Chapter Notes: Hysteroscopy and laparoscopy

Introduction
- The most significant change in gynaecological surgical practice over the last 20-30 years is endoscopic surgery.
- Pioneers like Semm and Lindemann from Germany, Bruhat and Hamou from France, Sutton from England, and Reich, Neuwirth, and
- Goldrath from the United States have transformed modern gynaecological surgery since the 1970s and 1980s.
- This change is marked by the understanding that many patients who would have previously undergone laparotomy or hysterectomy can now be treated with laparoscopic or hysteroscopic surgery.
- Minimal Access Surgery (MAS) has had a profound impact on various aspects of gynaecology, including diagnosis, therapy, reproductive medicine, urogynaecology, and oncology.
- The benefits of MAS include reduced post-operative pain, shorter hospital stays, and quicker return to normal activities.
Instruments and Equipment for Endoscopy
- Endoscopic surgery depends significantly on the surgeon's skill and advanced technology, even more so than traditional surgery.
- The early vision of pioneers in this field was heavily reliant on advancements in:
- Optics
- Illumination
- Video technology
- Instrumentation
- There has always been a close relationship between endoscopic surgeons and the industry, making the tools and equipment for Minimally Invasive Surgery (MAS) essential to the surgical process.
- Surgeons need to have a deep understanding of:
- The fundamental physical principles
- How equipment is assembled and connected
- When and how to use specific instruments
- How to respond to equipment malfunctions
Equipment common to hysteroscopy and laparoscopy
Light Source and Light Lead
- Good lighting is vital for endoscopic surgery. Factors like the power of the light source and the transmission quality of the light lead, as well as the size and characteristics of the tissue being illuminated, are crucial.
- Laparoscopy requires brighter lights to illuminate larger areas compared to hysteroscopy, especially in cases of bleeding, as blood absorbs light.
- Modern xenon generators have replaced older tungsten and metal halide sources and should be set to maximum brightness during surgery.
- The light source should not be turned off between cases but put on standby to extend the bulb's life.
- While modern bulbs can last hundreds of hours, a spare bulb should always be available in the operating theatre in case of failure.
- Light leads can be fibre optic or liquid. Fibre optics are more common and less expensive but can break, affecting light transmission, so they should be handled carefully. Liquid light leads are more durable but can be damaged if punctured.
- Despite being called 'cold light fountains', the light from these systems can still be warm enough to burn drapes or patients if left in contact.
Camera and Monitor System
- The introduction of video cameras and high-resolution monitors in the 1980s significantly improved endoscopic surgery by allowing everyone in the operating room to see the procedure, facilitating better assistance and teaching.
- Before this advancement, only the surgeon could see the procedure, making it challenging for others to assist effectively.
- Early cameras have evolved into 3-chip cameras, with video laparoscopes now available, although they are not yet widely used.
- Functions like zoom, white balance, and still images can usually be controlled through the camera.
- Some cameras can be sterilised, while others require a sterile sleeve for protection.
- The camera connects to a control unit, which links to a high-resolution monitor, as ordinary TVs offer much lower quality images.
Electrosurgical Generator
- Electrosurgery, commonly known as diathermy, has been utilized in surgical procedures for over 100 years.
- It is essential for haemostasis (stopping bleeding) and cutting, especially in hysteroscopic and laparoscopic surgeries.
- The modern solid-state generator is designed to safely and effectively deliver a high-frequency current at low voltage, differing significantly from older spark generators.
- Modes of Operation:
- Bipolar electrosurgery
- Monopolar cutting (includes pure cut and blended cut)
- Monopolar coagulation (includes desiccation, fulguration, and spray)
- Bipolar coagulation is frequently used in laparoscopy for achieving haemostasis, while the resectoscope is typically a monopolar tool. Although this chapter cannot cover all aspects of electrosurgery, the following practical points are useful for endoscopic surgeons:
- Independent Circuits: The bipolar, monopolar cutting, and monopolar coagulation are three separate circuits within the generator. For example, the settings for the monopolar cutting waveform do not affect the monopolar coagulation circuit.
- Safety: Bipolar electrosurgery is generally safer than monopolar because the electrical current only flows between the electrode prongs, not between the electrode and the patient plate. It is advisable to use bipolar electrosurgery whenever possible.
- Power and Voltage: Always use the lowest power and voltage necessary to achieve the desired result. The bipolar circuit operates at the lowest voltage, while monopolar coagulation uses the highest voltage, with monopolar cutting in between. Higher voltage can lead to sparking, making bipolar electrosurgery the safest option, especially in tight spaces like the pelvis.
- No Patient Plate Required: Since bipolar electrodes consist of both the active and return electrodes, there is no need for a patient plate when using bipolar electrosurgery.
- Cut and Coagulation Misnomers: The terms "cut" and "coagulation" can be misleading. Cutting happens due to electrical arcing between the electrode and tissue, causing vaporization and cell disruption. Coagulation occurs when the electrode touches the tissue, leading to heating and coagulation. These effects are independent of the current waveform, meaning both cutting and coagulation can be achieved with a cutting current. Keeping the electrode off the tissue results in cutting, while contact with tissue produces coagulation. Using monopolar cut for coagulation is generally safer than using monopolar coagulation, though it might be less effective.
- Further Information: Additional practical aspects of electrosurgery will be discussed later in this chapter. Electrosurgery is a highly valuable tool, and further study on the topic is strongly encouraged (see Further Reading).
Laser
- Lasers, which stands for light amplification by stimulated emission of radiation, have always seemed intriguing, possibly because they are costly and only accessible to a limited number of people.
- Unlike electrosurgery, lasers are not essential for successful endoscopic surgery, as there is no proof that they provide better results.
- However, in certain situations, like when working near important structures, lasers may be a safer option because they usually cause less heat spread (for example, the CO2 laser).
- With lasers, issues such as distant burns, insulation failures, and capacitive coupling do not occur.
- On the downside, lasers are generally less effective for haemostasis compared to diathermy.
- There are several types of lasers used in endoscopy, but the most common ones for laparoscopy are:
- CO2 laser
- Nd: YAG (Neodymium:yttrium aluminium garnet)
- Argon laser
- KTP (potassium titanyl phosphate) laser
- The CO2 laser is an optical laser that uses a tube with mirrors to deliver the beam. It is almost entirely absorbed by water, making it very precise for laparoscopy with minimal heat spread.
- However, CO2 lasers are not very good at stopping bleeding, and the optical arm required can make them difficult to handle and easy to misalign.
- The Nd: YAG laser is a fibreoptic laser, which makes it easier to use. Since this laser is not easily absorbed by water, it can be used for both hysteroscopic and laparoscopic procedures.
- Due to its properties, the Nd: YAG laser tends to have greater heat spread, making it better for coagulating tissue rather than vaporizing it.
- To improve precision and reduce tissue penetration, a sapphire tip can be added to the end of the fibreoptic cable.
- The argon and KTP lasers are also fibre lasers, and their effects on tissue fall between those of the CO2 and Nd: YAG lasers.
Photo and Video Documentation
- The widespread use of video cameras in endoscopic surgery allows for the recording of still images, short clips, or even complete procedures.
- Photographs serve as helpful clinical records that can be shared with patients and discussed with colleagues for obtaining a second opinion.
- Video recordings are valuable resources for teaching, conducting research, evaluating performance, and assessing tools used during surgery.
- For example, we record all our surgeries and keep those recordings for at least two weeks. This allows us to review any surgery if a post-operative complication occurs to identify potential causes during the operation.
- It's no surprise that manufacturers of surgical instruments offer equipment for capturing photos and videos.
- Modern systems have moved from analog to digital recording. These typically include a modified computer equipped with a touch screen, a DVD writer, and a color printer.
- While these commercial systems are convenient, they tend to be expensive and have limited capacity for continuous recording due to their small memory.
- Alternatively, you can build a digital recording system using a regular personal computer, which can have a recording capacity that is hundreds of times greater, depending on the size of the hard drive.
- It is important to follow local guidelines when making any visual recordings of patients.
- In the UK, for example, the General Medical Council has given guidelines stating that for laparoscopic images or images of internal organs, patients do not need to give permission or consent as long as the recordings are anonymized by removing any identifiable marks.
Equipment for Hysteroscopy
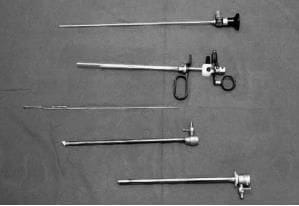
Hysteroscopes
- There are two types of hysteroscopes: Rigid and flexible.
- However, most gynaecologists prefer rigid hysteroscopes because they offer better images, are more durable, can be used with a resectoscope, and are less expensive.
- Rigid hysteroscopes usually have a Hopkins rod-lens optical system, while flexible ones use optical fibres.
- They come in various outer diameters, with 4 mm and 2.9 mm being common. Rigid hysteroscopes are available at different angles, such as 0°, 12°, 15°, or 30°, with oblique view ones being ideal for uterine work.
- For procedures other than contact hysteroscopy, a sheath is required to assist with uterine distension.
- Continuous flow sheaths facilitate irrigation and suction during surgery, using an inner sheath for inflow and an outer sheath for outflow.
Uterine Distension:
- The uterine cavity needs to be distended under pressure for a clear view during hysteroscopy. This can be achieved using gas (such as CO2) or low-viscosity fluids like normal saline, 5% dextrose, 1.5% glycine, 3% sorbitol, or 5% mannitol. High-viscosity fluids like Hyskon are also an option.
- Diagnostic hysteroscopy often uses CO2 or normal saline, while operative hysteroscopy typically involves normal saline. Resectoscopic surgery may use electrolyte-free solutions like glycine, sorbitol, or mannitol.
- The typical pressure for clear visualization is around 100 mmHg, but factors like an enlarged uterus may require higher pressure. Distension methods include gravity, pressure bags, or specialized hysteroscopic pumps.
- Modern pumps can control pressure and monitor fluid levels to reduce the risk of fluid overload.
- When using CO2, a specific hysteroscopic insufflator is necessary to prevent excessive pressure and flow.
Mechanical Instruments:
- Small, flexible or semi-rigid instruments such as scissors, grasping forceps, and monopolar electrodes are used for minor procedures during hysteroscopy.
- These instruments are delicate, typically ranging from 7 to 5 Fr gauge (with 3 Fr equal to 1 mm), so it is important to have replacements available in case they break.
- Despite their size, these instruments are generally safe and unlikely to cause harm to the patient.
Resectoscope
- The resectoscope, introduced by Robert Neuwirth in 1978, is a valuable tool for removing small fibroids and has become versatile for various gynecological procedures. The modern resectoscope consists of five parts: optic, handle mechanism, inflow and outflow sheaths, and an electrode. A passive handle is preferred for hysteroscopy as it keeps the electrode hidden and safe. The typical outer diameter is 26 or 27 Fr gauge (8.7-9 mm), using a 4-mm oblique optic.
- Electrodes come in various designs, such as cutting loops for polypectomy and knife electrodes for metroplasty. Power settings for monopolar electrosurgery typically range from 100 to 120 W to minimize tissue damage.
 A continuous flow resectoscope with a passive handle mechanism
A continuous flow resectoscope with a passive handle mechanism
Versapoint
- Bipolar resectoscopes are being introduced in the field, but the Versapoint system, developed by Gynecare in the USA, is already available for use.
- This system relies on 5 Fr electrodes of various designs, such as spring, twizzle, and ball, along with a specialized electrosurgical generator.
- The Versapoint can be used with a standard rigid hysteroscope or a dedicated Versascope for procedures like:
- Polypectomy
- Myomectomy for small intracavitary fibroids
- Metroplasty
- Being a bipolar instrument, the Versapoint allows for the use of physiological solutions like saline and Hartman's solution for uterine distension during procedures.
Laser Hysteroscope
- The initial clinical use of lasers in intrauterine surgery was documented by Goldrath et al. Using laser energy for hysteroscopic surgery offers advantages over the monopolar resectoscope, as it allows the use of distension media like saline.
- The preferred energy source is the Nd: YAG laser, with the fiber passed through the operating channel of a standard hysteroscope and used for:
- Contact mode: To vaporize tissue
- Non-contact mode: To coagulate tissue
- However, the popularity of laser intrauterine surgery has declined due to factors such as:
- High costs
- Longer operating times
- Increased rates of equipment failure
Equipment Used in Laparoscopy
Laparoscopes
- Laparoscopes typically employ a rod-lens system and are available in diameters ranging from 3 to 12 mm, with viewing angles between 0° and 30°.
- The 10 mm 0° scope is the most commonly used.
- Although fibre-optical micro-laparoscopes are an option, they are delicate and offer inferior image quality.
- Operating laparoscopes come with an additional channel for instruments or lasers; however, many gynaecologists prefer multipuncture methods.
- Videolaparoscopes equipped with CCD chips are still relatively new and costly for widespread adoption.
Veress Needle
- The Veress needle is instrumental in filling the abdomen with gas at the beginning of a laparoscopy.
- Developed by Hungarian chest physician Veress in the 1930s, this needle minimizes the risk of damaging the bowel or major blood vessels.
- While it is typically inserted through the abdomen, in obese patients, it can be introduced via the uterine fundus.
- Veress needles are available in both reusable and disposable variants.
Trocar and Cannula
- Trocars and cannulae are essential for providing access for the laparoscope and other surgical instruments.
- These instruments come in various sizes, with 5 mm and 10-12 mm sizes being the most prevalent.
- Traditionally constructed from surgical steel and designed for reuse, there is an increasing availability of disposable plastic options.
- Disposable systems often require less force for insertion, while designs featuring expanding sleeves result in smaller fascial defects.
- Non-disposable cannulae are equipped with valves to prevent gas leakage; however, these valves can potentially damage instruments, leading to a preference for simpler valves in modern disposable options.
Laparoscopic Insufflator
- Most gynaecologists opt for CO2 pneumoperitoneum, despite some advocating for gasless laparoscopy.
- Contemporary insufflators are advanced, computerized versions of earlier designs by Kurt Semm in the 1970s.
- These devices regulate intra-abdominal pressure, which is ideally maintained between 12 and 15 mmHg, although initial pressures can be increased up to 25 mmHg to mitigate injury risks.
- Some modern insufflators offer features like CO2 warming and smoke traps for CO2 laser surgeries.
Suction/Irrigation Pump
- A suction/irrigation pump is a vital tool in various procedures, capable of tasks such as removing blood, cleaning the pelvic area, deflating ovarian cysts, and providing assistance in complex cases.
- While a basic system may suffice, a high-pressure unit is recommended for surgeons specializing in serious laparoscopic procedures.
Ancillary Instruments
- There is a wide range of both disposable and non-disposable instruments available for use in laparoscopy.
- While 5 mm instruments are commonly used, larger instruments are necessary for specific tasks such as retrieval bags and morcellators.
- Atraumatic 5-mm grasping forceps are essential, with a preference for those that are easy to lock and unlock.
- Sharp scissors, particularly curved Mayo scissors, are also important tools in surgical procedures.
- A suction/irrigation cannula is typically required, along with bipolar forceps for haemostasis.
- Scissors can be used for electrosurgery, but caution is needed to avoid burns.
- Other haemostasis options include clips and staples, while newer devices like the harmonic scalpel and Ligasure device are available for dissection and haemostasis.
- Pre-tied Loop Sutures and Retrieval Bags.
- For major procedures involving haemostasis and repair, it is essential to have pre-tied loop sutures, suture carriers, and needle holders readily available.
 5-mm laparoscopic grasping forceps
5-mm laparoscopic grasping forceps
Retrieval Bags:
- Retrieval bags are invaluable for removing larger masses from the pelvis, such as intact ovarian cysts.
- Using a retrieval bag can be more efficient than making larger incisions for removal.
- Once the specimen is secured in the bag, it may be easier to extract it through a posterior colpotomy.
- Gynaecologists may find it advantageous that not all patients have this exit route unless the Pouch of Douglas is obliterated.
Powered Morcellators:
- Powered morcellators present an alternative for tissue removal.
- While smaller diameter morcellators can be effective, they may be time-consuming.
- Larger morcellators are more efficient but may leave a relatively large external scar.
Organization of the Operating Theatre
Hysteroscopy
- Diagnostic hysteroscopy is typically performed on an outpatient basis.
- Minor surgical procedures can often be carried out with local anaesthesia.
- More complex surgeries, such as hysteroscopic myomectomy, usually require general anaesthesia.
- It is essential to adhere to basic principles, including:
- Ensuring all necessary equipment is on a surgical cart.
- Positioning the monitor at a comfortable height for the operator and the patient, if they are awake.
- For procedures where fluid balance is crucial:
- Use a collecting drape under the buttocks to prevent cervical leakage of irrigant.
- Designate a staff member to monitor fluid balance, ensuring no air bubbles enter the inflow tubing to mitigate the risks of air embolism and serious complications.
Laparoscopy
- Laparoscopy involves a more intricate setup compared to hysteroscopy because it requires a larger amount of equipment.
- Similar to laparotomy, laparoscopy necessitates the presence of assistants, and their positioning can vary based on personal preference.
- Most laparoscopists favor using 0° optics, which allows one assistant to stand opposite the patient to control the laparoscope. This configuration enables the lead surgeon to operate with both hands free.
- Some surgeons, including the author, prefer using a 30° laparoscope for improved visibility from different angles.
- However, this can make the oblique view more challenging, leading to a preference for the surgeon to control the laparoscope themselves.
- The first assistant typically plays a crucial role in holding and retracting tissue during the surgery.
Diagnostic Hysteroscopy
- Diagnostic hysteroscopy is now a standard procedure in modern gynecology, replacing the traditional D&C (dilation and curettage).
- This procedure can be performed as an outpatient treatment, making it a key part of a One-Stop method for handling menstrual issues.
- Hysteroscopy allows for a nearly immediate diagnosis, and it serves as a logical first step before any operative hysteroscopy is done.
- The Royal College of Obstetricians and Gynaecologists (RCOG) has acknowledged the significance of diagnostic hysteroscopy, and it is now included in the essential training for this field.
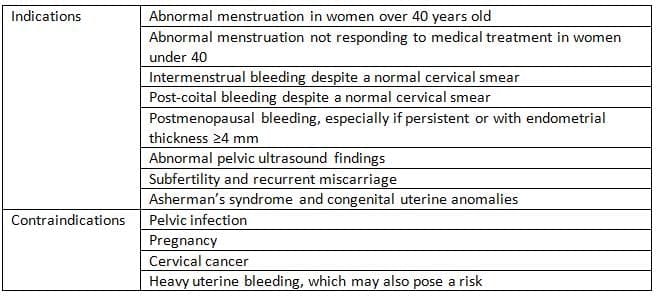
- The indications and contraindications for this procedure are limited and are listed.
- The best time to perform hysteroscopy is right after the menstrual period, but it is generally possible to make a diagnosis at any time, even during menstruation.
- Using liquid distension has several benefits compared to using CO2.
Technique Details
- The patient should be positioned correctly, specifically in the lithotomy position, where the hips are nicely bent and the buttocks are slightly beyond the edge of Show the table. This setup allows for clear access regardless of the uterus's position.
- The perineum and vagina are typically cleaned with a warm antiseptic solution, though some may choose not to clean the vagina at all.
- It is rare to cover the perineum, legs, and lower abdomen completely with drapes.
- A gentle bimanual examination should be performed to check the size and position of the uterus.
Indications and Contraindications
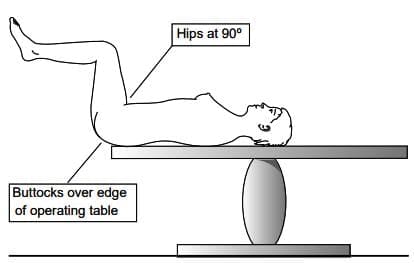 Patient position forhysteroscopy
Patient position forhysteroscopy
Conventional Technique
- Cervical Preparation: Speculum is inserted into the vagina to visualise the cervix, and the anterior lip of the cervix is grasped with a tenaculum. The cervix and uterine cavity are then sounded.
- Hysteroscope Insertion: The hysteroscope is inserted into the uterus, either with or without prior cervical dilation, depending on the size of the cervical canal. This technique can be adapted for outpatient settings, with local anaesthesia options if necessary.
- Visual Inspection: Once inside the uterine cavity, the hysteroscope allows for systematic inspection of the fundus, tubal areas, and the four walls of the uterus. Adjustments to the angle and approach may be needed based on the type of optic used.
- Post-Procedure: After inspecting the uterine cavity, the hysteroscope is withdrawn, and the endocervical canal is examined. If needed, a biopsy can be performed using a small curette or a device like a Pipelle, or by switching to an operative sheath for targeted biopsy.
 Collin speculum
Collin speculum
'No Touch' Hysteroscopy and Biopsy
- An alternative method for hysteroscopy is known as 'no touch' or vaginoscopic hysteroscopy.
- This technique is well-suited for use in outpatient clinics as it reduces patient discomfort.
- The reason it minimizes discomfort is that no extra instruments, like a speculum or tenaculum, need to be inserted into the vagina.
- In this method, the tip of the hysteroscope is placed at the vaginal opening.
- A low-viscosity distension medium is then activated to help with visualization.
- The hysteroscope is carefully guided to the external cervical os, moving along the cervical canal and into the uterine cavity.
- This method is effective for most patients, except in cases of cervical stenosis.
- Typically, there is no need to pause for local anesthesia during the procedure.
- Because of its advantages, this has become our standard method for outpatient hysteroscopy.
- It is now also possible to perform an endometrial biopsy using the 'no touch' technique without needing to insert instruments into the uterus.
- The Pipelle device is used for this purpose, and the H Pipelle (from Laboratoire C.C.D., France) is about twice as long but slim enough to fit through a narrow diagnostic sheath.
- At the end of the hysteroscopy, the hysteroscope is not completely removed from the cervix.
- The diagnostic sheath is then unlocked, and the optical part is taken out and replaced with the H Pipelle.
- The H Pipelle is then pushed through the sheath into the uterine cavity.
- Once the tip reaches the uterine fundus, the sheath is pulled out of the cervix.
- An endometrial biopsy is then taken in the usual way.
How to insert an oblique view hysteroscope into the uterus.
(a) Incorrect insertion hysteroscope looking upwards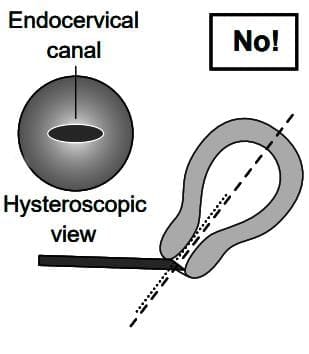
(b) Correct insertion hysteroscope looking upwards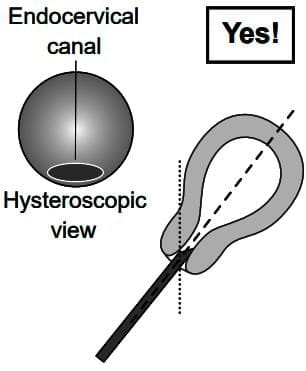
(c) Incorrect insertion hysteroscope looking downwards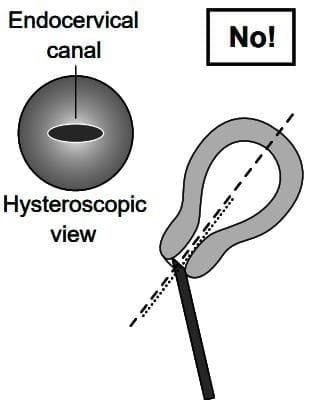
(d) Correct insertion hysteroscope looking downwards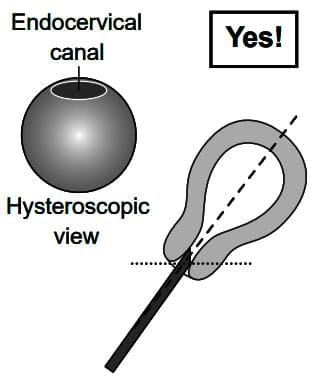
Results
- The medical literature has many studies about diagnostic hysteroscopy, which is an important method used to look inside the uterus.
- Although there are ongoing debates with those who prefer ultrasound, diagnostic hysteroscopy is still considered the best method for checking the uterine cavity.
- Even when performed in outpatient settings, hysteroscopy has a success rate of more than 90%.
- The chance of finding issues in the uterus depends on the reasons for the procedure.
- About 40% to 50% of women who experience menstrual symptoms will show positive results, mainly for conditions like fibroids and polyps.
- In cases of infertility, reports indicate that the detection rate can be as high as 60%.
 The H Pipelle being used forbiopsy after vaginoscopic or'no touch' hysteroscopy
The H Pipelle being used forbiopsy after vaginoscopic or'no touch' hysteroscopy
Complications
- Diagnostic hysteroscopy is generally a safe procedure with infrequent complications.
- The most common issue reported is discomfort or pain during cervical negotiation or uterine cavity distension.
- A vaso-vagal response to cervical dilation can occur, but it is typically alleviated by pausing the procedure and administering local anesthesia.
- Bradycardia requiring atropine is rare.
- Uterine perforation is unlikely when the hysteroscope is inserted under direct visualization, except in cases of severe cervical stenosis. In such instances, ultrasound guidance for hysteroscope insertion may be beneficial.
- Pre-procedure priming with a prostaglandin can also be advantageous.
- Infection and excessive bleeding are uncommon occurrences.
Operative Hysteroscopy
- Hysteroscopic surgery has specific and well-defined applicationsand is the preferred approach for various procedures:
- Polypectomy
- Myomectomy for intracavitary or submucous fibroids
- Adhesiolysis
- Metroplasty
- Newer second generation ablative techniques have largely replaced older methods of endometrial destruction, making these procedures easier to perform.
- Hysteroscopic sterilization using the Essure device is also now an available option.
- Although various techniques can be used for surgery, the resectoscope is the most versatile instrument, and mastering its use is a valuable skill. Thinning the endometrium in preparation for surgery can significantly assist in major procedures.
- Pretreatment options include:
- GnRH analogues
- Danazol
- Progestogen
- Combined pill
- This pretreatment is typically carried out for at least six weeks before surgery.
- Alternatively, scheduling the operation immediately after menstruation or curettage can be considered, although these methods are not as effective as proper endometrial preparation.
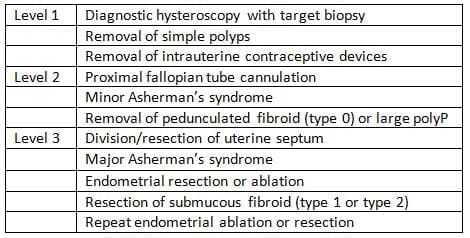
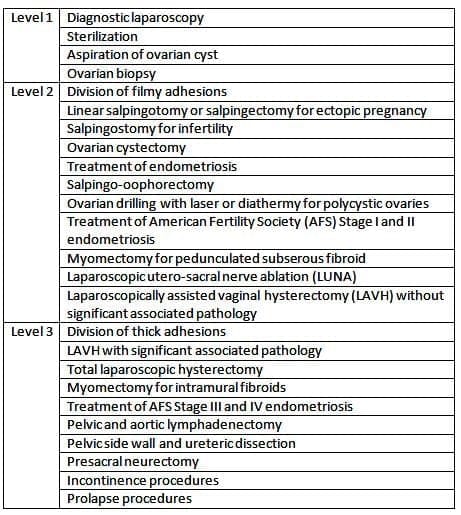
RCOG Classification of Operative Hysteroscopy Procedures
Techniques
- Minor procedures can occasionally be performed under local anaesthesia using mechanical instruments or the Versapoint system.
- However, major cases typically require general anaesthesia, although they can also be conducted with local anaesthesia and light sedation. Our approach includes:
- A premedication regimen involving diclofenac and temazepam
- Administering small doses of midazolam and either fentanyl or alfentanil in the operating theatre
- Local anaesthetic injections in the cervix, paracervix, and uterus using a needle attached to the resectoscope
- While it is not possible to cover all the instruments available to hysteroscopic surgeons or specific procedures in detail, it is crucial to understand how to use the resectoscope safely and effectively.
Using a Resectoscope
- The resectoscope is a powerful tool that requires proper handling to ensure patient safety.
- The initial step is to dilate the cervix sufficiently for easy insertion without over-dilating, as excessive dilation can lead to excessive leakage of the uterine irrigant.
- Dilating to 1 mm above the resectoscope's diameter is usually adequate.
- Once the resectoscope is in place and surgery can commence, it is important to remember three key rules:
- The electrode:
- The electrode should only be turned on while it is being inserted into the resectoscope sheath, meaning it should move towards the cervix.
- If the electrode is activated while being pushed out, it can lead to uterine perforation, which is a serious and potentially dangerous
- problem.
The only situation where this rule does not apply is during a metroplasty, where the cut needs to be made towards the uterine fundus.
- The myometrium:
- The myometrium should not be cut too deeply, especially at the cornu and in the cervix; if the ends of the small blood vessels are visible, it means the cut is too deep.
- Cutting too deeply can lead to serious risks, including uterine perforation and significant bleeding.
- Continuous monitoring of fluid balance is essential.
- Various methods for monitoring fluids have been proposed, such as:
- Checking central venous pressure
- Measuring serum sodium levels
- Assessing osmolality or using tracer substances like 1% ethanol
- Weighing the patient
- The simplest method is to maintain an inflow/outflow chart.
- Surgery should be halted if fluid absorption goes over 1.5 to 2 liters to prevent serious fluid overload and complications similar to those seen in a transurethral resection of the prostate (TURP).
- Fluid balance:
- Fluid balance needs to be monitored continuously.
- Various methods for monitoring fluids have been recommended, including:
- Checking central venous pressure.
- Measuring serum sodium levels regularly.
- Assessing osmolality.
- Using tracer substances like 1% ethanol.
- Weighing the patient.
- The easiest way to keep track of fluids is by maintaining an inflow/outflow chart.
- Surgery should be paused if the fluid absorption goes over 1.5 to 2 liters to prevent serious issues like fluid overload and a transurethral resection of the prostate (TURP) like syndrome.
Results
- When the indications are appropriate, hysteroscopic surgery can be highly effective.
- While there is limited literature on polypectomy, it is reasonable to assume that removing polyps under direct vision is superior to blind curettage.
- Numerous studies have demonstrated the success of hysteroscopic myomectomy, particularly when the uterus is not excessively enlarged and the fibroids are mostly intracavitary.
- Metroplasty should no longer be performed via laparotomy, and the same applies to the treatment of Asherman's syndrome.
- Hysteroscopic endometrial resection or ablation has been evaluated in many randomised trials and cost-benefit analyses, proving to be effective alternatives to hysterectomy, although they may not necessarily be more effective than newer second-generation techniques.
- The Mirena IUS is also a valid alternative for such patients.
Complications
- Although complications are rare with operative hysteroscopy, it is important for anyone performing this type of surgery to understand the risks and how to prevent and manage them.
- The most serious risk is uterine perforation, which can happen if the hysteroscope is activated incorrectly. This can lead to severe damage in the abdomen, causing bleeding and injury to internal organs.
- The first sign of a perforation could be a sudden loss of uterine swelling or quick absorption of fluid.
- In such cases, a laparoscopy or possibly a laparotomy is necessary to check the abdominal area. If no injury is found, surgery can continue after the perforation is stitched up.
- Perforation is more likely to occur when using a resectoscope, but using the right technique can significantly lower this risk.
- Another concern for hysteroscopic surgeons is fluid overload with low-viscosity fluids, especially those without electrolytes.
- Fluid can be absorbed during surgery through intravasation and transtubal loss, leading to serious electrolyte imbalances and effects on the heart and lungs.
- This complication can be avoided by closely monitoring the patient during surgery and stopping the procedure if needed.
- To manage fluid absorption, we also place a catheter in the bladder and give a low dose of frusemide if the absorption exceeds 1.5.
- Intraoperative bleeding can occur alongside uterine perforation but is often due to surgery being too deep in the uterine wall.
- Using electrocoagulation or laser coagulation on the bleeding vessel can help, but if bleeding continues after the procedure, using a balloon catheter for a few hours can typically stop it.
- Air embolism is a rare but serious complication that can happen if air enters the fluid used for distension, usually when changing the fluid bags.
- Infections are uncommon after hysteroscopic surgery. Despite a lack of strong evidence, I usually prescribe prophylactic antibiotics (1.2 g Augmentin intravenously) to women undergoing this procedure.
- Cervical priming with misoprostol has been suggested to lower the risk of cervical tears during dilation, although, in my experience, this complication is very rare.
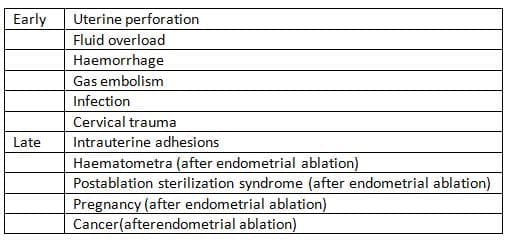
- Late complications from endometrial ablationare also quite uncommon.
- Cervical stenosis can occur if there is functional endometrial tissue, potentially leading to haematometra, and women who have undergone sterilization may experience painful swelling in their fallopian tubes due to retrograde menstruation.
- There have been reports of pregnancies occurring after this procedure, many of which involved complications.
- A few cases of endometrial cancer have been noted after endometrial ablation, though most of these patients had other risk factors.
Complications of Operative Hysteroscopy
Diagnostic Laparoscopy
- Diagnostic laparoscopy has been an essential procedure in gynaecological care since it replaced culdoscopy in the 1960s and 1970s.
- It was even used before diagnostic hysteroscopy became common.
- This procedure is usually performed in a hospital setting under general anaesthesia, although there have been some successes with microlaparoscopes.
- The main purposes of diagnostic laparoscopy are to investigate pelvic pain and subfertility.
Indications and Contraindications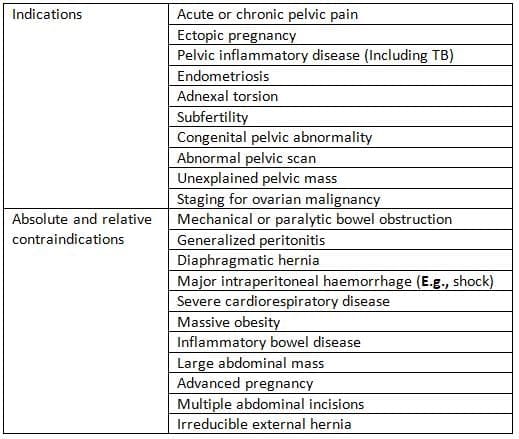
Techniques
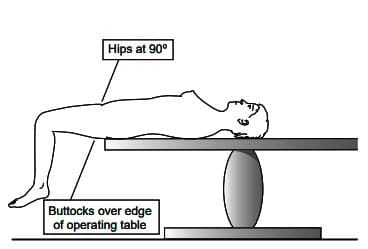
- Patient Positioning: Proper patient positioning on the operating table is crucial for the success of the procedure.
- The following guidelines should be followed:
- The buttocks should be positioned at the edge of the table to allow for full uterine anteversion.
- The legs are ideally placed in hydraulic leg supports, with the thighs at approximately 45 degrees to the horizontal.
- This positioning allows for hip extension if abdominal surgery becomes necessary.
- Pre-Procedure Preparation: Before starting the procedure, the following steps should be taken:
- Cleaning and Draping: The patient should be properly cleaned and draped to maintain a sterile environment.
- Bladder Check: If the bladder is full, it should be emptied using a catheter to prevent interference during the procedure.
- Bimanual Examination:. bimanual examination should be performed to confirm the size, position, and mobility of the uterus, as well as to identify any adnexal issues.
- Uterine Sounding and Cannula Insertion: The uterus should be sounded, and a uterine cannula inserted to facilitate manipulation and potential hydrotubation. If the uterus is retroverted, rotating the cannula 180 degrees can improve access to the Pouch of Douglas during laparoscopy.
Subumbilical Insufflation
- Although some doctors prefer open and gasless laparoscopy, most gynecologists begin laparoscopy by insufflating the abdominal cavity with CO2 using a Veress needle.
- It's important to check the spring mechanism of the Veress needle, as this is a crucial safety feature.
- Also, checking the gas flow through the needle is useful; noting the pressure in the tubing can help confirm the needle's proper placement in the abdomen later on.
 Patient positioning during laparoscopy.
Patient positioning during laparoscopy.
Technique for subumbilical insufflation and insertion of the primary port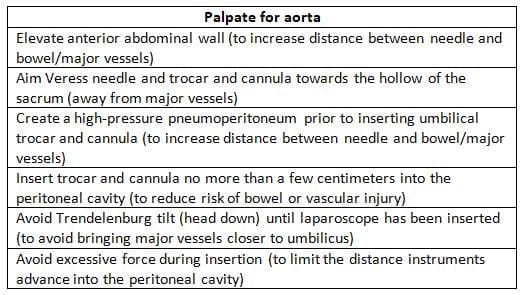
- The usual spot for inserting the Veress needle is the lower edge of the umbilicus. We prefer to make a vertical incision in the middle that is long enough to fit the umbilical trocar and cannula.
- The process of inserting the Veress needle and then the trocar and cannula for the laparoscope is briefly outlined in.
- The main goal is to access the abdominal cavity without causing unnecessary damage. It's important to remember that in many women, the aortic bifurcation is located just below the umbilicus, which should be considered when using umbilical instruments.
- After placing the Veress needle, you can check its position using Palmer's test; this involves drawing saline into the abdominal cavity with a syringe due to its negative pressure.
- Another method is to connect the gas tubing and monitor the flow and pressure of the gas; low flow with high pressure may indicate an obstruction, often due to incorrect placement, in which case the Veress should be repositioned.
- It is advisable to insufflate to a relatively high abdominal pressure (for example, 20-25 mmHg) to lessen the risk of damaging any organs during the insertion of the primary trocar and cannula.
- Once the correct expansion is achieved, the gas should be turned off, the Veress needle removed, and the trocar and cannula inserted, aiming towards the sacral hollow.
- Some gynecologists lift the lower abdominal wall manually at this stage, while others press on the upper abdomen to enhance the gas bubble in front of the incoming trocar.
 CO2 insufflation via Palmer's point.
CO2 insufflation via Palmer's point.
Insufflation via Palmer's point
- A well-known alternative to subumbilical insufflation is the use of Palmer's point.
- This point is located in the left mid-clavicular line, about 3 cm below the costal margin.
- The left upper quadrant of the abdomen is the area that is least likely to have adhesions.
- Therefore, Palmer's point is particularly helpful when there are concerns about possible lower abdominal or peri-umbilical adhesions, such as those from a midline laparotomy incision or appendicitis.
- Additionally, Palmer's point is beneficial when dealing with a large pelvic mass.
- The method for entering through Palmer's point is similar to techniques that have already been described.
Open Laparoscopy
- The safety of 'closed' versus 'open' laparoscopy is still being debated.
- Open laparoscopy, a method introduced by gynaecologist Hasson in 1970, is believed to reduce the risk of vascular and bowel injuries, although this has not been definitively proven.
- Currently, there are no large-scale randomised trials on this topic, and most gynaecologists prefer using a Veress needle for insufflation.
Insertion of Ancillary Port(s)
- After inserting the laparoscope, the patient may be tilted head down to facilitate the movement of the bowel away from the pelvis and lower abdomen.
- A greater tilt enhances the visibility of the pelvis but can make ventilation more challenging for the anaesthetist.
- Surgeons usually conduct a brief examination of the abdominal cavity before placing one or two ancillary ports in the lower abdomen.
- To minimise the risk of injury from these ports, they should be inserted under direct vision after identifying the deep and superficial epigastric vessels and the bladder.
- The 'safe triangle' concept is useful for port placement. This triangle is defined by the umbilical ligaments on the sides, with the symphysis pubis as the base and the umbilicus as the top.
- The inferior epigastric vessels, which always run outside the safe triangle, should be avoided during port placement.
- Ports can be placed either within the safe triangle or to the side of the inferior epigastric vessels.
Inspecting the Pelvis and Abdomen
- To properly inspect the pelvis, at least one probe or grasper is necessary to move the pelvic organs.
- After examining the upper abdomen, gently push any bowel in the cul-de-sac upwards.
- The best way to examine the adnexa and pelvic side wall is by grasping, lifting, and rotating the ovary towards the ipsilateral round ligament, which also helps to visualise the path of the ureter.
- Don't forget to check the uterovesical fold, as it might be the only site of endometriosis.
- Tubal patency can be evaluated using hydrotubation with a dilute methylene blue solution.
Ending the Procedure
- Remove the ancillary ports under direct vision.
- Deflate the abdomen using the port for the optic.
- Keep the laparoscope inside the cannula while withdrawing it to check for bleeding or any bowel or omentum being caught at the port site.
- Close the fascia in lateral ports larger than 10 mm properly to prevent herniation.
Results
- The success of finding problems during laparoscopy largely relies on the reason for doing the procedure.
- Some issues can be easily identified through preoperative tests, like an ultrasound, where laparoscopy is mainly used to verify or explain the diagnosis.
- Although diagnostic laparoscopy is no longer suggested as a routine test for all couples facing infertility, it can still uncover unexpected issues.
- For example, the detection rate of conditions like endometriosis and pelvic adhesions is approximately 20%.
- In cases of chronic pelvic pain, a specific study found that every one of the 141 patients who underwent laparoscopy had positive results.
Complications
- Diagnostic laparoscopy is considered safe, with complication rates ranging from 2 to 4 per 1000 procedures.
- Most complications occur during the initial setup when the abdomen is being prepared, such as injuries to the inferior epigastric vessels, major retroperitoneal vessels, or the bowel.
- Bleeding from the inferior epigastrics can usually be prevented with good technique, but if it occurs, various instruments and methods are available to control it.
- Injury to retroperitoneal vessels generally requires immediate laparotomy, while bowel injury can often be managed laparoscopically if the perforation is small and there is minimal faecal contamination.
Operative Laparoscopy
- The focus of the current discussion is not on what can be done laparoscopically, but rather on what cannot be done.
- Most procedures that are typically performed through laparotomy can also be carried out laparoscopically, as long as there isn't a large pelvic mass or extensive cancer present.
- However, this does not mean that laparoscopy is the best option for every case.
- There is significant debate regarding more complex procedures, and only a few have been subjected to prospective randomized comparisons, such as ectopic pregnancy, colposuspension, endometriosis, and hysterectomy.
- Therefore, the choice of surgical approach often depends on the specific skills of the gynecologist, any contraindications, and the associated risks of complications.
Techniques
- Due to space constraints, it is not possible to describe each procedure in detail.
- However, certain points and techniques are generally applicable to operative laparoscopy.
RCOG classification of laparoscopic procedures
 Where to Place the Ancillary Ports
Where to Place the Ancillary Ports
- Operative laparoscopy typically involves the use of multiple ports, with 2 to 3 ancillary ports being standard.
- It is crucial to place these ports away from the inferior epigastric vessels and high enough to allow instruments to be used on both sides of the pelvis.
- If frequent suturing is required, a 10-mm port should be used to facilitate the insertion of curved needles without the need to remove the ports.
- Alternatively, a larger cannula can accommodate bigger instruments, such as SEMM claw forceps.
Tissue Dissection and Hydrodissection
- The principles of dissection and adhesiolysis in operative laparoscopy are similar to those in laparotomy, primarily involving traction and countertraction.
- Scissors can be utilized for dissection, and when using monopolar electrosurgery or CO2 laser, extra caution is necessary to prevent thermal damage to adjacent tissues.
- High pressure irrigation can sometimes assist in dissection and protect underlying structures from heat injury.
Safe Use of Electrosurgery
- Electrosurgery is a common technique in laparoscopy for both haemostasis and cutting.
- However, due to the risk of electrosurgical injury, it is essential to take all necessary precautions.
- The instrument should only be activated when visible in the laparoscope, and the electrodes must be fully retracted into the cannula afterwards to prevent accidental injury.
- Electrosurgery should be performed near bowel or other critical structures in short bursts, if at all.
- Surgeons must be mindful of the risks associated with insulation failure, which can lead to severe complications, and remember that electrodes remain hot for a few seconds after activation.
Laparoscopic Suturing
- The ability to suture both inside and outside the body is a valuable skill in laparoscopic surgery, potentially distinguishing it from laparotomy.
- Pretied loop sutures are the easiest to work with and are suitable for procedures like salpingectomy.
- Untied ties can be used to secure adhesions or vascular pedicles and are fastened with slip knots and a knot pusher.
- Needle sutures are employed to repair incisions and can be tied inside or outside the body for delicate tissues.
Results
- Laparoscopic surgery generally leads to less postoperative discomfort and shorter hospital stays, with patients typically returning to normal activities more quickly than after laparotomy.
- However, more complex procedures often take longer and are less predictable in duration.
- Cost comparisons yield varying results, as longer operating times and the use of disposable instruments may offset the benefits of shorter hospitalisation.
Complications
- Laparoscopic surgery is typically seen as safer than traditional surgery. However, while the overall risk of complications is lower, it is not guaranteed. Serious problems can still occur, and many injuries may go unnoticed during the procedure.
- The complication rate reported in major national surveys ranges between 7-12.6 per 1000 procedures, with more complex surgeries posing a higher risk.
Complications of Laparoscopic Surgery
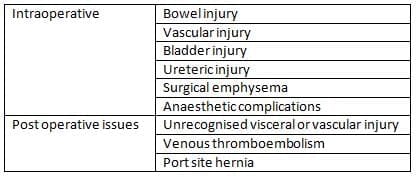
Risk of Specific Injuries:
- Intestinal injury: Estimated at 1.6-2.4 per 1000 procedures.
- Major vascular injuries: Risk of 0.3 per 1000 procedures.
- Urinary tract damage: Occurs in 2-8.5 per 1000 cases.
- Laparoscopic Hysterectomy: This procedure particularly increases the risk of ureter injury.
Timing of Complications:
- About 1 in 3 complications occur during the setup phase.
- Roughly 1 in 4 complications are unrecognised during the operation, especially bowel and ureter injuries, which are unrecognised in more than half of cases.
- Conversion to Open Surgery: On average, 2% of patients require conversion to open surgery (laparotomy).
- Mortality Rates: Gynaecological laparoscopy has a mortality rate of 4.4 per 100,000 procedures, compared to 150 per 100,000 for benign conditions.
Informed Consent for Endoscopy
- There is a common misunderstanding among patients that keyhole surgery turns a major surgery into a minor one.
- Many believe that this type of surgery not only provides better cosmetic results and a faster recovery but also reduces risks.
- In reality, the only difference is the size of the incision.
- Because of this misunderstanding, when complications arise, patients often think there has been negligence.
- Consequently, endoscopic surgery has become a significant area of medical lawsuits in gynecology.
- The Department of Health and the General Medical Council have provided guidelines on informed consent for surgery.
- There is also valuable information available online regarding this topic.
- While having clear reasons for surgery and using good surgical methods are essential for effective patient care, it is also crucial to give patients enough information to help them decide whether to proceed with a specific procedure.
- Patients should be informed about:
- What the procedure involves and why it is necessary.
- The relative risks of minimally invasive surgery compared to traditional surgery.
- Specifically, patients need to understand that:
- Any endoscopic operation might need to be changed to a laparotomy.
- Injuries to the bowel, bladder, and ureters are recognized risks with laparoscopy.
- Risks such as uterine perforation and fluid overload can occur with hysteroscopy.
Training in Endoscopic Surgery
- Surgical training has been greatly changed by MAS.
- Endoscopic surgery is quite different from traditional surgery.
- It likely requires more time to learn the skills needed for operating without direct vision and proper handling of tissue.
- Recognizing the significance of hysteroscopic and laparoscopic surgery in modern gynecological care, the Royal College of Obstetricians and Gynaecologists has incorporated basic endoscopic surgery (Level 1 hysteroscopy and laparoscopy) into the core curriculum for trainees.
- The College has appointed preceptors to guide this training.
- They are also introducing Special Skills Modules for advanced hysteroscopic and laparoscopic surgery, aimed at helping those who want to enhance their skills.
- This marks the first instance where surgical skill in a specific area is being rigorously tested.
- These modules could serve as a model for evaluating skills in other surgical areas in the future.
FAQs on Chapter Notes: Hysteroscopy and laparoscopy
| 1. What is 'no touch' hysteroscopy, and how does it differ from conventional hysteroscopy? |  |
| 2. What are the common complications associated with laparoscopy and hysteroscopy? | |
| 3. What is subumbilical insufflation, and why is it important in laparoscopic procedures? | |
| 4. What is the purpose of using Palmer's point for insufflation during laparoscopic surgery? | |
| 5. How is the pelvic and abdominal inspection conducted during laparoscopy, and what are its objectives? | |



