Chapter Notes: Neonatal care for obstetricians

The transition to the extrauterine life
Lungs
- When a baby is born, the lungs expand, which is a big challenge for the newborn.
- In the womb, the lungs make fluid that goes into the alveolar space, so the lungs are full of fluid.
- During normal birth at full term, the making of this lung fluid stops.
- High levels of thyroid hormone, adrenaline, and corticosteroids in the baby's blood cause the fluid flow to reverse forever, preparing the air spaces for breathing air.
- Most of the lung fluid is taken into the pulmonary lymph vessels and small blood vessels.
- A small amount of fluid is pushed out of the lungs because of high pressure from the vagina during the second stage of labor.
- In response to a number of stimuli following birth which include changes in environmental temperature, physical touch, sound, and light.
- A healthy baby born at full term usually takes the first breath within 60 seconds.
- The first breaths make high pressure in the lungs to overcome several factors, such as the surface tension at the air-liquid interface in collapsed small air sacs, the high resistance to flow and inertia of fluid in the airways, and the elastic recoil and compliance of the lungs and chest wall.
- Because of this, the initial breathing efforts result in both larger breaths in that create high negative pressure of 20 cm of water inside the lungs and forced breaths out that make positive pressure ranging from 20 to 100 cm of water.
- Replacement of lung liquid with air is mostly done within a few minutes after birth.
- This process may be delayed if the birth happens before labor starts because the drive to breathe is weakened by things like being born too early, lack of surfactant, low oxygen during birth, and general anesthesia.
- Once the lungs are expanded, how easy it is to stretch them gets much better, and the pressure needed for normal breathing in and out is only about 5 cm of water.
- If the baby fails to take back the lung fluid, it can cause short-term fast breathing in a full-term baby.
- Lungs that are expanded must be kept from collapsing again, and this relies on a surfactant system.
Surfactant
- Surfactant is a complex mix made mostly of phospholipids, with smaller amounts of neutral lipids and proteins.
- It is made by type 2 alveolar cells. These cells can be identified from about 24 weeks of pregnancy onward.
- However, surfactant production is limited until later in pregnancy.
- It is the phospholipids that notably dipalmitoyl phosphatidylcholine, or DPPC, which form a single layer at the alveolar-air tissue interface.
- They highly lower the surface tension, producing surface tension that changes with the size of the air sac.
- This stops alveolar collapse.
- The four surfactant-associated proteins SP-A, SP-B, SP-C, and SP-D each have essential roles.
- SP-B and SP-C aid spreading, adsorption and recycling of the phospholipids.
- SP-A has a dual role in improving surfactant function and with SP-D is part of the innate host defense mechanism against infection.
- Surfactant production and release increases during the later part of pregnancy under control of hormones such as corticosteroids and thyroid hormone.
- Maturation of the surfactant system can be stimulated by numerous agents including maternal glucocorticoids.
- Babies born preterm may fail to clear lung liquid or produce surfactant so that pulmonary compliance remains low and the high negative intrathoracic pressures required for lung inflation during the first breath persist.
- These infants develop respiratory distress and may require ventilation and surfactant replacement.
The heart and circulation
- In the unborn baby, oxygenated blood from the placenta is preferred to stream through the ductus venosus to the right atrium and across the foramen ovale into the left atrium.
- Here it mixes with the small quantity of pulmonary venous blood, then passes to the left ventricle from where it is pumped to the aortic root and to the cerebral and coronary circulations.
- A small proportion of inferior vena cava blood enters the right atrium and mixes with the poorly oxygenated blood returning through the superior vena cava, passing to the right ventricle and pulmonary artery.
- In the fetus, pulmonary vascular resistance is extremely high and only a small amount of blood passes through the lungs.
- Most of the blood passes through the ductus arteriosus into the aorta.
Haemoglobin
- In the full-term baby, the haemoglobin level is high, between 16 and 18 grams per deciliter.
- Of this, 80 percent is fetal haemoglobin, or HbF.
- HbF has a lower liking for 2,3-diphosphoglycerate, moving the oxygen dissociation curve to the left, leading to maximum oxygen transfer at lower partial pressure of oxygen.
- The proportion of HbF falls slowly during the first month after birth and by six months only 5 percent of haemoglobin is HbF.
- The relatively high total haemoglobin level also falls after birth.
- Haemoglobin is removed through the making of bilirubin which is taken away by the liver.
- Liver immaturity often leads to jaundice in the normal newborn baby.
- Too much breaking down of red blood cells or liver damage can lead to levels of unconjugated bilirubin high enough to cause brain damage.
Feeding and nutrition
- Human breast milk is the best food source for both full-term and early-born babies.
- It is linked with a big drop in both sickness and death rates.
- Every effort should be made to encourage a mother to feed her baby with breast milk.
- There are few real reasons not to breastfeed, though some rare inborn metabolism errors may stop it.
- In the United Kingdom, to encourage mothers who are HIV-positive to breastfeed is not the practice.
- However, this is not the case in developing countries where breastfeeding is generally safe for the baby if the mother needs medication.
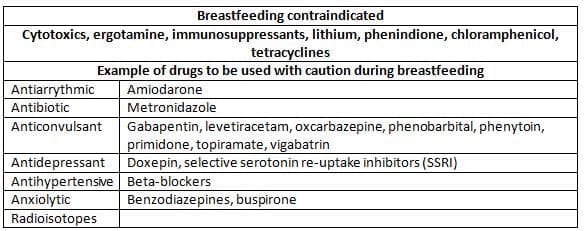
- Rarely breastfeeding is completely not allowed.
- The mother should be told if the drug prescribed is safe.
- Information can be found in the British National Formulary.
- If a potential problem is found, the advice of the local children's drug expert or local drug information center should be asked for.
- Often other drugs can be given and breastfeeding can go on.
- Human breast milk is a complex living fluid that changes in makeup over time.
- Colostrum has a higher level of protein and minerals than mature milk and gives a large number of active substances and cells.
- Term colostrum has about 3 million cells per milliliter, of which about 50 percent are polymorphonuclear leukocytes, 40 percent macrophages, 5 percent lymphocytes, and the rest epithelial cells.
- Colostrum also has antibodies, humoral factors, growth factors, and interleukins.
Drugs and Breastfeeding
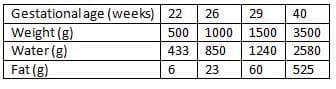
Body composition, fluids and electrolyte metabolism
- Table the average body makeup of appropriately grown babies at different gestational ages.
- Full-term babies have about 70 percent body water at term.
- Extracellular fluid decreases from 65 percent of body weight at 26 weeks to 40 percent at term.
- Administration of intravenous fluids to a mother or Caesarean section increases the baby's body water after birth.
- Following birth, an abrupt contraction of the extracellular compartment occurs, term infants lose about 5 percent and preterm babies 10-15 percent of body weight by diuresis during the first 5 days.
- This is an important adjustment to extract life.
- If it is interrupted by stress which causes secretion of anti-diuretic hormone, infants with respiratory problems show little weight loss until the lung condition improves.
- However, babies who are sick from many causes may also show too much weight loss and loss of more than 10 percent in a term baby is cause for concern.
- The glomerular filtration rate is low in newborn babies and only reaches mature levels by the end of the first year.
- Thus babies initially need little water, and 40-60 ml per kg per 24 h is adequate. Infants have a concomitant obligatory sodium loss and do not need dietary sodium until weight loss is complete.
- In a sick or preterm infant, fluid and electrolyte administration must be carried out with great care as well as frequent measuring of weight and blood electrolyte levels.
Infantile Body Compositions
Temperature control
- The placenta acts as a heat exchanger that moves heat made by metabolism from the fetus to the mother.
- After birth, the newborn baby works as a creature that keeps its own heat, keeping deep body temperature at 37 degrees Celsius.
- Heat control puts a big demand on the baby's metabolism and body functions because a large surface area to volume ratio and wet skin make the newborn baby easy to lose too much heat.
- Newborn babies have a special organ for making heat called brown adipose tissue, which allows heat making without shivering.
- Catecholamines are released when cold, starting oxidative phosphorylation in these cells, where uncoupling energy metabolism from ATP making lets chemical energy be turned into heat.
- Non-shivering heat making is weakened in the first few hours of life in sick babies and after the mother had sedative drugs.
- Despite this, the newborn baby has limited ability to keep core temperature in environmental temperatures below 32 degrees Celsius.
- Non-shivering heat making increases oxygen use and keeps core temperature.
- However, at environmental temperatures below 24 degrees Celsius, heat production is not enough and the body temperature will fall.
- It is important to make sure the environment temperature in delivery rooms and theater is 20 degrees Celsius for a full-term baby and at least 25 degrees Celsius if an early birth is expected to stop initial low temperature.
- Early-born babies are at special risk of low temperature because of lack of brown fat, small energy stores, high evaporative heat loss through immature skin, large surface area to volume ratio, hormone sickness extreme demands on the metabolic systems.
- These physiologic abilities and an unstable core temperature often come with severe illness.
- While a full-term baby with heat loss can be cared for by dressing and wrapping in warm blankets, sick or early-born babies need incubators or radiant heaters to keep a normal core temperature.
Resuscitation of the newborn
Assessment and simple resuscitation at birth
- Most babies born at full term and without special risk signs during pregnancy do not need resuscitation.
- Although all those who do can be resuscitated by simple methods using bag and mask ventilation.
- A small number of full-term babies may need more complex resuscitation involving putting a tube in the windpipe.
- Thus, while having equipment for resuscitation ready, the first task of the person attending is to decide if resuscitation is needed or not.
- Assignment of American Pediatric Gross Assessment Record or APGAR score is described in The table below shows.
Clinical Evaluation of the New born Infant (Apgar Scoring Method)
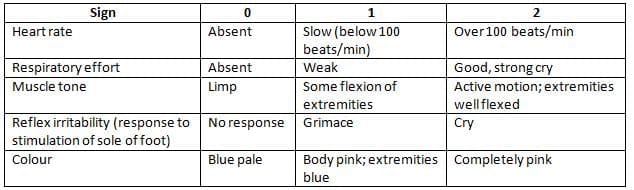
The Apgar score is got by giving the value of 0, 1 or 2 to each of five signs and adding the result.
- These scores are usually determined at 1 and 5 minutes and describe heart, breathing, and brain depression.
- There are many reasons for depression at birth, and low Apgar scores are neither proof of birth asphyxia, nor, except in extreme cases, a guide to brain prognosis.
- However, a low Apgar score shows a problem that needs explanation and management.
- It is helpful to note a time clock at the moment of delivery and some attendants suck the nasal passages right after delivery to remove fluid and debris from the throat and exclude blocked nasal passages, although many think this to be too much for low-risk births.
- In a baby who breathes right away on delivery, it takes minutes for the brain oxygen levels to reach normal outside the womb levels and there is no reason to think that a short period of no breathing at birth causes big injury.
- At least three quarters of normal full-term babies breathe within a minute of delivery and most of the rest have breathed before 3 minutes.
- The low-risk newborn can thus be safely given right away to the mother, while drying with a warm towel, which should then be thrown away, and the baby then covered in dry warm towels to allow skin-to-skin contact with the mother.
- The baby can then be watched, and failure to breathe by 30 seconds should convince the attendant that resuscitation might be needed.
- At first drying, or blowing cold air or oxygen over the face may start breathing.
- If this fails then resuscitation is right.
- In many units early-born babies are placed directly in plastic bag without drying.
- It helps control the whole baby except the head.
- The low birth weight baby will also require more care.
- If the baby is not breathing, give five inflation breaths, lasting about 2-3 seconds each.
- Give enough pressure to cause the chest to rise.
- Gas source: both should have a valve which releases pressure at 30 cm of water.
- After the airway has been adequately cleared by suction, the mask is positioned over the nose and mouth with the baby lying prone and the head in the neutral position.
- The nose and mouth should be completely covered by the mask.
- The bag is squeezed for 1 second to deliver several long inspiratory breaths, which should lead to regular ventilation at a rate of 30-40 breaths per minute.
- In many cases ventilating with air is effective as using oxygen. This technique requires practice and obstetricians and midwives should maintain their skills, if necessary, using an appropriate resuscitation dummy.
- The best guide to successful resuscitation is the baby's heartbeat.
- This can be determined in most cases by feeling the umbilical cord or the femoral pulsation, or by can be heard through the chest wall.
- Through a stethoscope over the chest. A heart rate above 120 is usually adequate.
- A heart rate below 100 needs more effective therapy.
- The heart rate provides a more immediate and accurate guide to the baby's state than respiratory effort or skin color and, especially for the occasional or inexperienced resuscitator, is the best short-term measure of success or failure.
Advanced life support
- If mask ventilation fails to produce an adequate heart rate on 2-3 minutes, a normal heart rate can be obtained by putting a tube in the windpipe.
- This may need special training. If thinking of the airway and repeated re-positioning does not work, this may indicate a blocked airway.
- If thinking of the airway.
- Be helpful. These scores are conventionally determined at 1 and 5 min and describe cardiorespiratory and neurological depression.
- There are many causes of depression at birth, and low Apgar scores are neither evidence of birth asphyxia, nor, except in extreme circumstances, a guide to neurological prognosis.
- Nevertheless, a low Apgar score signifies a problem that needs explanation and management.
- It is helpful to commence a time clock at the moment of delivery and some attendants aspire the nasal passages immediately after delivery to remove fluid and debris from the pharynx and exclude choanal atresia, although many believe this to be excessive for low-risk births.
- In an infant who breathes immediately on delivery, it takes minutes for the cerebral oxygenation concentration to reach normal extrauterine levels and there is no reason to believe that a short period of apnoea at birth causes significant injury.
- At least three quarters of normal term infants breathe within a minute of delivery and most of the rest have breathed before 3 min. The low-risk new- born can thus be safely given immediately to the mother, while drying with a warm towel, which should then be discarded, and the baby then covered in dry warm tow els to allow skin to skin contact with the mother.
- The infant can then be observed, and failure to breath by 30 s should be persuaded the attendant that resuscitation might be needed. Initially drying, or blowing cold air or oxy- gen over the face may stimulate respiration. If this fails then resuscitation is appropriate. In many units preterm babies are placed directly in plastic bag without drying. It helps control the whole baby except the head. The low birth weight infant will also require slow rotational movement of the head will also elect cells.
- Eye opening to the first 24 h after birth is pathological. It is usually unconjugated and the commonest causes are haemolytic anaemia or infection.
Admission to neonatal units
- Unnecessary admission of infants to neonatal units can strain resources and put the infant at risk of nosocomial disease, as well as interrupting bonding and frightening parents.
- Adequate transitional care facilities are essential to avoid misuse of neonatal care
Examination of the newborn infant
- A preliminary examination is made in the delivery room to establish that the baby does not have a major abnormality such as spina bifida and the full examination at a later time.
- In this way bonding and the initiation of breastfeeding are not interrupted.
- The examination should be carried out on every baby in the presence of the mother before discharge from hos- pital, ideally it should take place 24-48 h after birth; however, if discharge before this, the examination should still be undertaken. It should be possible to examine the baby again during the first week if any trained practitioner can carry out the newborn examination.
- A history should be taken including maternal obstetric and family history to identify problems in the baby that will require further management or follow up.
- During examination one relies heavily on observational skills. Note abnormalities of posture and asymmetry of facial or limb movements. Evidence of jaundice, poly- cythaemia, anaemia or rashes is noted and choanal atresia excluded.
- A systematic search for congenital abnormalities can be rapidly performed by examining along the midline and then passing the limbs. Starting with the head, the facial features should be noted and thought given to dysmor- phic syndromes. The palate needs to be examined visually to exclude a cleft palate or bifid uvula which signifies a sub-mucous cleft. The eyes must be examined by ophthal- moscopy to exclude cataracts: in a normal eye the red reflex is immediately obvious. Eye movements may not be fully coordinated in the first week of life and momentary strabismus is common.
- Examination should be made of (1) the back of the neck and the spine for skin lesions suggesting spinal dys- raphism, (2) the anus, (3) the genitalia, (4) the femoral pulses, (5) hips, (6) the abdomen, and (7) the chest for examination of the cardiovascular and respiratory system.
- The femoral pulses are examined. Absent or delayed pulses, and palmar creases are examined, urgent need to be checked for coarctation of the aorta. The heart should be auscultated for murmurs: many innocent murmurs are heard, but those associated with other con- genital defects, where major heart disease can occur.
Circumference
- This forms the basis of developmental surveillance in following years. It should also be ascer- tained that the infant has passed meconium and urine within 24 h of birth.
- The examination should be prepared to answer maternal questions and discuss the merits of BCG and hepatitis B vaccination, and routine screening tests if appropriate.
- Universal newborn hearing screening has recently been introduced in the United Kingdom. Universal biochem- ical screening for phenylketonuria and hypothyroidism during the newborn period is well established. In addi- tion, galactosaemia, cystic fibrosis, haemoglobinopathies and various aminoacidopathies are screened for in some parts of the United Kingdom.
Disorders in the newborn period
Preterm birth
- Infants born significantly before term usually require neonatal care until near the expected date of deliv- ery. Following the introduction of surfactant coupled with good specialist care of antenatal corticosteroids in the mid-1990s, survival rates for those well fell significantly although the risk of long-term handicap remained high. Rates in the twenty-first century remain simi- lar to those shown. Mortality in extremely preterm babies can be significantly reduced if hypothermia is prevented at birth; this is only possible if the delivery room is main- tained at an appropriate temperature. Most survivors do not suffer long-term disability, but in infants of less than 28 weeks gestation some 20% suffer neurodevelopmental impairment.
- The stress on parents and family of having a baby who undergoes intensive care can be immense. They have to suffer prolonged uncertainty about the infant's survival as well as a loss of control over their baby's and their own
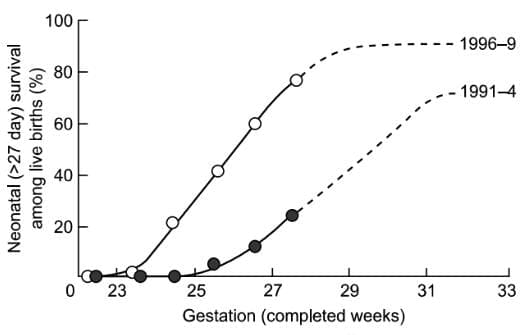 Neonatal survival among registered live births. Redrawn from Tin et al. BMJ 314, 107-10.
Neonatal survival among registered live births. Redrawn from Tin et al. BMJ 314, 107-10.
Respiratory disorders
- Abnormal breathing is a common presentation of many illnesses in the newborn period.
- Intermittent or periodic breathing is common and not usually significant.
- However, a breathing rate persistently above 60 breaths per minute needs further investigation, as do periods of no breathing lasting more than a few seconds, especially if associated with cyanosis and slow heart rate.
- Tachypnoea with recession and nasal flaring is fre- quently the presentation of respiratory or cardiac disor- ders, while no breathing may be the presentation of a great many disorders such as sepsis, meningitis, gastrointes- tinal obstruction or heart disease.
Surfactant deficiency
- The respiratory distress syndrome caused by inadequate surfactant production is mainly a disease of the preterm infant.
- However, it can occur in term infants, particu- larly those of diabetic mothers or after caesarean section without labour.
- Affected infants may require mechanical ventilation and intensive care. The classical clinical presentation is an infant with tachypnoea, subcostal and intercostal reces- sions over the first 48 h after birth, and a chest X-ray showing a ground glass appearance with air bronchograms. It can be associated with pneumothorax, bronchopulmonary dys- plasia (BPD) and intracranial haemorrhage although in more mature infants it normally resolves without seque- lae. The combined use of antenatal corticosteroids and surfactant modify the illness, improving survival and reducing the rates of complication such as pneumotho- rax and intracerebral haemorrhage but have little effect on reducing the incidence of BPD.
Congenital pneumonia
- Congenital pneumonia is a relatively common problem associated with a variety of microorganisms.
- The infant presents with respiratory distress and a chest X-ray shows patchy inconsistent shadowing.
- Treatment is with antibi- otics and intensive care as required.
Meconium aspiration
- Inhalation of meconium before or during delivery can be an extremely severe problem if pulmonary hypertension
Transient tachypnoea of the newborn
- Transient tachypnoea of the newborn is due to delayed reabsorption of lung liquid and leads to a moderate degree of tachypnoea and tachypnoea. In the preterm infant this can lead to marked respiratory distress, but in a term baby needing high inspired oxygen concentrations other causes of respiratory distress should be excluded.
Bronchopulmonary dysplasia
- This is a chronic condition affecting up to 50% of infants born at 26 weeks. Prematurity/delivery, pre- and post- natal inflammation and infection, ventilation, oxygen and poor nutrition are among the many factors contributing to the development and persistence of BPD.
- The underlying problem is an arrest of alveolar and peripheral vascular development. The severity is variable ranging from the need for supplemental oxygen for several weeks to pro- longed respiratory support with a ventilator or continuous positive airways pressure and death.
- A small proportion of babies are discharged home on supplemental oxygen; most outgrow the need by 12 months of age. All babies born prematurely have an increased risk of respiratory ill- ness within the first few years of life.
- This is increased in the group with BPD and respiratory problems may persist into adult life.
Cardiac disorders
- Some form of congenital heart disease affects between 7 and 9 per 1000 live births of whom approximately one quarter will present in the newborn period. Fetal anomaly ultrasound can detect many lesions, antenatally, however, some are more difficult to diagnose
Cyanosis due to reduced pulmonary
- Cyanosis due to reduced pulmonary blood flow
- The commonest causes are transposition of the great arteries (TGA), right to left shunts such as Tetralogy of Fallot and pulmonary or tricuspid atresia.
- Administration of 100% oxygen fails to increase arterial saturation and a chest X-ray may show oligemia.
- Tachypnoea may occur; however, respiratory distress is often not a prominent feature of the presentation whereas cyanosis may be profound.
- A measurement of blood gases is mandatory for those babies presenting with central cyanosis in order to rule out the possibility of respiratory or cardiac disease or to a specialist paediatric cardiac centre.
Cardiorespiratory distress due to increased
- Left to right shunting though septal defects with a consequent increase in pulmonary blood flow decreases the compliance of the lung, leading to chest recession and tachypnoea.
- The homoeostatic response to this shunt is fluid retention, leading to congestive cardiac failure with a large liver and oedema.
- Infants with large left to right shunts are not particularly hypoxic except when cardiac failure is severe.
- The commonest cause of large left to right shunts is the patent ductus arteriosus.
Cyanosis and cardiiorespiratory distress
- Infants in whom mixing between systemic and pulmonary circulations is impaired can present with breathlessness and cyanosis.
- Complex conditions such as transposition of the great arteries may lead to this presentation.
Shock syndrome due to low cardiac output
- The clinical picture of shock is a desperately ill infant with generalized pallor, cyanosis, cool peripheries and weak or absent pulses.
- Breathing is laboured or gasping, and the heart rate is elevated.
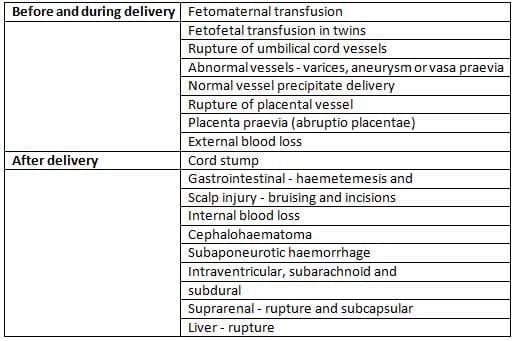
- The shock is usually due to major circulatory problems such as hypovolaemia, sepsis, significant blood loss or major interruption to the circulation such as coarctation of the aorta or complex cardiac defects.
- Causes of significant blood loss in the newborn baby are given in Table 11.4.
The asymptomatic murmur
- Murmurs are common in newborn infants and are fre- quently innocent. A low amplitude systolic ejection mur- mur is audible in some 60% of normal newborn infants.
- It is normally best heard over the pulmonary area and may be due to ductal flow or a tricuspid regurgitation or a pulmonary artery branch flow murmur which dis- appears before 6 months of age. Innocent murmurs are systolic, short, localized and may change. Infants may develop murmurs when unwell, because of increased car- diac output accompanying the ductus arteriosus. Other causes of asymptomatic murmurs in the newborn period include septal defects, aortic or pulmonary stenosis and Tetralogy of Fallot. A thorough search for other signs of cardiac disease should be made and an expert opinion arranged where appropriate. It is important to remem- ber that the mention of a heart murmur can strike panic into even the calmest of parents and the situation needs to be handled with great tact. Rapid definitive diagno- sis by echocardiography is the mainstay of successful management.
Neurological disorders
Neonatal encephalopathy
- Neonatal encephalopathy can be caused by hypoxia ischaemia due to birth asphyxia but also by other condi- tions including metabolic disorders and infections.
- These conditions should be excluded before a confident diag- nosis of hypoxic ischaemic encephalopathy due to birth asphyxia can be accepted.
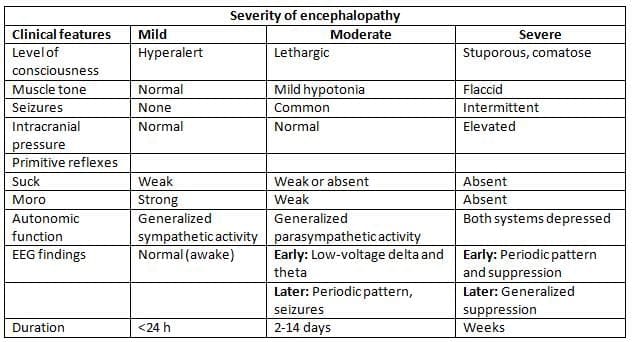
Classification of severity of Hypoxic ischaemic Encephalopathy in the term Newborn
Hypoxia-ischaemia
- Hypoxia-ischaemia followed by resuscitation may lead to apparent recovery followed by inexorable deteriora- tion beginning 6-8 h later and ending in severe cerebral injury.
- Consequently, it is frequently difficult to determine the prognosis soon after birth on clinical grounds alone.
- However, if asphyxia is severe or happened some time before delivery the infant will not develop spontaneous breathing; therefore, if despite advance life support there is no sign of spontaneous breathing 20 min after birth the outcome is extremely poor.
- Hypoxic ischaemic encephalopathy is graded clinically using clinical signs.
- A frequently used grading system - that of Sarnat and Sarnat - is given in Table 11.5.
- Infants with grade 1 encephalopathy have a very good prognosis whereas infants with grade 3 are all either dead or severely neurologically impaired.
- Grade 2 is a large group with variable outcome.
- Further investigation is required, preferably by paediatricians specialized in neonatal neurology and with access to sophisticated equipment such as electrophysiology, magnetic resonance spectroscopy. Diagnosis and an accurate guide to prognosis can then be obtained.
Cerebral palsy
- Cerebral palsy is a non-progressive brain syndrome which may not be apparent until after the first year of life and which can not be confidently diagnosed at birth.
- Population based studies have shown that about 20% of all cases of cerebral palsy are due to birth asphyxia in the term infant, approximately one third are associated with preterm birth, and the remainder have no obvious fetal or perinatal antecedent.
Convulsions
- Convulsions occurring just after delivery in term infants may be due to hypoxic ischaemic encephalopathy, metabolic disorders, infections, hypoglycaemia, hypocal- caemia, hypomagnesaemia or pyridoxine deficiency.
- Many otherwise idiopathic fits are caused by focal brain infarction, which have a much better prognosis than generalized hypoxic ischaemic injury but are difficult to diagnose without magnetic resonance imaging.
Brain injury in preterm infants
- Preterm infants are at high risk of cerebral injury and approximately 10% of infants born preterm develop significant neurodevelopmental impairment and another 10% have minor neurological lesions.
- First, intracerebral haemorrhage may affect only the ger- minal layers or ventricles in which case the prognosis is good; however, haemorrhage into the brain parenchyma is caused by haemorrhagic infarction and this is associated with neurodevelopmental impairment.
- Second, periventricular leucomalacia is there is a gen- eral loss of periventricular white matter with cavitation.
- Whereas haemorrhagic parenchymal infarction can be usually seen by cerebral ultrasonography, periventricu- lar leucomalacia is difficult to see and is probably under diagnosed. Both these conditions seem to be becoming less common than a mild ventricular loss of cerebral matter; this may present as dilation of the lateral ventricles on cerebral
- Ultrasonography but is often only apparent with mag- netic resonance imaging. The aetiology of this condition is poorly understood, the extremely preterm infant seems to be most at risk. The usefulness of cerebral ultrasonogra- phy alone to predict neurological prognosis in extremely preterm infants is therefore limited.
- The more mature preterm infants with normal ultra- sound scans at discharge from intensive care impairment have a greater than 50% chance of long-term impairment.
Brachial plexus injury
- Brachial plexus injury occurs in 0.4-2.5 per 1000 live births. The commonest type, Erb's palsy, involves C5 and 6 nerve roots. The incidence has not declined over the past few decades, however, the prognosis for recovery, which occurs in more than 80% of cases, has improved with better management including surgery to repair plex- us in severe cases. The arm is typically limp with the arm to the side, internally rotated and pronated, and the fingers flexed.
- This may also be present. Careful neurological examination is needed to determine the level of the lesion as this affects the prognosis for recovery of function.
Effects of maternal drug ingestion
- Infants of mothers who take drugs such as opiates, cocaine, amphetamines, barbiturates, benzodiazepines and some other medical drugs may develop withdrawal syndrome with irritability, poor feeding, apnoea and fits.
- The babies also exhibit withdrawal. Wherever possible the mother should be kept together; in many cases breast- feeding is not contraindicated. If a history of maternal drug abuse was known antenatally a plan of manage- ment can be agreed before birth and a referral to the social work team may be appropriate.
- Management of a baby at risk of drug withdrawal involves careful observation and skilled nursing. If withdrawal is severe treatment with opiates may be required. Naloxone should never be given to infants at risk of opiate withdrawal as it can provoke convulsions. Many labour wards no longer stock nalox- one for fear it will be given inadvertently to an infant of a substance-abusing mother.
Jaundice
- Jaundice beginning in the first 24 h after birth is pathological.
- It is usually unconjugated and the commonest causes are haemolytic anaemia or infection.
- Jaundice beginning on days 2-5 is commonly physiological, but unconjugated hyperbilirubinaemia may have many causes including haemolytic disease, ABO incompatibility and G-6-PD deficiency.
- Guidelines for the management of neonatal jaundice are derived from the belief that bilirubin levels greater than 340 micromol/l in term infants can cause deafness and kernicterus. The level is lower in preterm or sick infants, but accurate numbers to use are uncertain.
- Phototherapy is the usual treatment, but exchange transfusion is required for very high levels.
- Many authorities advise a more relaxed view of jaundice and jaundice in the case of newborn view.
- Prolonged jaundice which lasts more than 14 days in full-term infants and 21 days in preterm infants requires investigation to exclude things like hypothyroidism, urinary tract infection, and biliary atresia.
Hypoglycaemia
- Blood glucose level is only one measure avail- able of metabolic fuel and in term infants who are able to produce and utilize ketones, it is not easy to define an unequivocal level at which the baby is at risk of the neu- rological sequelae of hypoglycaemia.
- Authorities differ, but a pragmatic solution is to consider term infants with two consecutive blood glucose levels below 2 mmol/l (or a single blood glucose level below 1 mmol/l in inter- vention. The blood glucose must be measured using an accurate device as commercial test strips are not adequate for making the diagnosis of hypoglycaemia.
- Conditions commonly associated with transient low blood glucose are hypothermia, infection, prematurity, intrauterine growth retardation and maternal diabetes.
- Some infants develop transient hyperinsulinaemia, particularly those with stressed mothers with poor ante- natal control of diabetes.
- These babies may need very high glucose infusion rates to keep blood glucose normal.
- Persistent low blood glucose can be caused by hormone defects such as glycogenolysis, are much less able to mount a ketotic response and hypoglycaemia should be treated promptly.
Treatment
- Treatment is initially to give calories in the form of milk or intravenous glucose infusions. Rapid bolus injec- tions of concentrated glucose solutions (20-50%) are not recommended. If hypoglycaemia persists investigations, including insulin measurements, are required.
Infections
- Newborn infants are particularly prone to perinatal infec- tion. Risk factors include low birthweight infants, pro- longed rupture of membranes, maternal fever or chorio- amnionitis, foul smelling liquor, and problems for those undergoing intensive care: the presence of indwelling cannulae, central venous lines and invasive mechanical ventilation increase the risk.
- Organisms responsible for later neonatal infection frequently come from the skin or gut. Breastfeeding helps promote normal gut flora and reduces the risk of acquired neonatal infections. Adher- ence to good hand-washing practices by all staff, parents and visitors can significantly reduce the risk of acquired infection.
Septicaemia
- The signs of systemic sepsis are non-specific. Infants may present with apnoea, bradycardia or cyanotic episodes; poor feeding is a common association. They may be lethargic and hypotonic and they are hyper or hypother- mic. Sepsis frequently presents as a metabolic acidosis or shock and occasionally causes petechial skin rash or severe jaundice.
- Organisms which commonly cause infection in the new- such as Escherichia coli or Klebsiella. The prolonged use may increase the risk of infection with resistant organisms.
- Rapid treatment with antibiotics, immediate resuscitation and frequent, mechanical ventilation is required. Inves- tigations include chest X-ray, blood cultures, urine culture, and examination and culture of the placenta. A lum- bar puncture is performed once the baby is stable and will tolerate the procedure. The mortality of infants who develop septicaemia in the neonatal period is high with a significant number of survivors developing subsequent impairment.
Group B streptococcus infection
- Mortality due to maternal colonization by Group B strep- tococcus (GBS) is reduced by antibiotic therapy to the mother during labour and early treatment of infants with evidence of infection.
- About 25% of infants of colonized mothers develop infections, and 70% of these manifest
Meningitis
- Signs of meningitis in newborn infants are non-specific with a bulging fontanelle, opisthotonos and seizures occur- late in the disease. Meningitis usually presents as sep- ticaemia and can be complicated by cerebral oedema, cerebral infarction, brain abscess or deafness.
- Common causal organisms are GBS and E. coli. Listeria monocyto- genes is a rare cause of perinatal infection in the United Kingdom.
Urinary tract infection
- Urinary tract infections may present as jaundice, vomiting, poor feeding or septicaemia. The main cause is believed to be spread of blood-borne organisms to the kidney during septicaemia.
- Further investigations are essential to exclude associated urinary tract abnormalities such as vesicoureteric reflux or ureterocoele. Breastfeeding offers a significant degree of protection.
Eye infection
- The majority of sticky eyes are not infected but are due to a blocked nasolacrimal duct. In the absence of conjunc- tival redness or swelling investigation for infection and treatment with topical antibiotics is not required. Simple measures such as clearing with boiled water and lacrimal duct massage suffice with symptoms usually resolving in 3-6 months. Neonatal conjunctivitis can be caused by such organisms as Staphylococcus aureus, Chlamydia trachomatis, Haemophilus influenzae, Streptococcus pneumoniae and Neis- seria gonorrhoeae. Gonococcal ophthalmia usually presents within 24 h of delivery with profuse purulent conjunctival discharge and immediate diagnosis and treatment (sys- temic and topical) is required to prevent damage to the cornea.
- Chlamydial ophthalmia which is now among the com- monest causes of neonatal conjunctivitis presents between 5 and 12 days postnatal age: some babies infected as neonates will develop neonatal pneumonia later in infancy. Corneal scarring is rare. 14 days systemic and topical treatment is required. The identification of either
Skin infection
- Simple hygienic methods such as bathing, hand washing and routine umbilical cord care can prevent many skin infections. The infant's skin is vulnerable to infection by Staphylococcus, which usually leads to small pustules or lesions but can also cause sealed skin syndrome with severe exfoliation. Staphylococcal infections should there- fore be treated with antibiotics after appropriate cultures have been taken. Streptococcus can also cause skin infection and may lead to more serious disorders. Commonly limited to perumbilical redness with a small amount of discharge. The presence of indwelling umbilical catheters increases the risk of acquired periumbilical infection.
- The presence of oedema indicating cellulitis can occasion- ally lead to complications such as spreading cellulitis of the abdominal wall, fascia and sepsisemia and requires treatment with systemic antibiotics.
Tuberculosis
- Tuberculosis is a re-emergent disease and many hospitals now offer BCG vaccine and keep mothers infected with active tuberculosis should be vaccinated with isoniazid- resistant BCG vaccine and kept with the mother while both receive treatment with appropriate drugs. Breastfeeding should be encouraged.
- Expert advice on drug therapy is advisable as patterns of antibiotic susceptibility change over time.
Tetanus
- Neonatal tetanus due to infection of the umbilical stump by Clostridium tetani is the result of poor hygiene and is a distressing and severe condition with extremely high mor- tality. Opisthotonus and muscle spasms of the jaw and limbs are presenting features and can appear very rapidly after birth.
- Prevention centres on maternal vaccination during pregnancy and education to improve hygiene and change of local cultural practices.
Gastrointestinal disorders
Oesophageal atresia or tracheo-oesophageal fistula
- These conditions should be suspected when there is poly- hydramnios or excessive mucus from the mouth at birth. The baby may show rapid onset of respiratory stress and cyanosis particularly after the first feed. X-ray confirms the diagnosis; the naso- or orogastric tube does not pass into the stomach. A large bore nasogastric tube should be placed in the oesophageal pouch, constant suction and regular aspiration help prevent aspiration pneumonia.
- Associated congenital anomalies occur in 50% or more of infants. Surgery involves division of the fistula and anastomosis if not possible primary anastomosis is not possible, a gastrostomy repair.
- If primary anastomosis is not possible long-term complications include oesophageal repair. Common long-term complications
Diaphragmatic hernia
- Herniation of the abdominal contents into the hemithorax leads to severe respiratory difficulty with persistent pul- monary hypertension and atresia of both lungs. Essential management is to stabilize the infant prior to surgery with high rate ventilation, inotropic support, nitric oxide and in some centres extracorporeal membrane oxygenation.
Abdominal Wall Defections
- Our own management of all of the intestine and abdominal organs are a perinatal sack outside the abdomen, should be differentiated from gastrochisis where a congenital defect of the abdominal wall allows herniation of the abdominal contents without a peritoneal sac. The former is frequently associated with other con- genital defects, while the latter is not. Urgent surgery is Immediately after the amniotic sac breaks, wrap the abdominal contents in a plastic wrapper, taking care not to twist the bowel, and ensure proper support. This helps prevent hypovolemia due to fluid loss from the exposed bowel.- Insert a large bore nasogastric tube.
- Hypovolemia or excessive nasogastric output should be managed with 20 ml/kg of 0.9% sodium chloride bolus intravenous infusions. The risk of hypothermia is high unless good thermal management is present from birth. Primary repair is not always possible if the abdominal cavity is not large enough to accommodate all the contents; a silo made of sterile prosthetic material is attached to the abdominal wall and the contents gradually reduced over 7-10 days.
- Outcomes are worse for those requiring silo treatment as infected complications are high. The long-term outcome for most with exomphalos is determined by the presence of associated congenital anomalies. In gastroschisis 90% are now survive. However, their postnatal course is often protracted and parenteral nutrition may be required for several weeks with its risks and complications. In addition, bowel atresias and necrotizing enterocolitis may develop.
Intestinal obstruction
- High intestinal obstructions usually present with vomiting which may be bile-stained, and this ominous sign demands urgent investigation. Plain X-ray films of the abdomen can confirm the presence of obstruction showing a lack of air in the lower gut or a characteristic 'double bubble' of duodenal atresia. Hyperperistaltic waves may be visible and the abdomen may be distended in the upper part.
- Lower intestinal obstruction usually presents failure to pass meconium and abdominal distension with vomiting.
- A required if the amniotic sac has broken and for gastrochi- sis. Immediate management is to wrap the abdominal con- tents in a plastic fragment to prevent heat, fluid and pro- tein loss. A nasogastric tube is passed to decompress the bowel and disrupt its vascular supply. This should be excluded. Hyperperistaltic waves may be visible and the abdomen may be distended in the upper part.
- Lower intestinal obstruction usually presents with failure to pass meconium and abdominal distension with vomiting.
- A plain X-ray may show multiple dilated loops of bowel, but further investigations are needed to establish the cause. The commonest cause of low intestinal obstruction is Hirschsprung's disease, meconium ileus or atresia.
Necrotizing enterocolitis
- This poorly understood inflammatory condition is primar- ily a condition of preterm infants and those with congenital heart disease. It presents as an acute abdomen in the days or weeks after birth and varies in severity from mild to fatal. Diagnosis is clinical, aided by characteristic X-ray changes such as air in the bowel wall or biliary tree. Treat- ment is conservative with cessation of enteral feeding and with antibiotics or surgery.
Neonatal necrotizing enterocolitis
- This poorly understood inflammatory condition is primar- ily a condition of preterm infants and those with congenital heart disease. It presents as an acute abdomen in the days or weeks after birth and varies in severity from mild to fatal. Diagnosis is clinical, aided by characteristic X-ray changes such as air in the bowel wall or biliary tree. Treat- ment is conservative with cessation of enteral feeding and with antibiotics or surgery.
Low bowel atresia or hypoplasia and imperforate anus
- A meconium plug can sometimes mimic obstruction espe- cially in preterm infants.
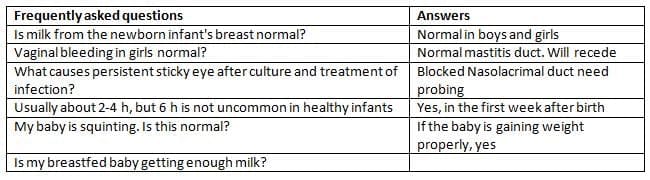
Common queries from parents
- Many minor alterations to physiology cause alarm to par- ents. Some common questions and responses are outlined in Table 11.6.
FAQs on Chapter Notes: Neonatal care for obstetricians
| 1. What are the key aspects of temperature control in newborns after birth? |  |
| 2. What are the primary steps involved in the resuscitation of a newborn? | |
| 3. How is jaundice in newborns diagnosed and managed? | |
| 4. What are the signs and risks associated with hypoglycemia in newborns? | |
| 5. What are the common disorders observed during the newborn period? | |



