Chapter Notes: Menopause and the postmenopausal woman


Introduction
- We are currently in a time when the population is getting older, with over 30% of women being 50 years old or more.
- It is crucial to take care of health during and after menopause to reduce the economic impact on society now and in the future.
- Recently, there has been negative media coverage about hormone replacement therapy (HRT), which is still considered an effective way to relieve menopausal symptoms.
- This controversy has created confusion for menopausal women, health professionals, and society about how to handle the short and long term effects of menopause.
Key Considerations
- Immediate Symptoms: The immediate symptoms of menopause can be very debilitating and need to be addressed promptly.
- Long-term Sequelae: Long term issues such as osteoporosis, which is a significant concern post-menopause, require attention as well.
- Ageing Society: These health issues will become increasingly important due to the ageing population.
Menopause Demographics
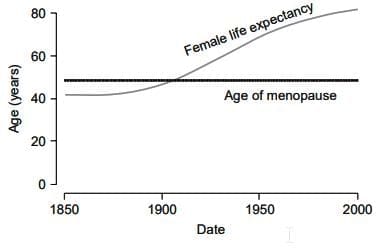
- 200 years ago, only 30% of women lived through menopause. Now, more than 90% will experience it.
- This shift means that the menopause transition and postmenopause are important parts of the 20th and 21st centuries.
- In the UK, life expectancy for women is now 82 years.
- As a result, most women can expect to spend over a third of their lives in a menopausal state.
Challenges for Postmenopausal Women
- Many postmenopausal women struggle with their quality of life.
- Improving menopause health care can help create a society where postmenopausal women maintain optimal health.
Understanding Menopause: A Physiological Perspective
- The term "Menopause" comes from Greek words meaning "Month" and "Cessation," signifying the end of menstrual cycles.
- Diagnosing menopause requires a year without any menstrual period.
- While the average menopause age is 51, body changes can begin years earlier and vary from person to person.
- Hormonal shifts can continue long after the last menstrual period.
The Climacteric Phase
- This transitional phase, called the climacteric (from the Greek word for "ladder"), involves significant changes in the body's neuroendocrine system.
- The climacteric phase can lead to various challenging issues, including:
- Reduced fertility
- Menstrual irregularity
- Vasomotor symptoms (Such as hot flashes)
Intermediate Effects
- The initial effects of these changes are often observed in the skin and urogenital area.
- Over time, these changes can contribute to problems with the skeletal system and cardiovascular health.
Female life expectancy
The Declining Oocyte Pool
- A baby girl is born with more than a million oocytes.
- As she grows older, the number of oocytes declines sharply, with only a few thousand remaining by her forties.
- After menopause, very few oocytes are left, often leading to infertility.
- The depletion of oocytes eventually results in the cessation of menstruation, which is a primary indicator of menopause.
- Ovarian failure occurs in two main stages:
- In the first stage, there is a marked decline in fertility, but menstrual cycles remain unaffected.
- In the second stage, changes in menstrual cycles become noticeable, with a shortened follicular phase and problems in the luteal phase.
Compensated and Decompensated Ovarian Failure
- Compensated ovarian failure begins with increased levels of gonadotropins, which can start in some women around the age of 30.
- During this phase, there is a reduction in the number of gonadotropin receptors in the ovaries of women nearing menopause.
- At the same time, the production of Inhibin by granulosa cells decreases, leading to a lower Inhibin:FSH ratio.
- Decompensated ovarian failure occurs when the oocyte pool declines significantly.
- This decline triggers a dramatic increase in follicle stimulating hormone (FSH), by 10 to 20 times, while luteinizing hormone (LH) increases only threefold due to its shorter half-life.
- As a result of the reduced number of follicles and the ageing of granulosa cells, oestrogen levels decrease, and there is a permanent cessation of progesterone production.
- Research indicates that the decline in Inhibin B is gradual and is not a better predictor than FSH for the final menstrual period (FMP).
- However, the early decrease in follicular phase levels of Inhibin B is easier to detect than the decline in FSH, making it a more reliable initial indicator of reduced ovarian reserve and menstrual irregularities.
Other Hormonal Changes
- Androgens: Both adrenal and ovarian androgen levels start to decrease from around age 20 until perimenopause, stabilizing by the time of the final menstrual period (FMP). Some testosterone is still produced by ovarian theca cells.
- Premature Ovarian Failure: The decline in androgen levels is especially pronounced in cases of premature ovarian failure, whether it occurs naturally or due to medical intervention.
- Oestrogen Therapy: Oestrogen therapy can increase sex hormone binding globulin levels, leading to further decreases in free androgen levels.
- Postmenopausal Oestrogen: The primary postmenopausal oestrogen is oestrone, which is mainly produced in peripheral adipose tissue and the postmenopausal ovary. Minimal oestrogen is produced, mostly through the aromatisation of adrenal androstenedione.
- Somatotrophic Axis: With age, the somatotrophic axis becomes less active, resulting in insulin resistance and an increase in central adiposity. This change leads to a shift in body shape from the female gynaecoid shape to the male android shape, which is an independent risk factor for coronary heart disease.
- Perimenopausal Weight Gain:
- Several factors contribute to perimenopausal weight gain, including:
- Genetic predisposition
- Socio economic influences
- Reduction in caloric need and expenditure
- Decrease in lean body mass
- Reduction in resting basal metabolic rate
- Several factors contribute to perimenopausal weight gain, including:
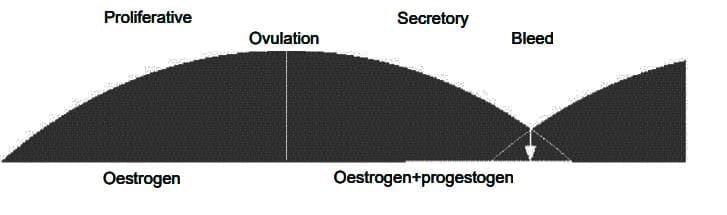
Understanding the Menstrual Cycle
- The menstrual cycle involves complex hormonal changes in the body.
- There is an increasing occurrence of anovulatory cycles, where ovulation does not take place.
- If a person misses three or more menstrual periods within a year, it is likely that they will complete the menopause transition within the next four years.
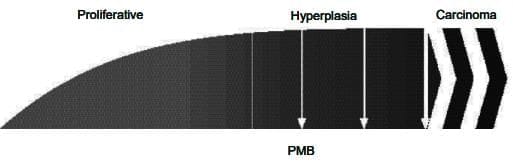
- Without the hormone progesterone, the body may continue to produce oestrogen, leading to:
- Endometrial proliferation, where the uterine lining grows excessively.
- Hyperplasia, an abnormal increase in the number of cells.
- In severe cases, the development of carcinoma, a type of cancer.
- This imbalance can cause menstruation to become:
- Heavy, with increased flow.
- Prolonged, lasting for extended periods.
- Unpredictable, with irregular timing.
- These symptoms, along with intermenstrual bleeding, may indicate underlying health issues and are not solely a result of the menopause transition.
Predicting Ovarian Reserve
- A study of the Hutterite population, who do not use contraception, showed that fertility rates significantly decline after the age of 35.
- This decline is due to several factors, including:
- Reduced oocyte numbers
- Poor oocyte quality
- Lower fertilization and implantation rates
- Decreased coital frequency
- Increased chromosomal anomalies
- The success of oocyte donation in in vitro fertilization (IVF) indicates a healthy and receptive endometrium.
- Ovarian reserve and response to gonadotrophin stimulation can now be predicted by two methods:
- Estimating early follicular phase FSH levels or Inhibin B
- Ultrasonographic measurement of ovarian volume
- An FSH level of >30 is a general guideline for diagnosing menopause, but individual assessments may differ due to fluctuations in ovarian activity, which can resume during the climacteric.
- Current research aims to develop an accurate predictive model for menopause by combining FSH and Inhibin with anti-Mullerian hormone (AMH).
- Recent studies have shown that follicular reserve can be predicted by measuring ovarian volume.
- The original research took place over 10 years ago, producing a nomogram from measurements in over 2000 normally cycling women, estimating the mean ovarian volume to be 3.57 cm³.
- Further work is necessary to confirm the predictive value of this model, but a combined model using both hormonal and sonographic measurements may be feasible.
Premature Ovarian Failure
- Premature ovarian failure refers to the cessation of menstruation before the age of 40 or the onset of menopause before 45.
- The primary cause is often idiopathic or spontaneous.
- However, there are genetic factors that can contribute, including:
- Turner's syndrome
- Fragile X syndrome
- Forkhead gene abnormalities, particularly defects in FOX03A, which lead to early activation of ovarian follicles and depletion of the follicle reserve.
- Another cause involves FSH receptor polymorphisms, where follicles are present but cannot respond due to the lack of the FSH receptor.
Endometrial effects of perimenopause
(a) Normal cycle
(b) Unopposed oestrogen effect
- The incidence of iatrogenic premature ovarian failure is rising as more women survive conditions such as leukemias, lymphomas, and gynaecological cancers due to improvements in surgical techniques, radiotherapy, and chemotherapy.
Consequences of the menopause
Immediate Effects
- Hot Flushes and Sweats: These are the most common symptoms of menopause. About 70% of Caucasian and Afro-Caribbean women experience them. In contrast, only 10-20% of Japanese and Chinese women report these symptoms, possibly due to differences in culture or diet, such as the intake of isoflavones.
- Cause of Hot Flushes: Hot flushes may be caused by the loss of oestrogen, which affects the activity of opioids in the hypothalamus, leading to difficulties in regulating body temperature.
- Role of Neurotransmitters: Neurotransmitters like noradrenaline and serotonin are believed to be involved in this process. Medications such as clonidine and venlafaxine are used as alternatives to hormone replacement therapy (HRT) to help manage these symptoms.
- Impact of Obesity: Women with obesity may experience fewer hot flushes and sweats because they have higher levels of oestrone and lower levels of sex hormone-binding globulin. This allows more active hormone to remain in their bodies.
- Other Immediate Symptoms: These include insomnia, anxiety, irritability, memory loss, tiredness, and poor concentration.
- Mood Changes: Fluctuations in hormone levels during menopause can lead to mood changes and perimenopausal depression. Declining oestrogen levels are thought to reduce neurotransmitters like serotonin, contributing to these symptoms.
- Vulnerability to Depression: Women who have a history of post-natal depression or premenstrual syndrome may be more susceptible to depression during perimenopause.
- Stabilising Hormone Levels: Treatments such as transdermal oestradiol can help stabilise hormone levels and alleviate symptoms.
- Cognitive Function: The effect of menopause on cognitive function is not fully understood. Some studies suggest a decline in cognitive skills, particularly in mathematical and visuo-spatial tasks. These cognitive issues may improve with oestrogen replacement, but more extensive studies are needed to confirm these findings.
- Sexuality and Libido: The menopause transition can lead to a decrease in sexuality and libido. This decline is partly due to reduced vaginal lubrication, which can cause painful intercourse (dyspareunia).
- Decrease in Androgens: There is also a decrease in androgen levels, which affects sexual desire. Women have more androgen receptors in their forebrain than men, and these receptors play a role in sexual aspects.
- Impact of Early Menopause: The drop in androgens is particularly significant for women who experience early menopause or premature ovarian failure, whether naturally or due to medical reasons.
Intermediate
- After menopause, a deficiency in oestrogen leads to a rapid loss of collagen, resulting in generalised atrophy.
- In the genital tract, this atrophy causes:
- Dyspareunia, which is pain during intercourse.
- Vaginal bleeding due to the fragility of the atrophic skin.
- Loss of rugations (the folds or ridges in the vaginal lining) and occasional stenosis (narrowing).
- In the lower urinary tract, the atrophy of the urethral epithelium leads to decreased sensitivity and various urinary symptoms, including:
- Dysuria, which is painful urination.
- Urgency and frequency of urination, collectively referred to as the urethral syndrome.
- Older women may also experience broader changes such as:
- Increased bruising.
- Skin that is thin, translucent, and more susceptible to trauma and infection.
- The similar loss of collagen in ligaments and joints may contribute to common aches and pains experienced by postmenopausal women.
Long term Effects of Menopause
- Osteoporosis is a health issue where bones become weak and fragile, leading to a higher risk of fractures and breaks.
- Cardiovascular disease refers to problems with the heart and blood vessels, which can increase during and after menopause.
- Dementia is a condition that affects memory and thinking, and it has been associated with menopause as well.
- These three health problems are often seen as long-term effects of the menopause, which is a natural part of aging in women.
- It is essential for women to be aware of these potential health risks during and after the menopause to take steps for prevention and management.
Osteoporosis
- Osteoporosis, or osteopenia, is a condition that makes bones weak and more likely to break.
- These fractures can lead to serious health issues in older adults, often requiring long hospital stays and making it difficult for them to regain mobility.
- The financial burden is significant: In the UK, over 150,000 fractures occur each year, costing around £1.75 billion annually, while in the USA, the cost is about $5 billion.
- With an ageing population and an increase in osteoporosis cases, these costs are expected to rise.
- Osteoporosis primarily affects women, who generally reach a lower peak bone mass than men and lose bone density more quickly after menopause.
- After menopause, the decline in oestrogen levels leads to a greater loss of bone than the formation of new bone.
- By the age of 70, 50% of women will have experienced at least one osteoporotic fracture, compared to 25% of men by age 90.
Bone mass and turnover
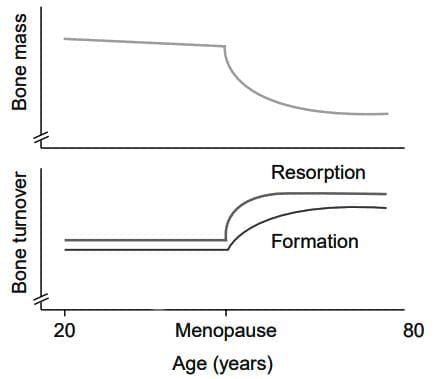
- Although the precise mechanisms of bone remodelling are not fully understood, ovarian hormones like oestrogen are vital for maintaining bone health.
- Factors that can increase the risk of osteoporosis include genetics, race, and lifestyle choices such as smoking and having a low body weight.
- Certain genetic variations may also make individuals more prone to developing osteoporosis. Vitamin D and oestrogen receptor genes, the collagen 1A1 gene and genes for various cytokines including interleukin 6 and tumour growth factor-β.
Cardiovascular Disease
- Before menopause, women are generally at a lower risk for cardiovascular disease, but this risk increases significantly after menopause, becoming similar to that of men by age 70.
- Surveys indicate that menopausal women underestimate their risk of heart disease, believing it to be around 4%, when in reality it is closer to 50%.
- Oestrogen is thought to protect women's heart health by increasing levels of good cholesterol (HDL) and decreasing levels of bad cholesterol (LDL).
- Oestrogen also helps blood vessels dilate, improving blood flow to the heart and protecting the walls of blood vessels.
- Research shows that menopausal women often have higher cholesterol levels and lower HDL levels.
- A study of 438 Australian women identified significant risk factors for coronary events, including high body mass index (BMI) and lower oestradiol levels.
- Recent studies suggest that oestrogen levels can independently predict the build-up of plaque in blood vessels.
- Even premenopausal women with reduced ovarian reserve may be at higher risk for cardiovascular disease.
Central Nervous System (CNS)
- Oestrogen appears to have a positive effect on blood vessels in the brain and supports the growth and communication of nerves.
- Research suggests that oestrogen may enhance blood flow to the brain and improve cognitive functions.
- In the long term, this could help prevent brain disorders such as vascular dementia and Alzheimer's disease, as adequate blood flow is a crucial factor.
- Oestrogen might also be involved in the processing of proteins related to Alzheimer's disease.
- However, some studies, including the Women's Health Initiative Memory Study, indicate that hormone replacement therapy (HRT) may not be beneficial for older women and could increase certain risks.
Evaluating Patients for Menopause
- Diagnosing menopause usually relies on a typical history of vasomotor symptoms, such as hot flushes and night sweats, along with prolonged periods of amenorrhea.
- Testing plasma hormone levels in patients with clear symptoms is often unnecessary, expensive, and time-consuming, offering little clinical benefit.
- However, it can be more challenging to diagnose in younger patients or those who have undergone a hysterectomy. In such cases, measuring FSH levels may be helpful, with levels of 15 IU/L or higher indicating the climacteric phase.
- For menstruating patients, persistent hot flushes and night sweats suggest the climacteric, but diagnosing those with psychological symptoms can be more complicated, even with a thorough psychiatric history.
- In these instances, a trial of oestrogen therapy may be warranted to assess the response before ruling out a hormonal cause.
Investigations after Diagnosis
- After confirming the diagnosis, investigations should be limited to the standard annual screenings for middle-aged women.
- This includes checking weight, blood pressure, and routine cervical cytology.
- A fasting lipid profile may be beneficial for women with risk factors, especially when considering starting HRT.
- The reanalysis of data from the Women's Health Initiative (WHI) study indicated no increased risk of cardiovascular disease in women with abnormal baseline lipids.
- If abnormal lipids are detected, they should be managed with diet and statins before initiating HRT.
- Routine breast palpation and pelvic examinations are not necessary unless clinically indicated.
- Mammography should be performed every 3 years as part of the national screening programme unless more frequent checks are required.
- If a woman chooses to continue HRT beyond the age when regular breast screening ceases, mammographic screening should also persist.
- For women over 45, screening should ideally be arranged before starting oestrogen therapy to identify any sub-clinical issues. An endometrial biopsy is not necessary before HRT unless there are indications of postmenopausal bleeding or irregular perimenopausal bleeding.
- If bleeding occurs after initiating treatment and an underlying malignancy is present, it will be irregular and demand immediate further investigation.
Assessing Osteoporosis Risk
- The most reliable method for assessing osteoporosis risk is dual energy X-ray absorptiometry (DEXA) of the lumbar spine and hip.
- While peripheral X-ray screening (e.g., Proximal Phalanx and Calcaneal) and ultrasound screening are improving, they are not as dependable as DEXA.
- Markers of bone formation and breakdown can indicate rapid changes, but their application is primarily for research purposes.
- There is increasing interest in a national osteoporosis screening programme that measures bone density, as predicting osteoporosis based on clinical risk factors and short term symptoms is not very accurate.
- However, this concept is premature since no studies have demonstrated that bone densitometry is suitable for widespread screening.
- The Royal College of Physicians (RCP) has issued guidelines on which high risk patients should be prioritised for DEXA screening.
- The RCP advises that DEXA scans be conducted no more than every 2 years, as changes in bone mineral density are often smaller than the equipment's margin of error.
Therapeutic options
HRT
Oestrogen, Dosage
- Patients should begin with the lowest effective dose of oestradiol and increase it only if necessary for symptom relief.
- There is no direct evidence linking higher doses of exogenous oestrogen to increased breast cancer or heart disease risk, but higher doses are associated with increased venous thromboembolic risk.
- Lower doses of oestrogen are less likely to cause breast tenderness and bleeding issues, which can facilitate therapy continuation.
- The minimum dosages of currently available systemic oestrogenare as follows:
- 0.3-0.625 mg oral conjugated equine oestradiol
- 1 mg of oral micronized oestradiol or oestradiol valerate
- 25-50 mcg transdermal oestradiol
- 25-50 mg of implanted oestradiol
- 150 mcg transnasal oestradiol
- 50 mcg oestradiol silicone ring
- Research indicates that the benefits of a 2 mg dose of oestradiol for symptoms and bone protection can be achieved with a 1 mg dose.
- Similarly, the benefits of a 50 mg oestradiol implant can be maintained with a 25 mg implant.
- Ongoing research is focused on a 0.5 mg oestradiol preparation that appears effective for symptom relief.
- Women with premature ovarian failure may require higher doses of oestradiol to mimic normal hormone levels.
Route of administration
- To replicate a natural state with a 2:1 oestradiol oestrone ratio, alternative routes of administration should be considered over oral administration.
- Oral oestradiol is partially converted to oestrone in the liver, which does not fully restore the desired ratio.
- Transdermal systems can be changed weekly, delivering either oestradiol alone or in combination with progestogen.
- Combined patches are available in sequential or continuous regimens and avoid the skin issues associated with older patches.
- Oestradiol can be administered transnasally in a 'pulsed' manner to maintain benefits while minimising side effects.
- It is also available as a low-volume daily gel or a silicone vaginal ring that delivers oestradiol for three months.
- The nasal, gel, and ring preparations contain only oestradiol and should be combined with progestogen for women with a uterus.
Local (vaginal) oestrogen
- New vaginal hormone replacement therapy (HRT) regimens have addressed the concern of endometrial stimulation.
- Oestriol creams do not cause endometrial hyperplasia, and vaginal tablets and silicone rings also effectively relieve local symptoms.
- These preparations can be used without progestogen opposition but are licensed for only three months in the UK and one year in Europe.
- Local vaginal oestrogen options include:
- 0.01% Oestriol cream and pessaries
- 0.1% Oestriol cream
- 25 mcg/24 h Oestradiol vaginal tablets
- 7.5 mcg/24 h Oestradiol releasing silicone ring
- Premarin cream - this can cause endometrial hyperplasia and should not be used without progestogen opposition for more than three months.
Progestogen / Progesterone
Regimens:
- Oestrogen was initially used alone in women who had not undergone a hysterectomy, which led to endometrial hyperplasia in up to 30% of cases.
- Progestogen has been added to oestradiol therapy for the last 30 years to prevent hyperplasia and carcinoma.
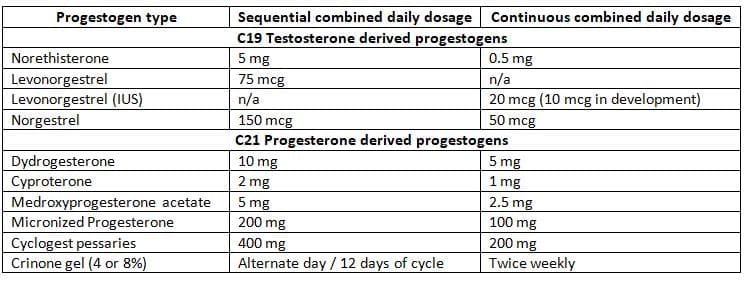
- It is generally recommended that women starting HRT begin with a sequential regimen of continuous oestradiol and progestogen for 12 to 14 days each month.
- Typical dosages of commonly used progestogens are Shown the Table.
Bleeding problems:
- If bleeding is heavy or irregular, the progestogen dose can be increased or the duration extended to 21 days.
- Persistent bleeding issues beyond six months require investigation through ultrasound and endometrial biopsy.
- After one year of therapy, women may switch to a continuous combined regimen for a bleed-free HRT approach that minimises the risk of endometrial hyperplasia.
- Alternatively, women can be switched to theTissue-selective agent tibolonewith both these regimens, there may be some erratic bleeding to start with, but 90% of those who continue with these regimens will eventually be completely bleed free.
- If starting HRT de novo, a bleed-free regimen can be implemented from the outset, provided the last menstrual period was over a year ago.
Minimum doses of progestogen given orally in HRT as endometrial protection
 IUS, Intrauterine system
IUS, Intrauterine system
Progestogenic side effects:
- It is vital that we maximise compliance for patients to receive the full benefits from hormone replacement therapy (HRT).
- Progestogen intolerance is a major factor affecting compliance. Progestogens have various effects beyond their intended use of changing the endometrium.
- Symptoms of fluid retention occur due to the sodium retaining effect of the renin-aldosterone system, which is triggered by stimulation of the mineralocorticoid receptor.
- Androgenic side effects like acne and hirsutism are issues with testosterone-derived progestogens due to stimulation of the androgen receptors.
- Mood swings and PMS-like symptoms arise from stimulation of the central nervous system progesterone receptors.
Minimizing progestogen intolerance:
- The dose can be halved, and the duration of progestogen can be reduced to 7-10 days. However, this may lead to bleeding problems and hyperplasia in a few cases ( 5-10% ), so there should be a low threshold for performing ultrasound scans and endometrial sampling in these women.
- Natural progesterone has fewer side effects due to receptor specificity but is only available in vaginal form in the UK (200-400 mg pessaries or 4-8% progesterone gel), while micronized oral progesterone is available in France.
- The levonorgestrel intrauterine system, recently granted a 4-year licence in the UK for progestogenic opposition, also reduces systemic progestogenic side effects by releasing the progestogen directly into the endometrium with low systemic levels.
- However, even the low levels from the 20 mcg levonorgestrel IUS can still produce side effects in severely progestogen intolerant women.
- A smaller, lower dose, 10 mcg system is in phase III clinical trial stage of development and should be ideal for these women.
- A new progestogen, drospirenone, a spironolactone analogue, has recently been combined with low-dose estrogen in a continuous formulation.
- It is not only progesterone receptor specific but also has anti-androgenic and anti mineralocorticoid properties, which may help with hirsutism and fluid retention, and it may also have anti-hypertensive benefits.
Progestogenic risks:
- The Women's Health Initiative (WHI) and Million Women Study (MWS) clearly showed an excess risk of breast cancer using estrogen and progestogen HRT compared to estrogen alone. It has been suggested that even non hysterectomised women should use estrogen-only preparations.
- According to MWS data, after 10 years of estrogen and progestogen HRT, there would be an extra 19 per 1000 cases of breast cancer and no cases of endometrial cancer; after 10 years of estrogen alone in non-hysterectomised women, there would be an extra 5 cases per 1000 of breast cancer and 10 cases per 1000 of endometrial cancer (Total 15:1000).
- From this perspective, it seems reasonable for all women (even with a uterus) to receive estrogen alone. However, this does not account for the extra cases of endometrial hyperplasia and bleeding problems, which could lead to excessive investigations like endometrial sampling, hysteroscopies, and even hysterectomies, all of which have their own risks.
- Current advice remains that progestogenic opposition should still be used.
- However, finding better ways to administer progestogens to protect the endometrium and minimise side effects is essential.
Testosterone
Preparations/Regimens:
- Unfortunately, only 100 mg/6 months implanted testosterone pellets are licensed for women; 25 mg pellets exist but must be ordered on a named patient basis.
- The recognition of an unfilled market for female androgen replacement has led to the development of a 300 mcg per day testosterone transdermal system to treat 'hypoactive sexual desire disorder'.
- While the licence for this product is awaited, it is necessary to continue improvising if one wishes to use preparations other than implants.
- One option is to use testosterone gel, which comes in 50 mg, 5 ml sachets at a dose of 0.5-1.0 ml per day.
- If the free androgen index remains within the normal range, there are rarely any side effects like hirsutism.
- Levels should be checked at the start and again at 4-6 weeks.
- Research has suggested, at worst, a neutral effect on the cardiovascular system. for example, findings regarding arterial compliance and lipid effects have been neutral.
- Alternatives include reduced doses of testosterone injections and oral preparations, though many avoid the latter due to concerns about the liver.
The Hrt Controversy:
- Over the past few years, health experts and their patients have received a lot of information about the possible advantages and disadvantages of hormone replacement therapy (HRT).
- This information comes from many different sources, and some are more trustworthy than others.
- The media often exaggerates the dangers of HRT through sensational headlines, which can create confusion.
- As a result, health professionals find themselves in a tough spot when it comes to giving advice to their patients.
- Patients are often left feeling uncertain about where to find reliable guidance.
Breast:
- Recent data from the WHI combined HRT study have confirmed earlier observational data from the Imperial Cancer Research Fund (now 'Cancer Research UK') regarding the risks of breast cancer with HRT.
- The WHI study was stopped early after an average of 5.2 years instead of 8.5 years because it was believed that the risks outweighed the benefits, with an excess of breast cancer and coronary heart disease in the treatment group (continuous combined conjugated equine oestrogens 0.625 mg and medroxyprogesterone acetate 2.5 mg).
- The WHI data suggested an extra risk of breast cancer with combined hormone therapy of 4 cases per 1000 women after 5 years.
- This year, further analysis found a hazards ratio for breast cancer of 1.24 (p > 0.001) after an average of 5.6 years on HRT.
MWS Survey Results
- The MWS, a large survey by Cancer Research UK of women in the NHS breast screening programme, reported an increased risk of breast cancer diagnosis with all HRT regimens (Relative Risk [RR] 1.66, 95% CI 1.58-1.75).
- There was a statistically higher risk with oestrogen/progestogen HRT (RR 2.00 [1.91-2.09]) compared to oestrogen alone (RR 1.30 [1.22-1.38]) or tibolone (RR 1.45 [1.25-1.67]).
- This was alarmingly reported by the press as a doubling of risk, without mentioning the absolute numbers.
- For oestrogen alone, it represented an additional 1.5 per 1000 cases after 5 years, and for oestrogen/progestogen, an additional 6 per 1000 cases after 5 years.
- In women aged 50-64, whose baseline risk is 32:1000, this resulted in an increased incidence of 33.5 cases per 1000 and 38 cases per 1000, respectively.
Comparison of MWS and WHI
- The higher risk estimates from the MWS compared to WHI were likely due to the observational nature of the MWS, which underestimated the duration of HRT usage, as it did not account for years of HRT exposure from baseline to breast cancer reporting on the UK cancer registry.
- Additionally, considering the natural biology of breast cancer, it is unlikely that cancers diagnosed after 1 year had developed newly; more likely, these cancers were missed by mammography at baseline, and HRT acted as a promoter, not an initiator.
- Although the MWS reported an increase in mortality, this was borderline significant (RR 1.22 [CI 1.00-1.48]) (p = 0.05); the lack of tumour details made it hard to draw definitive conclusions.
- Some authors have expressed concerns about the limitations of both MWS and WHI data.
- On a positive note, a second WHI study in women with hysterectomies using unopposed oestrogen reported a 23% lower rate of invasive breast cancer in the conjugated oestrogen group compared to placebo, narrowly missing statistical significance (p = 0.06).
- This unexpected result suggests that the addition of progestogen to oestrogen increases breast cancer risk, not oestrogen alone.
Cardiovascular Risks:
- Initial cardiovascular data from observational studies suggested up to a 50% reduction in the risk of coronary heart disease in HRT users and a neutral effect on stroke.
- However, the Heart Estrogen Replacement Study (HERS) did not confirm these findings in women starting HRT for secondary prevention of coronary heart disease, and the WHI study showed no benefit in primary prevention.
- In fact, the WHI suggested that after an average of 5 years of use, there were more heart disease cases in the active treatment group compared to placebo. The study also noted an excess of stroke cases.
- The cardiovascular risks in WHI were small, equating to an extra 7-8 cases per 10,000 women per year, largely due to an increase in cases during the first couple of years, likely because of an initial pro-thrombotic effect of the preparation used.
- The increase in stroke risk was clearly age-related (age 50-59, 4 cases; 60-69, 9 cases; and 70-79 years, 13 cases per 10,000 women per year).
Heart Disease and HRT
- Recent findings from the WHI study's conjugated oestrogen-only group suggest no significant impact on coronary heart disease (CHD) compared to placebo.
- This raises concerns about the role of progestogen in HRT.
- Given evidence from studies like HERS and WHI, guidelines from the American Heart Association and MHRA recommend against using HRT for CHD prevention.
- Future studies should explore new HRT preparations in younger women.
- A pilot study indicated that a specific HRT regimen post-myocardial infarction may lower re-infarction risk, paving the way for larger studies.
- A recent meta-analysis found that women starting HRT before 60 had significantly lower mortality rates, suggesting potential benefits of early HRT intervention.
Dementia:
- Observational and case-control studies have suggested that estrogen may help in preventing Alzheimer's disease.
- However, this idea is not supported by recent findings from the WHI Memory Study (WHIMS), which indicated that there is a two-fold increase in the risk of all types of dementia.
- The participants in the WHIMS study were older women, with an average age of 67 years, suggesting that the opportunity for preventing Alzheimer's might be in a younger age group.
- Increasing evidence points out that a key factor in all forms of dementia is infarction caused by cerebral micro-emboli, which is more likely to occur if hormone replacement therapy (HRT) is started in older women.
- Older women may face a higher risk of pro-thrombotic events during the first few years of HRT, making them more vulnerable to these issues.
- In contrast, starting HRT in a younger age group could provide beneficial effects on blood flow and lipid levels, potentially leading to long-term advantages.
Endometrial Cancer:
- Some research indicates that long-term use of sequential combined HRT might slightly raise endometrial cancer risk.
- In contrast, continuous combined HRT may offer a small protective benefit, as suggested by trends in the WHI and other studies.
- The MWS Investigators conducted an analysis of endometrial cancer risks associated with HRT.
- They found that non-HRT users had a baseline risk of 3 cases per 1000 women after 5 years.
- Sequential combined HRT was observed to have a neutral effect on endometrial cancer risk.
- Continuous combined HRT demonstrated a protective effect, with a reduced risk of 2 cases per 1000 women after 5 years.
- However, women using oestrogen alone had an increased risk, with 5 cases per 1000 after 5 years.
- Interestingly, users of the tissue-selective agent tibolone showed a higher incidence of endometrial cancers (6 cases per 1000 after 5 years), possibly due to higher-risk women being prescribed tibolone.
- A large prospective trial comparing tibolone to placebo showed no evidence of endometrial hyperplasia or carcinoma, leading to the study's continuation without changes.
Venous Thromboembolism:
- Research, including studies like HERS and WHI, indicates a two to threefold increased risk of venous thromboembolism (VTE) with oral HRT, particularly in the initial year of use.
- However, recent findings suggest that transdermal HRT may not elevate VTE risk, which is biologically plausible given its avoidance of hepatic first-pass metabolism.
Osteoporosis:
- For many years, data on bone markers and bone density indicated that HRT had a positive impact on bone health.
- The WHI study provided strong evidence supporting HRT's role in preventing hip and spine fractures, with a reduction of 5 cases per 10,000 women per year.
Colorectal Cancer
- The WHI study corroborated earlier observational research suggesting that combined HRT lowers the incidence of colorectal cancer, with a reduction of 6 cases per 10,000 women per year.
- However, this protective effect was not observed with oestrogen alone.
- The exact mechanism by which HRT reduces colorectal cancer risk remains unclear.
Contraindications to HRT:
- Coronary heart disease, stroke and venous thromboembolism were considered in the previous section.
- Natural oestrogens do not elevate blood pressure in women, whether they are normotensive or hypertensive.
- In fact, when natural oestrogens are combined with oral progesterone, they may even lead to a decrease in blood pressure.
- Therefore, there is no valid reason to withhold Hormone Replacement Therapy (HRT) from women with hypertension.
- Fibroids are influenced by oestrogens and typically shrink after menopause.
- However, Hormone Replacement Therapy (HRT) can keep these non-cancerous growths active, potentially causing them to increase in size.
- This may lead to heavier menstrual bleeding, but it's usually not a major concern since treatment can be easily stopped.
- For patients who have strong reasons to continue HRT, options like fibroid resection, embolisation, myomectomy, or hysterectomy are available.
- Women who have had endometriosis and reach menopause often find relief from their symptoms.
- Some may consider HRT, as there is a 4% chance of symptoms returning with its use.
- If HRT is stopped, any recurring symptoms can be alleviated.
- The treatment of patients with a history of endometrial cancer is a subject of debate.
- Some reports suggest that using oestrogen does not have negative effects for stage I to III patients.
- Squamous cervical cancer does not respond to oestrogen.
- There is no negative data regarding ovarian cancer survivors, although long-term oestrogen use without opposition may slightly increase the risk of ovarian cancer in healthy women.
- No data exists for adenocarcinoma of the cervix, vagina, or vulva.
- Breast cancer is the primary reason to avoid oestrogen treatment.
- However, women at high risk with a family history of breast cancer or benign breast conditions may not need to be denied treatment.
- The exact risk of breast cancer recurrence with HRT is unclear.
- A study on breast cancer survivors using HRT was stopped due to apparent increased risks, which also led to the premature termination of two other studies that found no excess risk.
- A large study on tibolone in breast cancer survivors is ongoing and has been allowed to continue by the data monitoring board.
Duration of HRT:
- According to the Women's Health Initiative (WHI), the risk of breast cancer appears to increase after 4 years of HRT.
- The Million Women Study (MWS) indicates a significant risk increase after just 1 year.
- However, cancers that manifest within a year may have been present beforehand, with HRT acting as a promoter rather than a cause.
- An editorial in The Lancet suggested limiting therapy duration to 3-6 months, but it is acknowledged that symptoms often return after stopping HRT, even after long term use.
- Since HRT aims to enhance quality of life, imposing strict time limits may not be justified.
- Therefore, therapy duration should be carefully evaluated based on individual benefits and risks.
- If therapy is to be discontinued, the dose should be gradually reduced over at least 6 months to minimise severe symptom resurgence.
Guidance for Health Professionals:
- The Medicines and Healthcare Products Regulatory Agency (MHRA) advises against using HRT for preventing heart disease.
- It is recommended for short term symptom relief at the lowest effective dose, and other options should be considered for long term osteoporosis prevention.
- Annual reviews of HRT use should assess the pros and cons for each individual.
- However, the British Menopause Society believes that recent studies should not alter prescribing practices, as HRT in the UK is primarily for symptom relief rather than prevention.
Alternatives to HRT
For Symptoms
- There is not much scientific evidence showing that complementary and alternative therapies are effective in managing menopausal symptoms or providing the same benefits as conventional treatments.
- Many women choose these therapies because they believe they are safer and more natural, especially in light of recent controversies surrounding HRT.
- The wide range of treatment options available can be overwhelming for women.
- Unlike conventional medicines, there is limited knowledge about the active ingredients, safety, and potential side effects of these alternative therapies.
- These therapies may have negative interactions with medications such as warfarin, antidepressants, and anti-epileptic drugs, posing serious risks.
- Some herbal products might contain compounds that mimic estrogen, which is particularly concerning for women with hormone-sensitive conditions like breast cancer.
- There are also concerns about contaminants in herbal products, including harmful substances like mercury, arsenic, lead, and pesticides.
- New regulations will require herbal preparations to be registered with the MHRA (Medicines and Healthcare products Regulatory Agency).
- This registration aims to regulate products that may be ineffective or harmful, ensuring they meet certain standards.
- It is important that alternatives to licensed treatments are held to similar standards of safety and efficacy.
Reasons for Considering Alternatives to Hormone Replacement Therapy (HRT)
- There are various reasons why some individuals may seek options other than HRT.
- The main reason is the preference to avoid hormone therapy due to concerns about potential side effects and risks associated with it.
- Clinicians might also have reservations based on the individual's or their family's medical history,
- Including factors such as:
- Cardiovascular disease
- Venous thromboembolism
- Breast cancer
- In certain situations, an alternative treatment might be considered a more suitable option than traditional HRT.
- While there are numerous alternatives available (over 200!), this discussion focuses on those backed by some trial evidence.
- Recent research indicates the increasing use of complementary therapies:
- 68% of women in a menopause clinic in London have experimented with an alternative treatment.
- 62% of these women reported satisfaction with the results.
Lifestyle Measures
- Some research indicates that women who are more physically active might experience fewer symptoms during menopause.
- However, not all forms of exercise are beneficial; infrequent high-impact activities can actually worsen these symptoms.
- The most effective type of exercise for alleviating menopause symptoms is regular, sustained aerobic activity.
- Additionally, reducing or avoiding alcohol and caffeine intake can help lessen the severity and frequency of vasomotor symptoms, such as hot flashes.
Non-pharmacological alternatives
Bioadhesive Gels for Vaginal Symptoms: e.g., Replens
- Bioadhesive gels like Replens are specifically formulated to address vaginal symptoms during menopause.
- These gels function as moisturisers, replicating natural vaginal secretions to alleviate dryness and discomfort.
- It is important to note that bioadhesive gels serve a different purpose than lubricant gels, such as KY jelly, which are used for immediate lubrication.
- Replens works by rehydrating vaginal tissues, providing a long-lasting solution for dryness and discomfort.
- This product offers an alternative to systemic or vaginal hormone replacement therapy (HRT) for women seeking relief from vaginal symptoms.
Pharmacological alternatives
Progestogens- Progestogens are often used as an alternative to combined hormone replacement therapy (HRT) for women experiencing severe hot flushes who cannot take oestrogen.
- However, recent studies, such as the Women's Health Initiative Memory Study (WHI/MWS), have raised safety concerns about progestogens. These studies suggest that the increased risk of breast cancer associated with HRT may be linked to the combination of oestrogen and progestogen, rather than oestrogen alone.
- Therefore, caution is necessary when prescribing progestogens to women who are at a higher risk of breast cancer.
- Additionally, potential risks to breast health should be considered for individuals at risk of blood clots.
Alpha 2 Agonists
- Clonidine, a central alpha-2 agonist, has been commonly used as an alternative treatment for hot flushes.
- However, it is important to note that clonidine is one of the options with the least evidence supporting its effectiveness, showing only minimal benefits in clinical trials.
Beta Blockers
- Beta blockers have been considered as a potential treatment option for hot flushes.
- Nevertheless, small studies conducted on the use of beta blockers for this purpose have not yielded promising results.
Selective Serotonin Reuptake Inhibitors (SSRIs) / Selective Noradrenaline Reuptake Inhibitors (SNRIs)
- There is substantial evidence supporting the effectiveness of SSRIs and SNRIs in treating hot flushes.
- While SSRIs such as fluoxetine and paroxetine show some positive data, the strongest evidence is for the SNRI venlafaxine, particularly at a dose of 37.5 mg twice daily.
- It appears that these medications primarily stimulate noradrenergic pathways rather than serotonergic ones, which may explain the better results observed with SNRIs.
- Studies indicate that SSRIs and SNRIs can reduce the frequency and severity of hot flushes by 50-60%, compared to an 80-90% reduction with traditional hormone therapy.
- One significant issue with these treatments, especially SNRIs, is the high incidence of nausea, which often leads to patients discontinuing the treatment before achieving maximum relief.
- Ongoing clinical trials are further investigating this area to improve treatment outcomes.
Gabapentin
- Recent research on Gabapentin, an antiepileptic drug, has demonstrated its effectiveness in reducing hot flushes compared to a placebo.
- At a dosage of 900 mg per day, Gabapentin has been found to decrease the frequency of hot flushes by 45% and their severity by 54%.
- Further studies are currently underway to confirm the safety and efficacy of Gabapentin as a treatment for hot flushes.
Complementary Therapies
- Among the largest groups using complementary therapies, middle-aged women make up a significant portion, with up to 33% of this population having tried these treatments at some point (as reported by the European Menopause Survey 2005).
- The total annual cost of complementary therapies is estimated to be around 17 billion US dollars.
- Most of these costs are paid by the users themselves since many of these treatments are unlicensed.
- Many women choose these therapies because they are seen as a safer alternative to traditional hormone treatments.
- However, there are concerns about the safety of some of these therapies.
- The current rules governing complementary and alternative medicine are insufficient and disorganized, with only osteopaths and chiropractors being recognized as regulated professions.
Phytoestrogens
- Phytoestrogens are plant-based compounds that mimic the effects of estrogens in the body. Since the discovery of estrogen-like activity in certain plants, over 300 plant species have been identified for their phytoestrogenic properties.
- Phytoestrogens are primarily found in foods such as soybeans, chickpeas, red clover, and certain oilseeds like flaxseed. The two main groups of phytoestrogens are isoflavones and lignans.
- Isoflavones, including genistein and daidzein, are abundant in soy products and legumes. Lignans, such as enterolactone and enterodiol, are found in flaxseed, cereal bran, whole grains, vegetables, legumes, and fruits.
- Isoflavones are primarily found in soybeans, chickpeas, red clover, and potentially other legumes such as beans and peas.
- Lignans are abundant in flaxseed and are also present in cereal bran, whole grains, vegetables, legumes, and fruits.
- There is significant interest in the role of phytoestrogens in health.
- Populations with high dietary intake of isoflavones, such as the Japanese, seem to experience lower rates of menopausal vasomotor symptoms and certain cancers.
- However, the evidence from randomized placebo-controlled trials in Western populations regarding the benefits of soy and red clover derivatives is mixed.
- There are ongoing studies to further investigate the effects of these products on aspects like lipoproteins, endothelial function, and blood pressure.
Soy
- Twelve randomized controlled trials have been conducted to compare different soy products with a placebo.
- Out of the nine studies where the treatment lasted more than 6 weeks, only four showed a significant improvement in symptoms compared to the placebo.
- One of the most significant trials involved 102 women who were treated for 12 weeks, resulting in a 45% reduction in hot flushes, whereas the placebo group only experienced a 30% reduction.
- Research indicates that mammographic density, which is a marker for breast cancer risk, does not seem to be influenced by soy products even after 2 years of use.
- However, there are some concerns regarding long-term soy treatment, particularly related to a low risk of endometrial hyperplasia.
Red clover
- Red clover contains high levels of isoflavones such as biochanin A and formononetin.
- Soy primarily has different isoflavones, including genistein, daidzein, and glycitein.
- The isoflavones from soy and red clover interact differently with steroid receptors, which might lead to varied effects on symptoms, but this needs more research.
- Five studies that used placebo groups have looked at red clover isoflavones for treating vasomotor symptoms.
- In these studies, the doses of red clover isoflavones ranged from 40 to 160 mg and the treatment lasted between 12 to 16 weeks.
- All studies showed a numerical decrease in the number of hot flushes when compared to the placebo.
- However, only two out of the five studies showed results that were statistically significant.
- There were no major safety issues reported with the short-term use of red clover isoflavones in any of the studies.
- It seems that breast density is not negatively impacted by red clover, but long-term studies on the risk of breast cancer are still needed.
- There is a lack of data from endometrial biopsies, but ultrasound scans of endometrial thickness have shown positive results.
Black cohosh
- Black cohosh is a type of flowering plant that grows year-round and is originally from North America.
- It is commonly used to help with symptoms related to menopause.
- There have been four studies that randomly assigned participants to test black cohosh, but only one of them used a placebo for comparison.
- Out of these studies, three reported positive effects on vasomotor symptoms, which include hot flashes and night sweats.
- One study compared black cohosh to conjugated estrogens, a form of hormone therapy.
- However, more research is needed to confirm how effective black cohosh really is.
- Recently, there have been seven serious side effects linked to black cohosh, mainly related to liver damage.
- One of these cases was so severe that it required a liver transplant.
- It seems that black cohosh does not have an effect on the endometrium, which is the lining of the uterus.
- Currently, there are no clinical trials that study how black cohosh affects breast tissue.
Evening primrose oil
- Evening primrose oil contains a lot of gamma linolenic acid.
- This oil is commonly used by women.
- However, there is no proof that it is effective for menopause.
Dong Quai
- Dong quai, a plant native to southwest China and commonly used in traditional Chinese medicine, has been studied for its effects on menopausal symptoms.
- However, research indicates that it does not work better than a placebo for these symptoms.
- There have been reports of interactions between dong quai and medications like warfarin, as well as potential photosensitivity issues due to the presence of coumarins in the plant.
Ginkgo biloba
- Despite its widespread use, the evidence supporting its effectiveness for menopausal symptoms is limited.
- Some studies suggest that dong quai may have a positive impact on anxiety and depression.
- Claims regarding cognitive benefits in postmenopausal women require further validation through larger studies.
St John's Wort
- St John's Wort has been found to be effective for mild to moderate depression in peri- and premenopausal women, likely due to its SSRI-like effects.
- However, its impact on vasomotor symptoms during menopause is not yet proven.
- It is important to note that St John's Wort can interact with various medications, including warfarin and the contraceptive pill, as it induces cytochrome P450 enzymes in the liver.
Steroids
DHEA (Dehydroepiandrosterone):
- DHEA, or dehydroepiandrosterone, is a hormone that declines significantly with age, leading to the idea that DHEA replacement therapy could mitigate some aging effects.
- In the United States, DHEA supplements are becoming more popular for their potential anti-aging benefits.
- Some research suggests that DHEA supplementation may improve skeletal health, cognitive function, overall well-being, libido, and vaginal health.
- However, there is currently no evidence to support the use of DHEA for alleviating hot flushes.
- The short-term effects of DHEA supplementation are still under discussion, and the long-term risks associated with its use are not yet fully understood.
Progesterone Transdermal Creams:
- Progesterone creams derived from wild yam have been marketed as remedies for menopausal symptoms and as protectants for bone health.
- However, the claim that diosgenin found in yams can be converted to progesterone in the human body is inaccurate.
- Recent clinical studies have indicated that progesterone creams do not provide any benefit for vasomotor symptoms associated with menopause.
- Additionally, there has been no observed impact on bone mineral density from the use of these creams.
Vitamins and Minerals:
- Supplements containing vitamins such as E and C, along with minerals like selenium, are commonly used by postmenopausal women.
- However, there is a lack of strong evidence supporting their benefits for this population.
Homeopathy:
- While some case histories and studies show promising results, more research is needed to establish their efficacy.
- One recent study investigated a homeopathic approach to managing estrogen withdrawal symptoms in breast cancer patients, finding significant improvements in daily living scores and reductions in symptoms like fatigue and mood disturbances.
Acupuncture:
- A small trial involving 45 postmenopausal women tested the effects of shallow acupuncture, electro-acupuncture, and oral estrogen on hot flush frequency.
- All groups experienced a reduction in hot flush frequency, with the greatest symptom reduction observed in the estrogen group.
- No adverse effects were reported in the study, although rare risks associated with acupuncture, such as cardiac tamponade, pneumothorax, and hepatitis, have been noted in other research.
- Further research is needed to confirm the specific benefits of acupuncture for menopausal symptoms.
Reflexology:
- Reflexology is a practice that involves applying pressure to specific points on the feet to alleviate stress and address various health issues.
- While it has been used for a range of conditions, there is limited research on its effectiveness for menopausal symptoms.
- One trial involving 67 women experiencing vasomotor symptoms found that both reflexology and foot massage led to a reduction in symptoms.
- However, there was no significant difference between the two interventions in terms of their effectiveness.
Alternatives to HRT
Skeletal Protection
- In December 2004, the European Medicines Agency recommended that hormone replacement therapy (HRT) should not be the first-line treatment for osteoporosis.
- This view was supported by the MHRA in the UK, which highlighted that the long-term risks of HRT outweigh its benefits.
- As a result, alternative treatments for the prevention and treatment of osteoporosis have been suggested.
Lifestyle Measures
- Women are encouraged to engage in regular exercise, maintain a balanced diet, and avoid smoking to support their health, especially in relation to bone density.
- Studies have shown that women who exercise regularly tend to have higher bone mineral densities compared to those who do not.
- While exercise helps reduce bone loss, it does not reverse osteoporosis, and it also improves muscle tone, which lowers the risk of falls.
- Additionally, a daily intake of calcium (around 1500 mg) and vitamin D (400-600 IU) may help reduce bone loss.
Bisphosphonates
- Bisphosphonates are compounds that resemble pyrophosphate and function by inhibiting the activity of osteoclasts, the cells responsible for bone resorption.
- The initial bisphosphonate to receive approval was etidronate.
- However, alendronate and risedronate have become more prevalent due to their superior effectiveness.
- Both alendronate and risedronate are supported by strong evidence from grade A randomized controlled trials demonstrating their efficacy in preventing and treating spine and hip fractures, with a potential 50% reduction in fracture risk.
- Alendronate has long-term data demonstrating its effectiveness over 10 years.
- There is evidence of bone preservation in women who discontinue alendronate, although this is less pronounced than in those who continue the treatment.
- The primary side effects of bisphosphonates include gastro-oesophageal irritation and ulceration. However, once-weekly formulations have improved patient tolerance.
- New formulations are being developed to enhance patient compliance, such as a once-a-month option (ibandronate) and a once-a-year option (zoledronic acid).
Raloxifene
- Raloxifene is part of the Selective Estrogen Receptor Modulators (SERMs) group.
- It has positive effects on the skeleton and cardiovascular system but negative effects on the breast and endometrium.
- Raloxifene was the first SERM to be licensed and can modestly increase bone mineral density (BMD) by 2-3% per year.
- It is approved for reducing spinal fractures.
- However, it lacks strong evidence for preventing hip fractures, leading NICE to recommend it as a second-line option after bisphosphonates.
Strontium Ranelate
- Strontium ranelate functions as both an antiresorptive and anabolic treatment, offering a dual-action approach for bone health.
- Recently approved for treating fractures in the hip and spine, demonstrating a 41% reduction in spine fractures over three years.
- Unlike bisphosphonates, it does not cause gastrointestinal side effects.
Teriparatide
- Teriparatide, a synthetic parathyroid hormone analogue, also combines antiresorptive and anabolic effects and is approved for treating spine fractures.
- Teriparatide requires daily injections and is expensive.
- NICE recommends it as a third-line treatment for elderly women with severe osteoporosis who have a history of fractures.
Statins: Some studies suggest that statins may have an impact on bone health, but robust evidence from randomized trials in humans is still lacking.
FAQs on Chapter Notes: Menopause and the postmenopausal woman
| 1. What are the common symptoms of menopause and how long do they typically last? |  |
| 2. How does menopause affect bone health in postmenopausal women? | |
| 3. What is hormone replacement therapy (HRT) and what are its risks and benefits? | |
| 4. What lifestyle changes can help manage menopausal symptoms? | |
| 5. How can postmenopausal women maintain their sexual health and intimacy? | |



