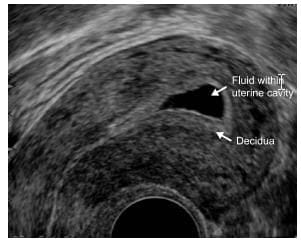
Uterine cavity expanded with fluid mimicking an intrauterine
- This is clearly not the case in a complete miscarriage because of its long clearance time of 24-36 h.
- It has also been shown that more than 50% of ectopics, which are detectable on the scan, present with hCG levels <1000 IU/l.
- Gentle pressure applied with the tip of the probe may be used to see whether the suspected tubal ectopic moves separately from the ovary. This slid-ing organs sign helps to avoid false positive diagnosis of ectopic pregnancy.
- Intrauterine or ectopic pregnancy.
- With the use of transabdominal ultrasound, a normal intrauterine pregnancy can be delayed for a few weeks until the fetus reaches viability.
- Avoiding disruption of the placenta. The fetus should be removed, the cord cut short and the placenta should be left in situ. Any attempt to remove the placenta may result in uncontrollable haemorrhage.
- Adjuvant treat-ment with methotrexate is not necessary and the residual placental tissue will absorb slowly over a period of many months, sometimes a year. The placental tissue left in situ may become infected leading to the formation of a pelvic abscess, which may require drainage.
Management
Surgery
- Surgery has been traditionally used both for the diag-nosis and treatment of ectopic pregnancy. In the second half of the twentieth century laparoscopy was mostly used as a diagnostic tool and open surgery was used to treat ectopic pregnancy.
- With recent advances in operative laparoscopy, the minimally invasive approach has also been accepted as the method of choice to treat most tubal ectopics in haemodynamically stable women.
- There are important advan-tages of laparoscopic over open surgery which include less post-operative pain, shorter hospital stay and faster resumption of social activity [30].
- However, the future reproductive outcomes following laparoscopic or open surgery are not significantly different. Although the rate of recurrent ectopic is slightly lower following laparoscopic surgery, the rates of subsequent intrauterine pregnancies appear to be similar [31].
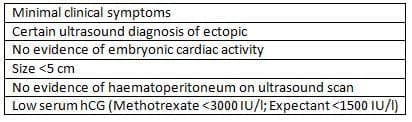
- Selection criteria for treatment with methotrexate are almost identical to those used for expectant manage-ment (Table 14.3) which was established for RCOG.
- The most important criteria are size of the ectopic <3.5 cm and serum hCG between 1000 and 5000 IU/l, with methotrexate is the risk of tubal rupture and blood transfusion, which occurred significantly more often in women receiving methotrexate compared to those who underwent surgery [32].
- In view of this, the overall role of methotrexate in the management of ectopic pregnancy is limited, but it may be offered on an individual basis to highly motivated women with small unruptured ectopics and a serum hCG level <3000 IU/l, who are likely to comply with well-organized follow-up.
Medical management
- Medical management of ectopic pregnancy has grown in popularity in recent years following several observational studies which reported success rates with a single dose systemic methotrexate in excess of 90% [33]. However, the diagnosis of ectopic pregnancy was based in many cases on non-specific ultrasound findings of serum hCG, rather than on direct visualization of ectopic on ultrasound scan or at laparoscopy. It is therefore possible that a significant number of cases intrauterine miscar-riages were misdiagnosed as ectopics, contributing to the high success rates. Nevertheless there are some obvious attractions of medical treatment such as the possibility
Selection criteria for conservative management of ectopic pregnancy
- to manage patients on an outpatient basis and avoidance of surgery. However, due to the need for prolonged fol-low up and increased failure rate in women presenting with higher initial hCG measurements, medical treat-ment is only cost effective in ectopics with serum hCG <1500 IU [34].
- Selection criteria for treatment with methotrexate are usually strict and they are listed in Table 14.3. Two ran-domized trials which compared methotrexate to surgery showed that only one third of all tubal ectopics satis-fied these criteria and were suitable for medical treatment with the success rates between 65 and 82% [35,36]. The overall contribution of methotrexate to successful treat-ment of tubal ectopic was between 25 and 30% while with methotrexate is the risk of tubal rupture and blood transfusion, which occurred significantly more often in women receiving methotrexate compared to those who underwent surgery [32].
- Follow up [35]. There is a role of side effects such as gastronomic, stomatitis, headache, nausea, sus-e leukopenia or thrombocytopenia may also occur.
- In view of this, the overall role of methotrexate in the management of ectopic pregnancy is limited, but it may be offered on an individual basis to highly motivated women with small unruptured ectopics and a serum hCG level <3000 IU/l, who are likely to comply with well-organized follow-up.
Expectant management
- Expectant management has important advantages over medical treatment as it follows the natural history of the disease and is free from serious side effects of methotrex-ate. The progress of ectopic pregnancy is easier to mon-itor as serum hCG measurements accurately reflect tro-phoblastic activity of the ectopic pregnancy with rising levels indicating an increased risk of rupture. This is dif-ferent from medical treatment, which is characterized by an initial rise in serum hCG following administration of
- methotrexate in cases with both successful and unsuccess-ful outcomes. Therefore medical treatment is often impossible to be confident about the probability of success-ful treatment for up to a week following injection, which increases the risk of adverse outcomes in comparison to expectant management.
- Expectant management requires prolonged follow up and it may cause anxiety to both women and their carers. However, the main limiting factor in the use of expec-tant management is the relatively high failure rate and the inability to identify with accuracy the cases that are likely to fail expectant management. To minimize the risk of failure many authors have used very strict selec-tion criteria for expectant management such as the initial hCG <25%. Recent studies showed that man-agement up to 40% of all tubal ectopics may resolve spontaneously on expectant treatment [40]. This obser-vation also reflects the increased sensitivity of modern ultrasound equipment, which enables detection of very small ectopics.
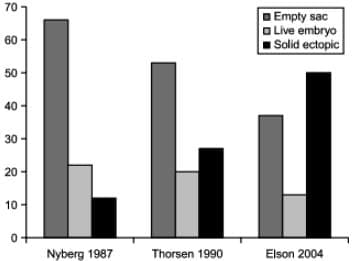
Relative frequencies of various morphological types of ectopic pregnancies identified on ultrasound scans over the past two decades. The proportion of more severe cases, such as live ectopics and well-formed gestational sacs, is decreasing, while the proportion of milder forms, like small solid ectopics, is increasing. This trend reflects the enhanced capability of modern equipment to detect tubal ectopics, rather than a change in the nature of the condition.
- It is very likely that a large pro-portion of these small ectopics were undiagnosed in the past and treated as early intrauterine miscarriages. How-ever, the sensitivity of equipment will probably improve further in the future and it is imperative for modern prac-tice to continue efforts to refine the selection criteria for expectant management of tubal ectopics.
- According to the current literature the success of expec-tant management may be determined by the serum hCG levels at the initial presentation. In general, if hCG is less than 1500 IU and the ectopic pregnancy is clearly visible on ultrasound scan, the addition of the serum progesterone and morphological features of ectopics on ultrasound scan enable further refinement in the prediction of the likely success of expectant management.
- Long-term follow up outcomes in women treated by conservative surgery or medically. Several studies have examined reproductive outcomes in women with ectopic pregnancies follow-ing successful expectant management compared to those who required surgery.
- Studies have found no significant differ-ences in the intrauterine pregnancy rates and the rates of subsequent intrauterine and extrauterine pregnancies.
- The main advantage of expectant manage-ment is avoidance of any intervention, rather than an improvement in the reproductive outcomes.
Fertility after ectopic pregnancy
- Intrauterine pregnancy rates following ectopic pregnancy range between 50 and 70% [41]. Recurrent ectop-ics occur in 6-16% of women with previous history of ectomics [42] and those women should be offered early scans in all future pregnancies to detect recurrent ectopics before complications can occur.
Non-tubal ectopics
Interstitial ectopics
- The implantation of the conceptus in the proximal portion of the Fallopian tube, which is within the muscular wall of the uterus, is called an interstitial pregnancy.
- The inci-dence of interstitial pregnancy is 1 in 2500-5000 live births and it accounts for 2-6% of all ectopic pregnancies [43].
- Risk factors predisposing to an interstitial pregnancy are the same as those for tubal ectopics and include previous ectopic pregnancy, previous salpingectomy, IVF and sexually transmitted infections [25%].
- A unique predisposing factor to interstitial pregnancy is previous ipsilateral salpingectomy.
- The maternal mortality associated with interstitial pregnancy is still high and the overall mortality rate of this form of ectopic pregnancy is about 2-2.5% [21].
Interstitial pregnancy
- Interstitial pregnancy remains the most difficult type of ectopic pregnancy to diagnose pre-operatively. This is partly due to lack of any symptoms prior to sudden rupture. In modern clinical practice the diagnosis of inter-stitial pregnancy should be made non-invasively using transvaginal ultrasound.
- The diagnosis is based on the visualization of the interstitial tube adjoining the lateral aspect of the uterine cavity and the gestational sac, the presence of a continuous myometrial layer surrounding the chorionic sac [45] .
- Ruptured interstitial pregnancy usually presents dra-matically with severe intra-abdominal bleeding, which requires urgent surgery. Haemostasis can usually be achieved by removing the pregnancy tissue and suturing the rupture site.
- However, in cases of extreme bleeding a cornual resection or in rare cases a hysterectomy may be necessary to arrest the bleeding.
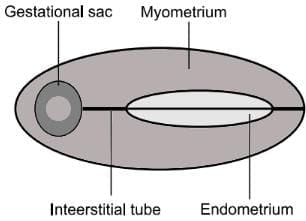
Schematic illustration of Interstitial Pregnancy
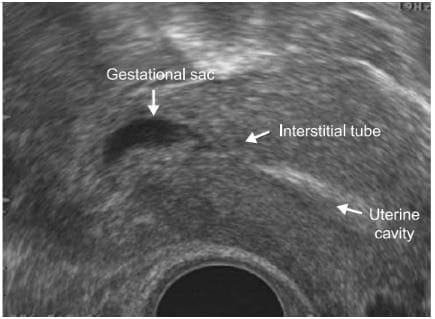
An angled view through the uterus revealing an empty uterine cavity and the interstitial segment of the tube adjacent to an ectopic sac. The sac is entirely enclosed by a myometrial layer, which is characteristic of an interstitial pregnancy.
- Unruptured interstitial pregnancy <12 weeks in size can be managed conservatively. Medical treatment with methotrex ate should be given to all women with ris-ing serum hCG on follow-up visit. Good results have been reported with both systemic and local methotrexate [46,47]. However, in viable interstitial pregnancies local injection under ultrasound guidance is preferable as it enables fetocide to be carried out at the same time, which increases the success rate of medical treatment. Small interstitial pregnancies with declining serum hCG levels can be managed expectantly without any intervention.
- Apart from the side effects of methotrexate, the main disadvantage of conservative treatment is the time taken for the pregnancy to be fully absorbed and in larger pregnancies this may take up to a year.
Pregnancies located below the internal os - cervical and Caesarean scar pregnancies
- Cervical pregnancy is defined as the implantation of the conceptus within the cervix, below the level of the internal os. Caesarean scar pregnancy is a novel entity, which refers to a pregnancy implanted into a deficient uterine scar fol-lowing previous lower segment Caesarean section [48].
- Prior to the introduction of high resolution transvaginal scanning, the distinction between cervical and Caesarean section scar pregnancies was not possible. In older litera-ture 33% of 'cervical' pregnancies occurred in women with a history of previous Caesarean section, which indicates that scar pregnancies probably account for a significant number of ectopics below the level of the internal os [49].
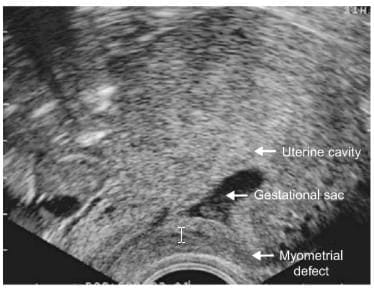
- The common characteristic of both cervical and Caesa-rean scar pregnancies is their implantation into myome-trial defects following previous intrauterine surgery . In case of cervical pregnancy the implantation
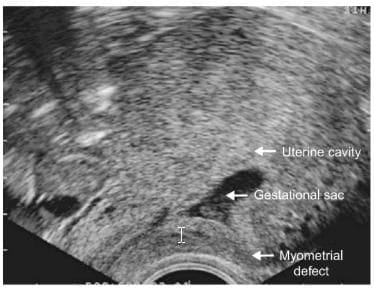
A clear anterior myometrial defect is evident after the removal of a Caesarean pregnancy.
- The risk of recurrence of cervical/Caesarean ectopic is low, and provided the next pregnancy is located normally within the uterine cavity, it is likely to be uncomplicated.
Ovarian pregnancy
- Ovarian pregnancy is defined as the implantation of the conceptus on the surface of the ovary or inside the ovary, away from the Fallopian tubes. There are no direct risk factors associated with primary ovarian pregnancy. The role of IUCD as a direct risk factor for ovarian pregnancy is unclear [53]. The role of pelvic inflammatory disease and assisted reproduction as predisposing factors is also not clear. Chance might also have played a role in some cases, as recurrent cases of ovarian pregnancy have rarely been reported.
- The diagnosis of ovarian pregnancy is rarely achieved pre-operatively; most cases are treated surgi-cally as the diagnosis is usually made only at operation [54]. On ultrasound scan the ovarian wall can be seen implanted into the ovary next to the corpus luteum.
- Laparoscopy has emerged as the gold standard method for the management of most ovarian pregnancies. The technique of laparoscopic removal depends on the size and location of the pregnancy status. Conservative laparo-scopic surgery involves ovarian resection or aspiration of the pregnancy combined with coagulation of the implanta-tion site using thermocoagulator [55]. However, in cases with profuse intraoperative bleeding an oophorectomy or salpingo-oophorectomy may be necessary to achieve haemostasis.
An instance of ovarian pregnancy identified via ultrasound scan. The gestational sac, featuring a prominent trophoblastic ring, is located to the side of a cystic corpus luteum.
Abdominal pregnancy
- Abdominal pregnancy is a rarity that only a few gynaecologists will encounter during their professional career. Most abdominal pregnancies are the result of re-implantation of ruptured undiagnosed tubal ectopic preg-nancies. With the increasing accuracy of first-trimester transvaginal ultrasound. The diagnosis is based on the advanced abdominal pregnancy will decrease even fur-ther in the future. The clinical and ultrasound features of an early abdominal pregnancy are very similar to tubal ectopics, which progress beyond the first trimester, are typically missed on routine transabdominal scanning.
- Abdominal pregnancy should be suspected in women in those who complain of painful fetal movements. In the growth restriction (IUGR). Perinatal mortality is high (>40%) and the incidence of fetal malformations is also increased [56].
- In women with a clinical suspicion of abdominal preg-nancy a transvaginal scan should be performed between the internal ostium the contrary between the ovari-es to establish the continuity between the cervi-cal canal, uterine cavity and the differential diag-nostic includes abdominal pregnancy and pregnancy in an atretic non-communicating cornu of a unicornuate uterus.
- The visualization of both ovaries separate from the tubes The diagnosis of abdominal pregnancy is surgical. The tim-ing of the intervention depends on clinical signs and patient's symptoms. In advanced abdominal pregnancies the late second trimester termination of pregnancy may be delayed for a few weeks until the fetus reaches viability.
- Avoiding disruption of the placenta. The fetus should be removed, the cord cut short and the placenta should be left in situ. Any attempt to remove the placenta may result in uncontrollable haemorrhage. Adjuvant treat-ment with methotrexate is not necessary and the residual placental tissue will absorb slowly over a period of many months, sometimes a year. The placental tissue left in situ may become infected leading to the formation of a pelvic abscess, which may require drainage.
FAQs on Chapter Notes: Ectopic pregnancy
| 1. What is human chorionic gonadotropin (hCG) and its role in detecting ectopic pregnancy? |  |
| 2. What are the common symptoms of an ectopic pregnancy? | |
| 3. How is an ectopic pregnancy diagnosed? | |
| 4. What treatment options are available for an ectopic pregnancy? | |
| 5. What are the potential risks and complications associated with an ectopic pregnancy? | |



