Chapter Notes: Malpresentation, malposition, cephalopelvic disproportion and obstetric procedures

Malpresentation and Malposition
Introduction and definitions
- The lowest part of the fetus that reaches the lower uterine segment and cervix is called the presentation.
- Around 95% of fetuses at term show the vertex in labor, which is known as normal presentation.
- The vertex is shaped like a diamond, marked by the two parietal eminences, the anterior fontanelle, and the posterior fontanelle.
- When the presentation is not the vertex, such as breech, brow, face, or shoulder, it is called malpresentation.
- The exact cause for malpresentations is unknown in most cases.
- Malpresentations can be linked to a contracted pelvis, large baby, too much amniotic fluid, multiple pregnancies, placenta low in the uterus, early labor, fetal abnormalities like neck tumors, uterine issues that are congenital or acquired such as lower segment fibroids, or pelvic problems.
- Position refers to how the denominator of the presenting part relates to fixed points in the mother's pelvis.
- The fixed points in the pelvis include the sacrum at the back, sacro-iliac joints at the back sides, ileo-pectineal eminences at the front sides, and symphysis pubis at the front.
- The denominator is the clearest outer point in the presenting part, like the occiput for vertex, mentum for face, and sacrum for breech.
- Malposition mostly applies to vertex presentations, which are normal.
- The vertex is in occipito-anterior position (right, left, or direct) in about 90% of cases by the late first stage of labor at term, and this is normal position.
- In these cases, the head is fully flexed, showing the smallest front-to-back diameter called suboccipito-bregmatic and side-to-side biparietal diameter, both 9.5 cm by 9.5 cm, with parietal eminences at equal levels in the pelvis, known as synclitism.
- If the occiput is in the back half of the pelvis, it is malposition.
- These often show a slightly extended head with a larger front-to-back diameter called occipito-frontal of 11.5 cm.
- They can also have anterior or posterior asynclitism, where one parietal eminence is in the front half of the pelvis and lower for anterior asynclitism, or the opposite for posterior.
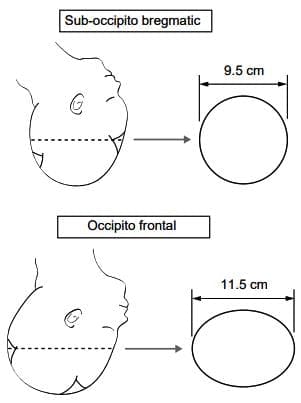
Anteroposterior diameters of the vertex in the well-flexed head (suboccipito-bregmatic - usually OA positions) and slightly deflexed head (occipito-frontal - usually occipito-posterior or transverse positions).
- When the sagittal suture shifts more to the back or front due to head extension with asynclitism, it presents a larger diameter, leading to longer, harder labors and more deliveries needing help.
- Most malpositions fix themselves to normal position because the head flexes at the atlanto-occipital joint, and the occiput turns forward with more uterine contractions.
- This happens from the push of the fetal spine on one side of the oval head, which rests on the downward-sloping pelvic floor muscles called levator ani.
- This natural labor process helps in spontaneous vaginal births.
- Show the Image front-to-back diameters of the vertex in a well-flexed head (suboccipito-bregmatic, usually occipito-anterior positions) and slightly deflexed head (occipito-frontal, usually occipito-posterior or transverse positions). Reproduced from the 1st edition of Dewhurst's textbook of Obstetrics and Gynaecology for Postgraduates.
- Show the Image posterior asynclitism of the vertex, where the posterior parietal bone is prominent and the sagittal suture is shifted much anterior in the pelvis.
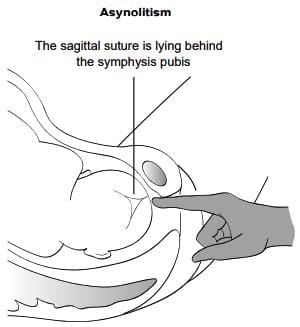
Posterior asynclitism of the vertex - posterior parietal bone is prominent and the sagital suture is shifted much anterior in the pelvis.
Malpresentation (breech, face, brow, shoulder) in labour
Breech presentation
- The rate of breech changes with gestation: 40% at 20 weeks, 6-8% at 34 weeks, and 3-4% at term.
- In most breech cases, there is no clear reason for the fetus presenting by breech.
- It is helpful to check for factors that lead to breech, and ultrasound helps with this.
- Causes include bicornuate uterus, uterine fibroid, low-lying placenta, multiple pregnancies, too much or too little amniotic fluid.
- Rarely, breech can be from congenital issues like spina bifida or hydrocephaly.
Identification of breech presentation
- Breech often presents with hips flexed and knees extended, called extended breech.
- Next common is hips and knees both flexed, called flexed or complete breech.
- Sometimes one leg flexed and the other extended, called incomplete breech.
- Rarely, one or both feet present, called footling breech, or it can be knee presentation.
- Show the Image types of breech presentation: flexed breech, footling presentation, extended (frank) breech.
- Because the breech does not fit well in the pelvis, there is higher chance of cord prolapse, up to 10% in footling.
- With careful feeling during antenatal checks, breech is found.
- It is easier to find as gestation increases, or if the mother has had babies before or has a thin belly.
- The fetus is lengthwise, with head as a round hard mass in the upper part, usually to one side under the hypochondrium, tender on deep press.
- The breech, which is wider, is felt above or in the pelvis.
- When breech is extended, head is hard to identify.
- Easier in early gestation as head can be bounced.
- If extended breech in pelvis, hard to tell from deeply engaged head.
- Ultrasound or vaginal exam helps identify engaged head.
- On listening with stethoscope, fetal heart is above umbilicus, but Doptone can pick it below, so deceptive.
Antenatal management
- Higher perinatal death and injury with breech is known.
- With routine prenatal checks, congenital issues are rarer cause, leaving early birth, birth lack of oxygen from cord issues, and trauma as main causes.
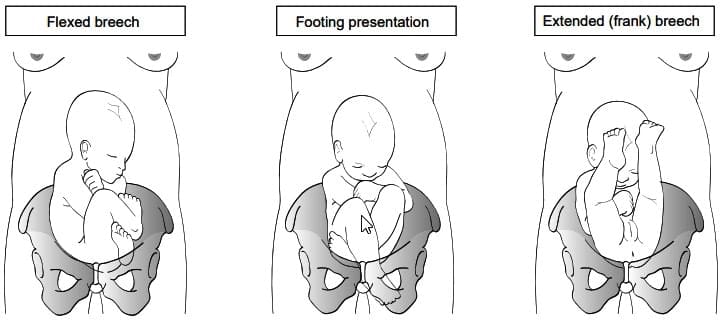
Types of breech presentation
- Current studies suggest planned C-section for term breeches.
- Training in assisted vaginal delivery needed as some mothers choose it.
- Study did not cover those in full labor with breech, preterm breeches, or breech in multiples.
- Evidence shows breech may indicate underlying issue, and delivery mode may not change outcome.
- Most cases have no major abnormality, so delivery as head first or planned C-section may lower injury and death from assisted breech delivery.
- External cephalic version, ECV, offered after 36+ weeks as chance of spontaneous turn from breech to head after 37 weeks is 1 in 20.
- Couple needs full counseling on success rates, risks, and procedure details.
- ECV not done in placenta praevia, multiples, bleeding before birth, growth restriction, preeclampsia or high blood pressure.
- ECV is somewhat not advised for those with uterine scars.
- ECV only in place where urgent C-section possible if fetal issue during or after ECV.
- Done in delivery room after scan confirms breech, notes fetal back side, breech type, fetal posture, placenta position, amniotic fluid amount.
- CTG 20-30 min before ECV should show no low oxygen in fetus.
- Multiple births before, flexed breech, enough fluid, breech mobile above brim increase success chance.
- Mother in Trendelenburg position, IV fluids before to possibly increase fluid, sound stimulation, short tocolytic for uterus relax suggested to raise success.
- Forward or backward flip practiced after lifting breech and shifting to opposite side where head moved, then head to lower part.
- Average success about 60% in women with prior births, under 40% in first-time mothers.
- Risks include cord issues, membrane break before labor, blood transfer between fetus and mother, placenta detach, fetal issue or death.
- If mother Rhesus negative, anti-D given after ECV try, Kleihauer-Betke test to check dose enough.
- CTG after ECV for 30-40 min should show normal reactive trace, no uterus irritation.
- No bleeding, fluid leak from vagina, or uterus pain before sending home.
- If ECV fails, counsel on planned C-section or assisted vaginal breech delivery.
Intrapartum management
- Careful choice for assisted vaginal delivery key for best result.
- Frank and complete breech with fetal weight under 4000 g preferred, footling advised on higher cord prolapse chance.
- Pelvis size should be sure, clinical check enough, no proof CT or X-ray pelvimetry helps success.
- Natural labor start preferred.
- Starting labor with breech only in chosen cases, as C-section may be better than starting.
- Mothers told to come to unit when membranes break or painful contractions start.
- Check no cord presentation or prolapse on arrival.
- Labor handled like vertex.
- Cervix dilatation rate, breech descent, fetal heart pattern guide labor.
- If progress poor, check uterine contractions strength.
- Short oxytocin boost useful and safe in chosen cases.
- If poor progress in first few hours of boost, better choose C-section.
- Second stage needs full mother cooperation and help, so epidural for pain and second stage management suggested.
- In most breech, early push feeling, so check cervix dilatation, encourage push only when breech at perineal phase of second stage.
- Key not to act early, lithotomy only after front buttock and anus visible over perineum with no pull back between contractions.
- Episiotomy not needed in multipara with stretchy perineum, but helpful in first-time mother.
- Done with regional block or pudendal block and local perineum infiltration.
- Usually fetus comes out in sacro-lateral position.
- Mother encouraged to push with contractions to deliver unhelped up to umbilicus.
- Help for breech as side move with pull only for head delivery.
- In extended knees (frank breech), legs delivered by slight thigh out and knee bend.
- Show the Image delivery of extended legs by slight thigh abduction and knee flexion.
- Body kept with back up ideally.
- When scapulae seen, if arms flexed, forearms delivered by sweeping front of fetal chest.
- If arms extended, shoulder in and down then elbow out to bring forearm and hand down.
- If not possible, Lovset manoeuvre: posterior shoulder below sacral promontory brought front below symphysis pubis by turning fetus clockwise holding with thumbs on sacrum and index on anterior superior iliac spines.
- Show the Image delivery of arm by body rotation so posterior shoulder below sacral promontory becomes anterior and below pubic symphysis.
- After shoulder delivery that came front, fetus turned anticlockwise for opposite shoulder descent.
- After shoulder delivery, fetus back should face front, on vaginal exam chin faces sacrum.
- Head descent helped by fetus weight, gently held till neck nape under symphysis pubis.
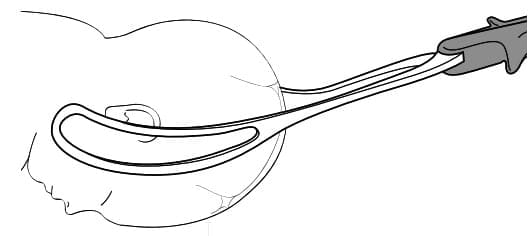
- This means head low in pelvis, delivered by one of three ways: (1) Swing trunk to mother's belly till fetus mouth and nose visible; (2) Mauriceau-Smellie Veit manoeuvre with two fingers on maxilla to flex head, delivery by shoulder pull; (3) Piper or Neville Barnes Forceps applied from below while assistant holds baby below horizontal, pull applied.
- Show the Image head delivery by jaw flexion and shoulder traction.
- After any method, head delivery finished after sucking oro-pharynx then nasopharynx, and stretching perineum beyond forehead.
Conclusion
- Current proof supports planned C-section for term breech.
- Not enough proof for mode in preterm breeches.
- Injury and death may be more from gestation and birthweight estimate than delivery mode.
- Key to have detailed talk with parents and pediatricians for informed choice on delivery mode.
- Some mothers want assisted vaginal breech delivery, others come in advanced labor.
- Their wishes and needs should be met.
- Skills gained by helping others, practicing assisted breech at C-section, on models.
- Having experienced person reassures new doctor and couple.
Brow presentation
- In brow, head half extended, presents largest front-to-back diameter (mento-vertical, 13 cm).
- Lowest head part felt on vaginal exam is forehead, but called brow as orbital ridges and nose bridge most clear.
- Rate rare, about 1 in 1500-3000 births.
- May fix in labor by flexing to vertex or extend more to face, lead to vaginal birth.
- Lasting brow at term not for vaginal birth, needs C-section.
- In early labor, prepare for C-section, wait to see if flex or extend.
- No progress in next few hours with lasting brow means C-section, not oxytocin boost.
- In very early preterm, fetus may descend as brow, deliver as brow or change to face or vertex on pelvic floor.
- Though vaginal possible in preterm, spinal cord damage risk, C-section preferred.
- Labor issues include cord prolapse with membrane break, rare uterus rupture if ignored.
- In fetal death inside or lethal issue in very preterm, where fetal injury not concern, allow labor if good progress for vaginal birth.
- At term, destructive actions and vaginal possible for fetal death or lethal anomaly, but C-section preferred in developed places for fear of birth tract injury by those not familiar.
Face presentation
- Face happens in about 1:500 to 1000 births.
- General malpresentation causes apply for face.
- Small chance of congenital issue like no brain or thyroid swell, exclude by ultrasound.
- Mostly from head extension in normal fetus.
- Suspect face on belly exam if head bump felt higher on opposite side of fetal spine.
- In thin woman, deep groove may be felt between occiput and back.
- Face confirmed on vaginal exam when nose, eyes, hard gum edges felt.
- Hard to recognize if membranes whole, especially if part high or swelling from labor hours.
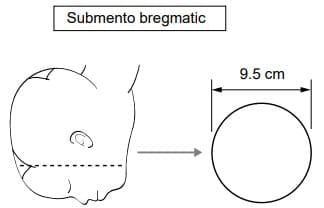
The anteroposterior submento-bregmatic diameter of face presentation
- Labor mechanism like vertex.
- Transverse submento-bregmatic diameter enters pelvis.
- Mostly rotates forward to mento-anterior, chin behind symphysis pubis.
- Presenting side biparietal 9.5 cm and front-to-back submento-bregmatic 9.5 cm good for vaginal.
- Show the Image front-to-back submento-bregmatic diameter of face. Reproduced from the 1st edition of Dewhurst's textbook of Obstetrics and Gynaecology for Postgraduates.
- Descent possible back in pelvis for mento-anterior due to large sacral space.
- Head born with chin under pubic arch, then forehead over perineum.
- If rotates to mento-posterior, though diameters same, frontal bones side large, no descent behind narrow retropubic arch, so C-section advised.
- Even with good mento-lateral or anterior, if no progress, safer C-section in first stage.
- In late second stage with face at outlet in mento-anterior or lateral, outlet forceps by skilled if no spontaneous.
Shoulder presentation
- In women with prior births and single pregnancy, shoulder more common without cause from uterus laxity.
- Linked to preterm, congenital fetal or uterine malformation, fibroids, placenta praevia, too much fluid.
- Rate at term about 1:400.
- Transverse lie with shoulder antenatal fixes to lengthwise with labor start from more uterus muscle tone.
- If membranes break with transverse fetus, likely cord prolapse, shoulder presentation, arm prolapse with cervix opening.
- In early labor with whole membranes, wait for spontaneous or helped fix to lengthwise while preparing C-section.
- If membranes break and still transverse, C-section to avoid fetal or uterus injury.
- If diagnosis late, fetus may be stuck transverse, safe delivery only by C-section with midline vertical cut.
- Possible to deliver through lower transverse cut with quick uterus relax using short drug like 0.25 mg terbutaline in 5 cc saline IV over 5 min.
- If uterus not contract after despite oxytocics, small beta blocker like 1 mg Propranolol IV may need to contract uterus and avoid bleeding after birth.
- Labor and spontaneous vaginal possible in very preterm and dead fetuses.
Cephalopelvic disproportion
- Diagnosis of cephalopelvic disproportion usually after well-done labor trial.
- In first stage, no cervix dilatation despite good contractions, more caput and moulding, CTG signs of head press, fresh meconium may suggest disproportion.
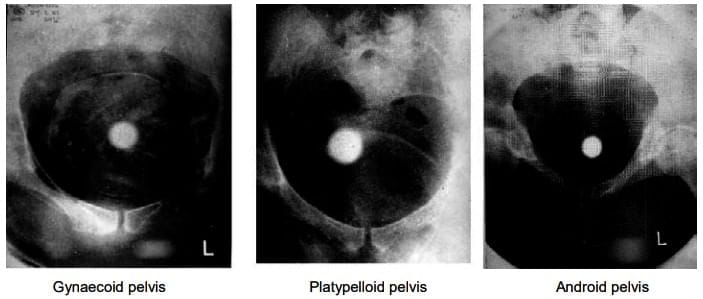
Different pelvic shapes in xxx that influences outcome of labour.
- Traditionally, no progress from issues with passage, passenger, power.
- If cervix not dilate well under 0.3 cm/h with 6-8 h oxytocin boost, rule out power issues, look for passage or passenger problems.
- Clear passenger issues like big head from fluid, large baby, brow should be found before boost.
- Similarly, born small pelvis or deformed from accident known earlier.
- Pelvis shape affects labor outcome, rarely from android or platypelloid pelvis.
- Show the Image different pelvic shapes that influence labor outcome: Gynaecoid pelvis, Platypelloid pelvis, Android pelvis. Reproduced from the 1st edition of Dewhurst's textbook of Obstetrics and Gynaecology for Postgraduates.
- More common relative disproportion from degrees of head deflexion or asynclitism showing larger diameter.
- Enough contractions 6-8 h may help flexion, fix asynclitism, moulding for smaller head diameter.
- Also helps max pelvic give by more symphysis pubis separation.
- These changes may lead to labor progress and delivery.
- In second stage, no head descent with more caput and moulding despite good contractions may show disproportion.
- If no progress with spontaneous contractions assessed weak, try oxytocin boost for 1 h.
- If head low enough for instrument delivery, woman may push.
- No descent means disproportion.
- If from malposition or asynclitism and station below spines, possible delivery by forceps or ventouse.
- No progress from disproportion in first stage and second when station high, delivery by C-section.
Instrumental vaginal deliveries
- Rate of instrumental vaginal deliveries varies 6 to 12%, depends on place and people.
- Common reasons: delay in second stage, poor mother push, fetal distress including cord prolapse in second stage.
- Mother reasons: severe heart, lung, high blood pressure disease or brain issue where push may harm health.
- Long second stage from weak uterus contractions, poor mother efforts, minor disproportion or malposition.
- Rate slightly more with epidural, may from weak uterus activity second to no Ferguson's reflex from no reflex oxytocin release from upper vagina stretch.
- Weak uterus in these women may improve with oxytocin drip to lower instrumental deliveries.
- Certain musts before instrumental vaginal delivery.
- Mother and fetus condition, clinical situation considered carefully.
- Medical person introduce to woman and partner, explain instrumental reason.
- Assessment with chaperone.
- Findings, action plan, procedure explained.
- Verbal or written consent based on rules after explain indication, pros, cons, recorded.
- Distressing time for mother and partner, sensitive explain and counsel needed.
- General check: mother condition, pain relief, hydration.
- Pain relief as pudendal block and local perineum infiltration (20 ml 1% plain lignocaine) enough for low forceps or ventouse.
- For midcavity, epidural; for trial, spinal better.
- Fetal condition based on clinical info and auscultation or CTG normality degree.
- In cord prolapse, bleeding before birth, long deceleration, urgency to deliver, actions quick.
- Belly exam key to check fetus size, fifth of head felt, contractions enough.
- Oxytocin if contractions weak (less than four in ten minutes, each over 40 s) no fetal issue signs.
- Bladder not felt means empty; if not, catheterize.
- If fetus large (depends on mother size but over 4.5 kg estimate), extra care to avoid long pull, prepare for shoulder dystocia.
- Vaginal exam confirm cervix full dilated, membranes gone.
- Note amniotic fluid color and amount.
- Presentation vertex.
- Too much caput or moulding suggest some disproportion.
- Overlapping skull bones not reducible with gentle press is moulding +++ ; ++ overlapping reducible by gentle digital press; + bones meeting no overlap.
- Position like left occipito-anterior or occipito-transverse, station as leading bony skull to ischial spines identified.
- Ideally station below spines with head descent on contraction and push.
- In 3D, female pelvis fits term fetal head.
- So when head 0/5th palpable above brim, leading part below ischial spines.
- In obese mother or occipito-posterior, palpation of fifths above brim hard, deceptive.
- If 1/5th or 0/5th head palpable but vaginal shows head above spines, small head felt may be fetal chin, vertex occipito-posterior.
- No instrumental when head over 1/5th palpable and/or station above spines.
- Station and position decide if proceed with instrumental and instrument type.
- Position by feeling sutures, posterior fontanelle, occiput.
- Inverted Y sutures or parietal over occipital help find posterior fontanelle.
- Posterior fontanelle small, caput and moulding make hard.
- Anterior fontanelle easy as soft diamond at two parietal with two frontal junction.
- If anterior fontanelle easy in pelvis center, means deflexed head.
- In well-flexed, anterior fontanelle to pelvis side wall.
- Useful confirm position by feeling and flicking fetal ear.
- Finger move from occiput direction for ear flick.
- Ear palpation shows largest head diameter biparietal descended below midcavity.
- Sagittal suture should halve pelvis.
- If sagittal far back or front, asynclitism, suggests delay reason, warns instrumental difficulties.
- Head descent and turn with contraction and push give idea of successful instrumental chance.
- Instrumental in dorsal position with legs flexed abducted or left lateral, but easier in lithotomy with buttocks beyond bed edge.
- Check pain relief enough.
- Procedure under clean antiseptic conditions.
- Clean vulva perineum, catheterize bladder if needed.
- Pain relief judged by head station.
- Regional as epidural or spinal for mid cavity, head engaged but station above +2 cm below ischial spines.
- If vertex beyond +2 cm not to pelvic floor, low cavity, regional or pudendal with local perineum enough.
- Outlet when head on perineum, scalp visible no labia separation.
- Here vertex to pelvic floor, direct, right or left occipito-anterior, no or under 45 degree turn.
- Pudendal and local perineum usually enough, some prefer regional.
- Better C-section if head above ischial spines.
- When vertex below spines, instrumental possible, different forceps and vacuum by position and station.
- To compare outcomes, suggest use specific station and position like right occipito-transverse at +2 or left occipito-posterior at +3 at instrumentation time, instead broad mid, low, outlet.
Choice of instruments - forceps/ventouse
- Different forceps and vacuum for instrumental vaginal delivery.
- Choice by operator experience, vertex station, position.
- Assessment of station and position very important.
- For occipito-anterior in mid or low cavity or low direct occipito-posterior (face to pubis), Neville Barnes with or without axis traction handle or Simpson's forceps used.
- Wrigley's ideal for outlet.
- If occipito-lateral or posterior, Kielland's for rotation without trauma to fetus or mother passages.
- Vacuum as silk, silastic or metal cup with suction from cup dorsum, anterior cup for occipito-anterior.
- Posterior metal cup or rigid plastic with suction to cup side for occipito-posterior or lateral
Biparietal-bimalar application offers uniform grip on the two sides. The sagittal suture bisects the shank which is over the flexion point - about 3 cm anterior to the occiput. Not more than a finger can be inserted between the heel of the blade and the head.
- So cup manipulated between head and vagina to flexion point 3 cm front of occiput on sagittal.
Forceps delivery
- Most forceps have pair fenestrated blades with cephalic and pelvic curve between heel and toes at distal end.
- Heel to shank to handle.
- Handles sit together held by one hand, kept by lock on shank.
- Cephalic curve to grasp head, toes over maxilla or malar, blade length grasps sides from malar along head front ear and parietal front occiput.
- This bimalar-biparietal gives even pressure.
- In this, shank over flexion point, correct pull direction.
- Pelvic curve fits pelvis, minimal in rotation forceps like Kielland's.
- Before apply, assemble blades to check pair fit.
- Handle on left hand is left blade, in direct or left occipito-anterior, inserted first negotiating pelvic cephalic curve with curved move between fetal head and operator hand on left vaginal wall.
- Right blade by right hand between left hand protecting vagina and head, negotiating curves.
- If correct, handles horizontal, lock easy.
- Three key points: sagittal suture midline no asynclitism, occiput 3 to 4 cm above shank so traction at flexion point, not over one finger space between head and blade heel so optimal with even pressure from beyond malar to parietal.
- Show the Image biparietal-bimalar application offers uniform grip on two sides. Sagittal suture bisects shank over flexion point about 3 cm anterior to occiput. Not more than finger inserted between blade heel and head.
- Check before traction.
- Traction along pelvic curve, with contractions and mother push.
- Episiotomy usually when head crowning at vulva.
- Traction direction up as head born by extension.
Keilland 's Forceps
- Before Kielland's, key to identify belly fetal back side, vaginal occiput.
- Forceps applied with knobs to baby occiput.
- Anterior or posterior blade first by obstetrician preference.
- Anterior blade by direct, reverse, classical, wandering method.
- In wandering, anterior blade over face then to fetal head side.
- Posterior blade direct.
- Blades locked, asynclitism fixed by sliding shanks till sliding locks same level.
- If no asynclitism, sagittal suture equal from two blades.
- If not lock easy, check application, reapply.
- Abnormal position like occipito-transverse fixed by rotating handles to baby back, then fetal occiput to anterior to emerge under symphysis pubis.
- When correct with shank 2-3 cm below occiput, head flexed with traction.
- No too much twist force.
- Rotational forceps and vacuum for malposition best by experienced or supervised.
Complications of Forceps
- Forceps used less due to more mother vagina perineum tears including 3rd 4th degree vs vacuum.
- Short face scalp scrapes common, clear in days.
- VII nerve paralysis rare, resolves days or weeks.
- Cephalhaematomas and skull fracture rare, depressed fracture may need surgery lift.
Ventouse delivery
- Ventouse or vacuum alternative to forceps for same second stage reasons.
- Conditions for any instrumental checked before apply.
- Cups different sizes, usually 4, 5, 6 cm diameter.
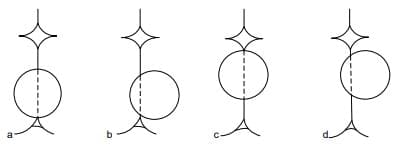
- Cup over flexion point 3-4 cm front occiput on midline by sagittal suture.
- Halfway between parietal eminences, promotes flexion for minimal vertex diameters through pelvis.
- Over flexion point is flexing median application.
- At this, anterior cup margin 3-4 cm behind posterior anterior fontanelle margin along sagittal.
- If close occiput not midline, flexing paramedian.
- If midline closer anterior fontanelle, deflexing median.
- If off midline, deflexing paramedian.
- Deflexing show larger diameters especially paramedian.
- Show the Image possible vacuum cup placement most favorable to unfavorable (a) to (d): (a) flexing median; (b) flexing paramedian; (c) deflexing median; (d) deflexing paramedian.
- Key for accoucheur to know head position, if asynclitic, so cup correct over flexion.
- Special cup for occipito-lateral or posterior.
- Tubing from lateral cup aspect (posterior metal) or groove in cup (posterior rigid plastic Omni cup) allow insert move between vaginal wall and head to flexion point.
- Soft silk, plastic or anterior metal with tubing from cup center for occipito-anterior as flexion within reach when labia parted, cup advanced.
- These not for occipito-posterior or lateral as lateral wall not allow central stem or tubing on dorsum for shift to occiput.
- Once cup firm on scalp, vacuum by hand or mechanical pump to 0.2 bars or 150 mmHg or 0.2 kg/cm2 negative pressure.
- Check position to sagittal and posterior fontanelle, exclude vaginal or cervical tissue.
- Increase vacuum to 0.7-0.8 bars or 500-600 mmHg or 0.8 kg/cm2 before traction with contractions and push.
- No need vacuum in steps 0.2 bar every minutes or release between tractions.
- Traction to flex head, descend along pelvis axis.
- Descent with flexion promotes auto-turn to occipito-anterior from lateral or posterior.
- Ventouse over forceps increased last decade from proof less perineum trauma including third degree tears.
- Soft tissue in cup stays as raised circular bump called chignon, settles 2-3 days.
- Baby injuries: scalp scrapes, eye bleeds, haematoma to one skull bone, baby jaundice, rarely subgaleal bleed causing severe injury or death.
- Also more baby jaundice.
- Follow-up of low outlet instrumental show normal physical neurological outcome.
- Not used in very preterm under < 34 weeks babies and those with possible bleed tendencies for fear subgaleal bleed and injury or death.
Possible placementof the vacuum cupmost favourable to unfavourable
(a) to (d);
(a) Flexing median;
(b) Flexing paramedian;
(c) Deflexing median;
(d) Deflexing paramedian.
- Apply ventouse before full dilatation but after 7-8 cm in multiparous by experienced but caution.
- In heart, lung, neurological disease where mother push may compromise, forceps better than vacuum.
Trial of instrumental delivery
- Sometimes hard to assess if instrumental safe or choose C-section.
- If fetal distress, C-section better as delay may harm baby.
- Trial in theatre under good epidural or spinal, with theatre team, anesthetist, pediatrician present.
- Intent to stop instrumental if hard, go immediate C-section.
- This explained clear to mother and partner, consent before, done by senior.
Caesarean section
- Delivery of baby by abdominal and uterine cut known as Caesarean section (CS) is more used for safe delivery.
- For fetal or mother reasons, elective or emergency.
- Small part from mother request no medical reason or money gain.
- Blood transfer safe, better anesthesia, clean techniques, antibiotics make it safe.
- Rate 10-25% in most developed places, depends on people and facilities.
Indications For CS
- Based on timing at decision, indications in four groups.
- Category 1 or emergency CS: immediate threat to mother or fetus, ideally within 30 min, like abruption, cord prolapse, scar rupture, scalp blood pH under 7.20, long FHR deceleration under 80 beats/min.
- Category 2 or urgent CS: mother or fetal issue but not life threat now, deliver within 60-75 min, FHR problems concern.
- Category 3 or scheduled CS: need early delivery but no issue now, concern pregnancy continue may affect in hours or days.
- Wide indications, like no progress CS in next hour or two, or growth restricted preterm fetus with no end diastolic flow but normal CTG, or preeclampsia with slow worse liver or kidney tests, CS in hours to days.
- Timing varies but plan to deliver before worse.
- Category 4 or elective CS: timed to suit mother and staff, indication for CS but no urgency, like placenta praevia no bleed, malpresentations like brow breech, past hysterotomy or vertical cut CS, past repair vesico-vaginal or recto-vaginal fistulae or stress incontinence, HIV.
- Placenta accreta more with anterior placenta praevia in scarred women, may cause big bleed, rarely hysterectomy, so consent and prepare right.
- Place intra-arterial catheters for embolization of uterine arteries at CS if facilities.
- Elective CS around 39 weeks as newborn breathing issue less after.
- But medical or obstetric condition sets gestation for elective CS, main to do as late as possible without harm to mother or fetal health.
Types of Caesarean Section
- CS described by uterus incision type.
Lower uterine segment incision
- Lower segment CS has horizontal cut on lower segment after folding back visceral peritoneum.
- This commonest CS.
- Abdomen opened by low midline, paramedian, or more Pfannenstiel (suprapubic horizontal) cut, peritoneal cavity opened.
- Bladder folded from lower segment, transverse cut on lower uterine segment careful not injure fetus.
- Presenting part delivered through lower segment.
- Forceps can assist in head presentation.
- Traditionally lower uterine segment muscle closed two layers then visceral peritoneum closure.
- Merits of single vs two layer muscle closure and closure vs no closure of visceral peritoneum now studied by CAESAR randomized trial.
- Lower segment CS common as easier cut lower segment, deliver fetus from cut point, approximate layers from thin muscle vs upper.
- Plus peritoneal layer can close, thought advantage vs infection.
- Blood loss and infection less with lower segment CS vs upper segment CS.
- Uterine cavity cleaned no retained tissue.
- Make sure cervical os open for blood drain.
- Uterine wound closure followed by peritoneal toilet, blood or fluid in abdomen pelvis removed by suction or gauze on sponge holder.
- Chance to check ovaries and tubes.
- Prophylactic antibiotics and low molecular weight heparin vs thromboembolism given intra-op by anesthetists.
- If mother Rhesus negative and baby positive, anti-D given, Kleihauer-Betke test for dose adequacy.
- Mother care like after major abdominal surgery.
Midline Vertical Incision
- Midline vertical cut could be lower or upper segment.
- Commonly starts lower segment as small buttonhole till uterine cavity, extended up.
- Because hard to cut, more blood loss, poor approximate at close, more post-op issues, no trial vaginal next pregnancy from possible higher scar rupture, midline reserved for specific.
- Midline used when lower segment hard from fibroids or anterior placenta praevia with large vessels lower segment.
- Other: preterm breech poor formed lower segment, stuck transverse lie with broken membranes or transverse lie with uterus anomaly.
- Extreme like perimortem CS.
- In special, lower or upper (or span both) vertical or inverted T cut made.
Complications Associated With CS
- Injury and death with procedure not fully avoidable.
- Common issues: bleed, anesthesia issues, infection.
- Prophylactic antibiotics to lower infection.
- Sometimes injury to bowel, bladder, ureters or fetus.
- Thromboembolism rare but fatal, so pre, intra, post-op steps to avoid.
- Intra-op pneumatic boots for legs, prophylactic heparin.
- Post-op heparin, graded elastic stockings, move, chest leg physiotherapy to lower deep venous thrombosis.
- Late issues wound infection, second bleed not uncommon.
- Vesico or uretero-vaginal fistulae from visceral injury very rare.
- Anesthetic issues very rare from experienced anesthetists, most CS under regional.
- Women rarely complain light general anesthesia causing awareness unnoticed as paralyzed.
- Other: vomit on induction, post-op lung collapse after general.
- Aspiration gastric contents causes Mendelson's syndrome, dreaded general anesthesia issue can cause mother death.
- To lower, gastric contents neutralized 20 ml 0.3 Sodium citrate, emptying with Metoclopramide 10 mg IV.
- For elective CS, Ranitidine 150 mg H2 agonist 2 h before.
- In recent meal or opiates, pre-op stomach emptying to lower post-op aspiration risk.
- Caesarean hysterectomy for uncontrollable post-birth bleed, placenta accreta or uterus rupture, cervical cancer as planned treatment.
- Mother death very low, usually from CS reason or anesthetic or bleed issues, estimated under 0.33 per 1000.
Episiotomy and perineal lacerations
- Perineal tears can happen with normal or instrumental vaginal delivery.
- Vulval and front vaginal tears occur with vaginal delivery but back vaginal tear with perineal injury more common, happens more with head delivery, sometimes shoulders.
- Perineal tears classified by perineum involvement.
- First degree tear skin only, second degree perineal muscle.
- Injury to anal sphincter third degree tear, subdivided by involvement degree.
- If under half thickness external anal sphincter 3a, full thickness 3b, internal sphincter involved 3c.
- When tear damages sphincter and anal epithelium fourth degree tear.
Episiotomy
- Episiotomy intentional surgical perineum cut after informed consent to increase soft tissue outlet for birth help.
- Not suggested for every delivery, rate depends on caregiver view and judgment.
- Episiotomy suggested when front tears with bleed or multiple perineal tears appear.
- When fetal distress, done to speed delivery.
- Helps instrumental vaginal deliveries though less need with ventouse and stretchy perineum.
- If delivery delayed thought from rigid perineum, episiotomy may help.
- When vaginal actions needed like some assisted breech deliveries, shoulder dystocia, episiotomy useful.
- Women with past pelvic floor or perineal surgery may benefit from episiotomy.
- In USA, midline episiotomy from fourchette few cm toward anus popular, while mediolateral from fourchette lateral to 45 degree in UK.
- Sharp scissors for single cut 3-6 cm by perineum size.
- Depth involves superficial perineal muscles like second degree tear.
- If episiotomy with normal vaginal delivery, local perineal infiltration enough.
- In instrumental, woman may have epidural or spinal.
- Whatever anesthesia, key check if feel pain before cut, if need more local infiltration.
- Though midline episiotomies minimal bleed, easier repair, less pain post, heals well vs mediolateral, more 3rd 4th degree tears from straight easy extend to anus.
- Noticeable blood loss not uncommon with episiotomy, avoided by doing when head crowns.
- Early cut increases blood loss, immediate repair after delivery helps minimize blood loss.
Perineal Repair
- Adequacy of pain relief rechecked before start repair, made easy with good light, optimal exposure.
- Exposure and hard see vaginal skin edges from bleed above overcome by tampon or vaginal swab with tail out introitus.
- Care to remove tampon or swab after repair done.
- Vagina very vascular, descending branches to vaginal skin may retract, so apex of tear or episiotomy secured by suture above apex to stop bleed.
- Suture threaded down at half to 1 cm intervals taking each vaginal wall turn with continuous locking suture using synthetic like vicryl rapide.
- This helps stop bleed, prevents vaginal shortening.
- Distance between sutures medial side may longer vs lateral vaginal wall for good approximate so at fourchette hymenal membrane and pink vaginal skin to pigmented outer skin margin meet as before tear or episiotomy.
- Perineal muscles approximated by continuous or interrupted sutures.
- Perineal skin approximated by subcuticular suture as less pain, heals well.
- Continuous loose non-locking sutures to approximate perineal muscles and subcuticular has less pain, no need remove sutures.
- Vaginal exam confirm good approximate of cut edges, good stop bleed.
- Rectal exam not always needed but helps exclude accidental suture in rectum.
- Before clean and place pad vs vagina, instrument needle swabs count.
- Detailed notes include estimated blood loss, post repair care include enough instructions for pain relief with right analgesics.
- Though rare, episiotomy and perineal tears may have bleed, pain, haematoma need more medical or surgical within hours of repair.
- Late issues infection, break down repair, pain, scarring, painful sex, rarely fistula.
- Endometriosis of scar rare but consider if woman complains cyclical pain at episiotomy site.
Third and Fourth Degree Tears
- Careful exam reveal damage extent as 3 a, b, c or 4th degree tear.
- Once recognized as 3rd or 4th degree, repair in operating theatre with good light, experienced help, right instruments, under anesthesia to relax sphincter as dissection and muscle mobilization needed.
- Anal epithelial tears repaired with 3/0 vicryl rapid sutures, knots on lumen side.
- 3/0 PDS suture with round bodied needle for muscle repair.
- Post-op care key, managed with laxative, stool softener, antibiotic.
- Symptoms may last, repair not always success with risk incontinence feces and gas.
- Where facilities, follow-up to evaluate symptoms, if need do investigations like endo-anal ultrasound or anal manometry.
- If symptoms last, repair by experienced colorectal surgeon may consider.
FAQs on Chapter Notes: Malpresentation, malposition, cephalopelvic disproportion and obstetric procedures
| 1. What is malpresentation in labor, and what are the types? |  |
| 2. What is cephalopelvic disproportion (CPD), and how does it affect labor? | |
| 3. What considerations are important when choosing between forceps and ventouse for assisted delivery? | |
| 4. What are the indications for performing an episiotomy during labor? | |
| 5. What are the types of perineal lacerations, and how are they classified? | |



