NEET PG Exam > NEET PG Notes > Gynaecology and Obstetrics > Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse
Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse


Introduction
- Up to 50% of women may develop uterovaginal prolapse in their lifetime.
- 20% of these women experience symptoms and require treatment.
- An actuarial analysis in North America shows an 11% risk for women up to age 80 needing surgery for pelvic floor weakness.
- Women who undergo surgery for pelvic floor issues have a 29% chance of needing additional surgery.
- Current management of pelvic floor dysfunction is not optimal.
- As the global population ages, the prevalence of pelvic floor dysfunction is expected to rise.
- Gynaecologists need to enhance their understanding of pelvic floor dysfunction to improve treatment outcomes.
Structure and Function of the Pelvic Floor
- The pelvic floor supports pelvic and abdominal organs and helps control their contents.
- It consists of two main components: muscle and fascia, which work together.
Muscle
- The levator ani muscles consist of the pubococcygeus, coccygeus, and ileococcygeus muscles on both sides, creating a strong muscular pelvic floor.
- The levator ani is a type of striated muscle that we can control voluntarily, and it is special because it keeps a resting tension.
- You can enhance its strength through pelvic floor physiotherapy exercises.
- When these muscles contract, they help to lift the pelvic floor upwards, which supports continence.
- This lifting action increases the angle between the bladder and urethra in the front and between the rectum and anal canal at the back.
- Having a larger angle is an important factor in keeping things from leaking.
- When at rest, healthy pelvic floor muscles provide necessary support and help with continence.
- When there is more pressure in the abdomen, the levator ani muscles tighten up to give extra support and resist any pressure on the bladder and rectum.
- This tightening response relies on having a healthy nerve supply to the muscles.
- If there is damage to the nerves that control the pelvic floor muscles, it can affect how well the muscles work and respond.
Fascia
- Fascia surrounds the levator ani muscles, connecting them to the bones where they start and joining the two muscles in the center.
- The midline fascia allows the urethra, vagina, and rectum to pass through it.
- The levator ani muscles below and the fascia attachments support the pelvic organs.
- In certain areas, the fascia becomes thickened and forms ligaments such as the uterosacral, cardinal, and round ligaments.
- For over a century, there has been discussion about the structure and role of pelvic fascia.
- As humans began to stand upright, the pelvic floor adapted, with fascia taking over some muscle functions to offer extra support against gravity.
- Various factors that affect the strength or integrity of fascia can influence how the pelvic floor works.
- Congenital factors, like the excessive stretchiness of collagen in the fascia, can make the pelvic floor weaker.
- Environmental factors, such as stretching or tearing of the fascia during childbirth or heavy lifting, can also lead to weakness.
- Weakness in the pelvic floor muscles or fascia can result in uterovaginal prolapse.
- Issues with the pelvic floor can create symptoms that go beyond just organ displacement.
- It is important to understand the pathophysiology of pelvic floor dysfunction to create effective treatment options.
Pathophysiology of pelvic floor dysfunction
Muscle
- The pelvic floor muscles, like other striated muscles in the body, experience a slow loss of nerve connections as people get older.
- This nerve loss leads to a gradual weakening of the muscles over time.
- Although some effects of aging can be improved through muscle training, the loss of nerve connections decreases the number of neurons available to stimulate muscle fibers for contraction.
- Vaginal delivery can increase the risk of pelvic floor muscle nerve loss, especially if the active stage of labor is prolonged.
- On the other hand, having a Caesarean section may provide some protection against this type of injury.
- After childbirth, some nerve recovery can occur, which helps in the rehabilitation of the muscle to some extent.
- This reinnervation means that more muscle fibers receive signals from each remaining nerve fiber.
- However, this makes the pelvic floor muscles more susceptible to age-related nerve loss, leading to a more significant decrease in muscle activity as people age.
- Consequently, damage to the pelvic floor muscles during childbirth may only become noticeable when combined with the effects of aging.
- The exact location of nerve loss in the pelvic floor muscles during childbirth is not fully understood.
- It is suggested that stretching of the pudendal nerve near Alcock's canal at the ischial spine may cause nerve injury, but it is also possible that crushing injuries occur at the neuromuscular junction in the muscle.
- In conditions like multiple sclerosis, pelvic floor muscles may behave unpredictably, leading to issues such as inappropriate relaxation causing incontinence or spasms that result in difficulty with voiding.
- Women with ectopia vesicae have an incomplete development of the pelvic floor at the front.
- This condition makes them more likely to experience uterovaginal prolapse, which poses additional surgical challenges to treat, partly due to previous surgeries and partly due to anatomical changes from having an improperly formed anterior pelvis.
Fascia
- Fascia is made up of various parts, including collagen, elastin, and smooth muscle, all of which are found in a connective tissue framework.
- Each of these components can affect how the fascia behaves biomechanically.
- Several factors play an important role in providing support to the pelvic floor.
Congenital
- Congenital differences in collagen behaviour are clinically evident in women who have increased joint elasticity.
Joint hyperextensibility as an index of fascial stretchiness

- Women with hyperextensible joints may also experience added flexibility in their pelvic fascia, which can lead to uterovaginal prolapse at a younger age.
- These women often perform well in sports that require high joint flexibility, such as gymnastics.
- They tend to have fewer striae gravidarum (stretch marks) during pregnancy due to their increased skin elasticity.
- Labor may occur more quickly because there is less obstruction from the pelvic floor fascia.
- Extreme cases of this condition are seen in Ehlers-Danlos syndrome, but milder forms are much more common.
- It is crucial for gynecologists to identify women with these conditions, as their treatment may need to be adjusted.
- There is a higher chance of recurrence after surgery, and the use of prosthetic support materials may be recommended.
- Some types of collagen disorders are also linked to clotting problems.
Age
- As people age, the fascia tissues become stiffer and more likely to break.
- A young child typically has stiffer movements compared to an older adult.
- The fascia in the pelvic floor tends to provide less support as one gets older.
- Gynecologists who repair the pelvic floor often notice that the tissues they use for the repair are of poor quality and have low blood supply.
- After surgery, the healing process occurs with less strength and takes more time.
- About one in three cases of prolapse surgery leads to a recurrence. This is partly due to a decrease in the strength of fascia as people age.
- The longer the follow-up period after surgery, the greater the risk of recurrence.
Childbirth injuries
- Many women notice that their pelvic floor feels different after having a baby through vaginal delivery.
- Restoring the tone and shape of the front part of their abdominal wall can also be quite challenging.
- These changes happen because of a mix of changes in the muscles and the fascial tissues.
- There is ongoing debate about whether the pelvic floor fascia stretches or tears during pregnancy and childbirth.
- Some experts think that the fascia stretches, suggesting that when repairing the pelvic floor during prolapse surgery, it should include fascial pliability.
- Others believe that the fascia only tears and does not stretch, so the repair should focus on finding the sites of the tears and fixing them (this is called site-specific repair).
Endocrine
- The menstrual cycle, pregnancy, and menopause are key events in women's health that can affect the pelvic floor fascia.
- Many women report that symptoms of prolapse feel worse during their menstrual period.
- This is believed to be due to higher levels of progesterone, which increases the flexibility of the fascia.
- Recent research indicates that women who are examined during menstruation often show a more advanced stage of prolapse compared to other times in their cycle.
- This finding is important when making decisions about treatment.
- In pregnancy, prolapse symptoms are usually more noticeable in the first trimester but tend to lessen as the uterus grows and moves out of the pelvis.
- Many women experience stress incontinence for the first time during pregnancy.
- Studies have shown that during pregnancy, the elasticity of the fascia increases, which likely leads to reduced support for the pelvic floor and a higher chance of stress incontinence.
- Women who have stress incontinence during pregnancy are more likely to continue experiencing this issue after giving birth.
- The occurrence of uterovaginal prolapse increases after menopause.
- It is unclear how much of this increase is due to hormonal changes compared to natural aging processes.
Uterovaginal prolapse
Description
- Prolapse is typically categorized into three parts:
- Anterior compartment
- Uterine/Vault compartment
- Posterior compartment
- The anterior vaginal wall prolapse is often referred to as a cystocele, while the posterior prolapse is called a rectocele or enterocele.
- Because it can be hard to create clear descriptions for research purposes, scoring systems have been developed to help with this.
- The most commonly used and validated scoring method in current research is known as the POPQ (Pelvic Organ Prolapse Quantification System).
The system is shown diagrammatically
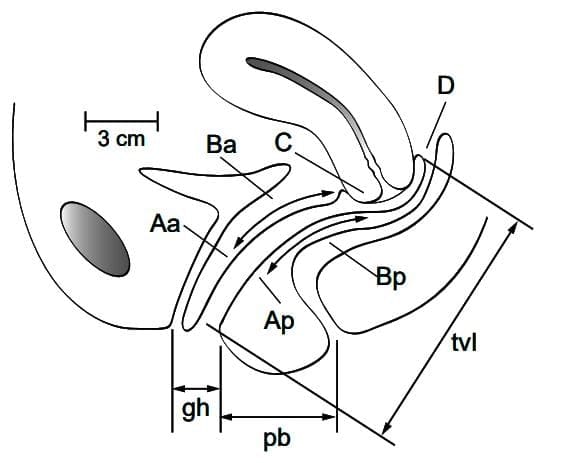
- Abbreviations: Aa, anterior wall; Ap, posterior wall; Ba, anterior wall; Bp, posterior wall; C, cervix or cuff; D, posterior fornix; gh, genital hiatus; pb, perineal body; tvl, total vaginal length.
Symptoms
- Prolapse typically causes a feeling of fullness in the vagina or a noticeable lump at the entrance.
- This feeling often changes based on posture, similar to other symptoms of prolapse.
- If the symptoms do not go away when lying down, it may indicate a different cause.
- Low back pain is a frequent symptom, but it can also occur in women who do not have prolapse.
- Vaginal atrophy, if it exists, can make many symptoms of prolapse worse.
- It is important to treat vaginal atrophy first with topical estrogen, unless there are medical reasons not to do so.
Urinary Symptoms
- An anterior vaginal wall prolapse can lead to various urinary symptoms.
- Women with this type of prolapse may experience stress incontinence, especially if the urethra is not properly supported.
- Additionally, they might have voiding issues caused by the kinking of the urethra.
- These voiding issues can lead to:
- Frequent urination due to not fully emptying the bladder.
- Hesitancy in starting to urinate.
- A weak urinary stream.
- Not being able to fully empty the bladder can cause recurrent urinary infections, which may bring about:
- Increased urgency to urinate.
- Urgency incontinence.
- It is crucial to understand that anterior vaginal wall prolapse does not directly cause detrusor overactivity, which may be due to another underlying problem.
- Therefore, fixing an anterior vaginal wall prolapse might not eliminate urinary symptoms if there are other issues involved.
- If the anterior prolapse is causing kinking of the urethra, it may actually be stopping stress incontinence from happening.
- After surgery to repair the anterior prolapse, it is possible for new stress incontinence to develop, which may upset the patient.
- Sometimes, a posterior vaginal wall prolapse linked to obstructed defecation can also cause problems with urination.
Bowel Symptoms
- Posterior vaginal wall prolapse can lead to various bowel symptoms.
- It can be challenging to determine if these bowel symptoms are caused directly by the prolapse or if they relate to fascial weakness that may also be impacting the bowel.
- Conditions like slow transit constipation and diverticular disease are more common in women who experience fascial weakness.
- Constipation is a frequent issue among women and can lead to obstructed defaecation.
- The presence of a posterior vaginal wall prolapse may not actually cause obstructed defaecation, but could instead be a sign of it.
- Typically, a posterior vaginal wall prolapse does not lead to ano-rectal incontinence.
Coital Symptoms
- Uterovaginal prolapse usually improves when a woman is lying down, except in severe cases.
- The condition generally does not affect normal sexual activity.
- Many women experience vaginal discomfort throughout the day, which can be distressing.
- The presence of prolapse may make some couples hesitant to engage in sexual activity, mainly due to concerns about appearance and potential harm.
- Worries about continence and other issues related to urine and bowel control might also contribute to this hesitation.
- Some couples may feel that the loss of vaginal tone leads to dissatisfaction in their sexual relationship.
- There is an increasing interest in cosmetic vaginal surgery and medications for male impotence, which may be affecting attitudes toward these issues.
Investigation of prolapse symptoms
Examination
- A general examination should check for fitness for surgery.
- A thorough abdominal examination is necessary to rule out any intra-abdominal mass.
- A bimanual pelvic examination or ultrasound should be conducted to check for any pelvic mass and to measure the size of the uterus and ovaries if they are present.
- The patient should be examined while lying down, preferably in the left lateral position using a Sims speculum.
- If there are no signs of prolapse, even when the patient performs a Valsalva maneuver, the examination should continue while the patient is standing.
- It is crucial to recreate the symptoms and signs that the patient reports.
- If symptoms cannot be reproduced, a further examination may be needed.
- Many women only notice their symptoms after being in an upright position for a long time.
- Appointments early in the morning may make it difficult to detect a prolapse.
- Some healthcare providers examine women in the lithotomy position for a closer look at vaginal supports, especially when searching for specific issues in the endopelvic fascia.
- A second retracting instrument will be needed to see the lateral sulci clearly.
- The POPQ examination provides an objective record of the stage of prolapse.
Urodynamics Studies
- If a woman does not have any urinary symptoms, urodynamic studies are not recommended outside of research.
- When a woman experiences significant urinary symptoms, urodynamics can help identify the cause, allowing the gynecologist to provide guidance on treatment.
- If the urodynamic tests show obstructed voiding, there is a good chance that surgery to repair the cystocele will fix the voiding issues.
- However, if the urodynamics reveal that the bladder is atonic, the outlook for improvement is less promising.
- Should the urodynamics indicate that the bladder is overactive, surgery is unlikely to help with urinary symptoms.
- This information can affect a woman's choice about whether to go ahead with surgery.
- After undergoing anterior vaginal wall repair, some women may develop stress incontinence, which can be bothersome.
- Some doctors conduct a urinary stress test while the prolapse is reduced, using either digital methods, sponge forceps, or a ring pessary.
- There is no solid evidence that this testing method can accurately predict which women will experience stress incontinence following surgery.
Proctography
- An anterior rectocoele can cause problems with defecation.
- Rectal mucosal prolapse can also lead to difficulty in defecation and may not be detected during a vaginal examination.
- Proctography can provide useful information about what might be causing issues with defecation.
- This procedure may help prevent unnecessary and ineffective vaginal surgeries.
Magnetic Resonance Imaging
- Magnetic resonance imaging is a tool used in research.
- It aims to find prolapse that is not visible during clinical examinations.
- As of now, there is no evidence that it helps improve treatment results.
Treatment
Conservative
- Some women choose non-surgical options for treating their prolapse for several reasons:
- Unsatisfactory Treatment Prognosis: They may feel that the expected results from surgical treatment are not appealing enough.
- Health Concerns: They may not be healthy enough to undergo surgery.
- Desire to Delay Surgery: They might want to postpone surgery for personal reasons.
- Conservative Treatment Options may include:
- Lifestyle Changes:
- Suggestions on diet and weight management.
- Avoiding drinks with caffeine.
- Maintaining proper water intake and fiber consumption.
- Using laxatives wisely and adjusting medication like diuretics.
- Refraining from high-impact exercises and heavy lifting to alleviate symptoms.
- Pelvic Floor Physiotherapy:
- No studies confirm the effectiveness of pelvic floor exercises for vaginal prolapse symptoms.
- While severe prolapse may not benefit, early-stage prolapse might improve enough to avoid surgery.
- Vaginal Pessaries:
- Pessaries have been used for about 4000 years, with the first ones made from pomegranate skins.
- The most common type in the UK is the polypropylene ring pessary.
- The best fit for the ring pessary is not clearly defined; if there is little support in the back area, it may not stay in place.
- Finding the right size often requires some testing.
- There is no established schedule for changing pessaries, and the use of topical estrogen is also not well-defined.
- In North America, a wider variety of vaginal pessaries is available (see www.milexproducts.com).
- Patients are advised to wash their pessaries regularly, though there is no proof that this is necessary.
- Sexual Activity Considerations:
- Ring pessaries usually allow for sexual intercourse without issues, although some women prefer to take them out during sex.
- Space-filling pessaries, like the shelf pessary, can interfere with sex, making them unsuitable for sexually active women.
- Shelf pessaries may be especially useful for uterine or vaginal vault prolapse.
- They can be challenging to change and may become stuck in the vaginal wall.
- Regular check-ups every six months are recommended, and using topical estrogen may help lower the risk of sores and erosion.
Ring

Surgical
- For the past 100 years, surgery has been the main treatment for uterovaginal prolapse.
- The surgical methods used today are not very different from those used by famous surgeons a century ago.
- More people are realizing that a good result from surgery should involve more than just having the right anatomy.
- How well a person is able to function after surgery might be even more important to them.
- There have been very few strong studies on prolapse surgery that look at both the anatomical results and how well patients can function, including how it affects their quality of life.
- More research is needed in this area.
- Key Surgical Questions
- Which technique gives the best and longest-lasting anatomical result?
- Does using synthetic support material help in surgery?
- Is the abdominal approach better than the vaginal approach?
Anterior vaginal wall prolapse
- In 1909, White described the vaginal paravaginal repair to fix a cystocele.
- Four years later, Kelly introduced the anterior vaginal repair, which involved a central pleating of the pubocervical fascia.
- The Kelly operation became the preferred method for treating anterior prolapse due to its simplicity and Kelly's esteemed reputation in the surgical field.
- The discussion about the benefits of the Kelly repair versus the paravaginal repair still continues today.
- A literature review by Weber and Walters, covering over 90 articles from 1966 to 1995, showed gaps in the research and concluded that there was no significant difference in success rates between the paravaginal repair (failure rate of 3-14%, whether done vaginally or abdominally) and the central plication repair (failure rate of 0-20%).
- Beck reviewed 246 anterior repairs and found that 5% of women experienced new stress incontinence and another 5% had new detrusor overactivity after surgery.
- Less than 1% of patients reported long-term voiding issues.
- Post-operative fever occurred in 10% of women, but overall, the rate of complications was low.
- A few studies have been published on using additional support materials like polypropylene mesh to enhance the anterior vaginal repair.
- These results indicate a lower chance of recurrence but come with a higher risk of mesh erosion.
- It seems that the best mesh material has not yet been developed, and using support materials in initial repairs does not appear to be justified
Posterior vaginal wall prolapse
- Posterior vaginal wall prolapse typically involves a surgical method known as classical posterior vaginal repair. This procedure not only tightens the tissue beneath the vaginal skin but also involves stitching the fascia that covers the pubococcygeus muscle, which may even include the muscle itself.
- Including the pubococcygeus fascia and muscle in the repair is likely to provide a stronger fix, which can lead to more complications both during and after surgery. However, it is uncertain if this approach leads to improved functional results.
- In a study by Kahn and Stanton, which followed up two years after the conventional posterior vaginal repairs (that included levator plication), it was found that:
- One in four women showed signs of posterior prolapse during examination.
- More women reported problems with bowel function and painful intercourse compared to before the surgery.
- Some experts suggest that using a transanal method for repairing rectoceles might work better for issues with bowel movements, but existing studies do not strongly support this idea.
- There are few studies focused on the effectiveness of adding support materials to a posterior vaginal wall repair. The potential risk of mesh erosion needs to be considered against the possible advantage of reducing the chance of the condition returning.
- Perineal descentis often observed with posterior vaginal wall prolapse.
- While its clinical importance is not fully understood, it indicates either:
- The perineum is no longer supported by the pelvic floor.
- There is a weakness in the pelvic floor overall.
Uterine prolapse
- The usual method for treating uterine prolapse in women who do not want more children is a vaginal hysterectomy, along with any necessary repairs to the vaginal walls.
- After the hysterectomy, the vaginal vault is supported by reconnecting the uterus and cardinal ligaments to the vagina.
- These ligaments can also be tightened in the middle to help prevent enterocele from forming.
- The Manchester repair used to be common but is now less favored. This method involved bringing the cardinal ligaments together in front of the cervix, which was removed during the operation.
- A major issue with using the uterine and cardinal ligaments is that their weakness has caused the prolapse in the first place.
- Using these weak tissues raises the risk of the prolapse coming back.
- There is no proof that preserving the uterus through methods like abdominal sacrohysteropexy or sacrospinous hysteropexy reduces the chance of the prolapse returning.
- Additionally, there is no evidence that performing a routine sacrospinous colpopexy during a hysterectomy lowers the risk of vault prolapse, even though this procedure may have more complications.
- This implies that, without evidence suggesting otherwise, a gynecologist should carry out a vaginal hysterectomy and provide support for the vaginal vault using the uterosacral ligaments.
- If there is no defined support tissue, a sacrospinous colpopexy or sacrocolpopexy might be necessary.
Vaginal vault prolapse
- Vaginal vault prolapse happens in about 5% of women after having a hysterectomy.
- Studies show that a similar number of women have had either an abdominal or a vaginal hysterectomy.
- Since abdominal hysterectomy is done more often than vaginal hysterectomy, it indicates that vaginal hysterectomy may lead to vault prolapse.
- Vault prolapse is usually linked with some level of anterior and posterior vaginal prolapse, with posterior being the most common type.
- There is often significant stretching of the vaginal wall, particularly in the posterior area.
- If extensive vault prolapse is not treated, it could result in ulceration and, in rare cases, bowel extrusion.
- Treatment for vaginal vault prolapse can include a surgical procedure known as sacrospinous colpopexy or an abdominal (or laparoscopic) sacrocolpopexy.
- A Cochrane review found that sacrocolpopexy has a higher success rate, but if it fails, it tends to fail sooner than sacrospinous colpopexy.

- Dyspareunia (pain during intercourse) seems to happen more often after sacrospinous colpopexy.
- Both surgical options do not significantly differ in terms of urinary and bowel symptoms after surgery.
- Sacrocolpopexy usually requires a longer recovery period, especially when done as an open procedure, making it more expensive.
- The frequency of adverse events appears to be similar for both procedures, and patient satisfaction rates are alike.
- Both surgeries can lead to large amounts of bleeding-from the sacrum for sacrocolpopexy and from the pudendal vessels for sacrospinous colpopexy.
- There is mixed evidence about which procedure results in a better anatomical correction.
- Mesh erosion is a notable issue after sacrocolpopexy and may sometimes require the complete removal of the mesh.
- Colpocleisis is a rare option where the vaginal canal is completely closed; it is considered for women who cannot undergo major surgery and have not responded to other treatments.
- During colpocleisis, strips of vaginal skin are removed from both the anterior and posterior walls, and then they are stitched together.
The document Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse is a part of the NEET PG Course Gynaecology and Obstetrics.
All you need of NEET PG at this link: NEET PG
FAQs on Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse
| 1. What is pelvic floor dysfunction and how does it relate to uterovaginal prolapse? |  |
Ans. Pelvic floor dysfunction refers to a range of disorders that affect the muscles and tissues of the pelvic floor, which support the bladder, uterus, and rectum. Uterovaginal prolapse is a specific type of pelvic floor dysfunction where the uterus and, in some cases, the vagina, descend into the vaginal canal due to weakened pelvic support structures. This condition can result from factors such as childbirth injury, congenital issues, and hormonal changes associated with aging and menopause.
| 2. What are the common symptoms of uterovaginal prolapse? | |
Ans. Common symptoms of uterovaginal prolapse include a feeling of heaviness or pressure in the pelvic area, bulging or protrusion of the vaginal wall, urinary incontinence or urgency, difficulty with bowel movements, and discomfort during sexual activity. Some women may also experience lower back pain and a sensation of incomplete bladder emptying.
| 3. How does childbirth contribute to the development of uterovaginal prolapse? | |
Ans. Childbirth can significantly contribute to the development of uterovaginal prolapse due to the physical stress and trauma exerted on the pelvic floor muscles and connective tissues during delivery. Factors such as the size of the baby, prolonged labor, and the use of forceps or vacuum extraction can increase the risk of injury to the pelvic support structures, leading to weakened support and potential prolapse.
| 4. Are there any non-surgical treatments available for uterovaginal prolapse? | |
Ans. Yes, there are several non-surgical treatment options for uterovaginal prolapse. Pelvic floor exercises, such as Kegel exercises, can strengthen the pelvic muscles. Pessary devices can be used to support the pelvic organs. Lifestyle modifications, such as weight management and avoiding heavy lifting, can also help mitigate symptoms. Hormonal therapy may be considered to improve tissue health in postmenopausal women.
| 5. What role do congenital conditions play in uterovaginal prolapse? | |
Ans. Congenital conditions can predispose individuals to uterovaginal prolapse by affecting the structural integrity of the pelvic floor. Some women may be born with weaker connective tissues or anatomical variations that result in inadequate support for pelvic organs. These inherent weaknesses can be exacerbated by factors such as pregnancy, childbirth, and aging, leading to the onset of prolapse symptoms.
About this Document

4.61/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse for NEET PG 2026 is part of Gynaecology and Obstetrics preparation. The notes and questions for Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse covers topics like and Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse.
Introduction of Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse in English is available as part of our Gynaecology and Obstetrics for NEET PG & Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse in Hindi for Gynaecology and Obstetrics course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse
Description
Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse of Gynaecology & Obstetrics with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET PG exam.
Information about Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse
In this doc you can find the meaning of Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse defined & explained in the simplest way possible. Besides explaining types of Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse theory, EduRev gives you an ample number of questions to practice Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse tests, examples and also practice NEET PG tests


Related Searches
Sample Paper, past year papers, Semester Notes, pdf , ppt, Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse, video lectures, study material, Free, practice quizzes, Objective type Questions, Viva Questions, Extra Questions, Exam, Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse, MCQs, Previous Year Questions with Solutions, mock tests for examination, Important questions, Summary, shortcuts and tricks, Chapter Notes: Pelvic floor dysfunction I: Uterovaginal prolapse;