Chapter Notes: Induction and augmentation of labour


Introduction
A typical pregnancy concludes with three stages:
- Pre-labour
- Cervical ripening
- Labour
- These stages occur as a continuum rather than as separate events. Endogenous prostaglandins are involved in all these processes. Interventions designed to artificially ripen the cervix, induce uterine contractions, and enhance labour once it has started also lack clear boundaries.
- This chapter will briefly outline reasons for these interventions and methods that may be used.
- Labour induction and augmentation can cause conflict and distress.
- While most health workers consider these procedures to be routine and technical, many women associate them with emotional challenges, leading to feelings of uncertainty and reduced self-worth.
- It is crucial for health workers to approach labour induction with sensitivity and to include women in the decision-making process.
- Labour induction is among the most common interventions in obstetrics.
- It is a significant intervention in the normal course of pregnancy, with the potential to trigger a series of further interventions, particularly Caesarean sections.
- However, with modern methods of labour induction, the risk of needing a Caesarean section seems to have decreased.
When to Induce Labour
- Inducing labour is a decision that requires careful clinical judgement.
- Several factors influence this choice, including whether to allow the pregnancy to continue, induce labour, or opt for an elective cesarean section.
- Benefits and Risks to the Mother
- Benefits for the mother include:
- Improving medical conditions exacerbated by pregnancy, such as pre-eclampsia or placental abruption.
- Alleviating discomfort from multiple pregnancies, polyhydramnios, or previous surgical interventions.
- Initiating necessary treatments, such as for cervical cancer.
- Easing emotional distress following intrauterine death.
- Reducing anxiety regarding the baby's health.
- Risks for the mother include:
- Increased pain and the need for pain relief measures.
- Potential for uterine hyperstimulation.
- Risk of cesarean section, infections, and other complications.
- Postpartum bleeding and rare instances of uterine rupture.
- Anxiety if the induction process is prolonged or unsuccessful, and feelings of inadequacy for not experiencing a natural birth.
- Benefits for the mother include:
- Benefits and Risks to the Baby
- Benefits for the baby include:
- Improved growth and development in cases of suboptimal growth.
- Reduced risk of intrauterine death due to complications like diabetes or prolonged pregnancy.
- Risks for the baby include:
- Prematurity and associated complications from uterine hyperstimulation.
- Benefits for the baby include:
Factors Influencing the Decision
- The health and condition of the mother.
- The health and condition of the baby.
- The gestational age of the baby and the certainty regarding its age. In cases of uncertainty about lung maturity, amniocentesis may be conducted to assess markers such as the lecithin/sphingomyelin ratio.
- The mother's history of previous cesarean sections.
- The preferences and wishes of the mother.
- The likelihood of successful and efficient induction leading to vaginal delivery, which is influenced by the condition of the uterine cervix.
Cervical 'Ripeness' Before Labor
- In the days or weeks leading up to labor, the cervix undergoes a process of softening, shortening, and partial dilation. However, the timing of this process can vary significantly among individuals.
- A cervix that is considered 'unripe' has not undergone these changes and is therefore less responsive to attempts to induce labor.
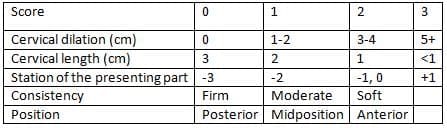
Modified 'Bishop' cervical score
Cervical Composition and Changes During Pregnancy
- The cervix is made up of approximately 50% collagen, 20% smooth muscle, and the remaining portion consists of elastin and glycosaminoglycans.
- During pregnancy, the levels of hyaluronidase in the cervix increase significantly, while the levels of dermatan and chondroitin, which tightly bind collagen, decrease.
- Enzymes like collagenase and elastase also increase during this period, along with enhanced vascularity and water content in the cervix.
Modified Bishop Cervical Score
- In 1964, Bishop introduced a clinical scoring method for assessing cervical readiness for labor, which has since been updated.
- A Bishop score of 6 or higher indicates a favorable condition for successful induction of labor.
- A score of 5 or lower suggests an unfavorable condition, where methods like artificial rupture of the amniotic sac and oxytocin infusion are less likely to be successful.
Fibronectin Measurement
- Recently, measuring fibronectin levels in cervicovaginal secretions has been explored as a method to predict the onset of labor, although its effectiveness varies.
Guidelines from the Royal College of Obstetricians and Gynaecologists
The Royal College of Obstetricians and Gynaecologists suggests the following guidelines:
- Ultrasound Scan: Offer an ultrasound scan before 20 weeks of pregnancy to confirm the gestational age.
- Membrane Sweeping: Perform membrane sweeping after 40 weeks of pregnancy.
- Inducing Labour: Induce labour routinely after 41 weeks of pregnancy.
- Fetal Monitoring: If induction is declined, start fetal monitoring at 42 weeks. Induction of labour is suggested if monitoring shows abnormalities.
- Pregnancy Complications: In cases of pregnancy complications, offer membrane sweeping or labour induction at the appropriate gestational age.
Methods of Inducing Labour with a Favourable Cervix
Artificial Rupture of Membranes (Amniotomy)
- Definition: Amniotomy involves the artificial rupture of the amniotic membranes to induce labour.
- Procedure: This can be done using toothed forceps or a specially designed plastic hook.
- Timing: Depending on the urgency of the situation, an oxytocin infusion may start simultaneously with amniotomy or later if progress is slow.
Oxytocin Administration
- Myometrium Response: The myometrium's reaction to oxytocin varies significantly, necessitating a variable dose infusion adjusted based on uterine contractions.
- Starting Dose:. typical starting dose is 1 mU/min, doubling every 20-30 minutes until adequate contractions are achieved or a maximum of 32 mU/min is reached.
- Labour Establishment: Once labour is established, the infusion rate can be gradually reduced to about 7 mU/min as sensitivity increases.
- Infection Considerations: Amniotomy should be avoided if the woman's infection status is unknown (e.g., HIV, hepatitis). In such cases, oxytocin can be administered with intact membranes.
Use of Prostaglandins
- Indication: Prostaglandins are preferred for inducing labour with an unfavourable cervix, as amniotomy and/or oxytocin are usually ineffective in such cases.
- Flexibility: Prostaglandins can also be used for some cases with a favourable cervix.
- Effectiveness: Some studies suggest that various prostaglandins, such as misoprostol, may be more effective than oxytocin infusion for induction with a favourable cervix.
- Patient Satisfaction: Prostaglandins often lead to greater satisfaction among women undergoing induction.
Methods for Inducing Labour with an Unfavourable Cervix
- When the cervix is not favourable, the primary method for inducing labour involves the use of exogenous prostaglandins or techniques that promote the release of endogenous prostaglandins.
- These methods aim to soften the cervix and initiate contractions.
Prostaglandins for Labour Induction
- The practice of using prostaglandin F2 alpha to induce labour dates back to the 1960s. Subsequently, prostaglandin E2 (PGE2, dinoprostone) was developed and largely replaced F2 alpha.
- PGE2 is primarily administered vaginally, with various forms available, including:
- Tablets
- Suppositories
- Gels
- Pessaries
- Research indicated that a 10-mg PGE2 vaginal insert performed comparably to 3 mg PGE2 vaginal tablets taken twice every 6 hours. In cases of uterine hyperstimulation, removing the vaginal insert often sufficed to restore normal uterine activity.
- In contrast, a significant number of women in the PGE2 tablet group required medical intervention for hyperstimulation.
Various dosages and timings for PGE2 administration exist, but its use has been restricted in some countries due to cost considerations. - The Royal College of Obstetricians and Gynaecologists recommends vaginal prostaglandins for initiating cervical ripening or labour induction in both favourable and unfavourable cervices.
- Specifically, they advise:
- PGE2 tablets (3 mg every 6 to 8 hours, with a maximum total of 6 mg)
- PGE2 gel (2 mg for nulliparous women with a modified Bishop cervical score < 4, 1 mg for all others, repeated every 6 hours to a maximum of 4mg
- In cases where the membranes have ruptured, intravenous oxytocin is recommended as an alternative starting agent.
- Oxytocin is most effective when the membranes are ruptured. If used after PGE2, a gap of 6 hours after the last vaginal dose of PGE2 is advised to reduce the risk of uterine hyperstimulation.
Comparison of Methods for Inducing Labour
- Vaginal PGE2 is widely recognized as a standard method for inducing labour. Other methods, which are less established, will be compared to PGE2 as the 'gold standard'. Special focus will be given to misoprostol due to the ongoing debate about its use and the amount of recent research on it.
- Comparisons of alternative methods are best based on results from randomized clinical trials.
- To manage the complexity of hundreds of reported trials comparing various combinations of 25 labour induction methods, the Pregnancy and Childbirth Group of the Cochrane Collaboration, along with the Clinical Effectiveness Support Unit of the Royal College of Obstetricians and Gynaecologists, developed a strategy.
- This involved reviewing clearly defined clusters of comparisons in a series of systematic reviews using standardized outcomes and clinical subgroups.
Effectiveness and Risks
- A key issue in these comparisons is that one method may seem more effective just because a larger dosage was used.
- The most important factor is the relationship between effectiveness and the risk of uterine hyperstimulation, which can affect fetal health and increase the risk of uterine rupture.
- In the last column of Table 23.2, the relative risk of failed delivery within 24 hours is multiplied by the relative risk of uterine hyperstimulation with fetal heart rate changes.
- This result provides a rough indication of efficiency (the balance between effectiveness and hyperstimulation) for each method compared to PGE2 as the 'gold standard'.
- According to this method, the efficiency of mechanical methods appears to be better, while vaginal misoprostol is less effective.
- Oral misoprostol and oxytocin with amniotomy show similar efficiency to that of PGE2.
- There were too few data on vaginal PGF2-alpha to comment.
Intracervical Prostaglandins
- Prostaglandin E2 (PGE2) can be administered directly into the cervical canal in smaller doses compared to vaginal administration.
- The goal is to enhance the local effect on the cervix. However, this method is more complex, and there are no clear advantages over vaginal administration.
Intravenous Oxytocin Alone
- Traditionally, oxytocin is used in conjunction with amniotomy.
- In regions with high HIV prevalence, amniotomy is avoided in women with unknown HIV status.
- However, using oxytocin alone without amniotomy is significantly less effective than vaginal PGE2 for inducing labor in women with an unfavorable cervix.
Amniotomy and Its Effects
- Artificially rupturing the amniotic membranes through the cervix has been a recognized method for inducing labor for over 200 years.
- A rise in prostaglandin metabolites has been shown to relate to the time from induction to delivery after rupturing the membranes.
- This method has some benefits:
- Avoids the use of external uterine stimulants, reducing the risk of uterine hyperstimulation.
- Allows for monitoring of the amniotic fluid.
- However, there are also downsides:
- The procedure may cause discomfort for the patient.
- It can lead to the risk of ascending infections.
- Prolonged rupture of membranes may raise the risk of fetal infections, including HIV.
- The procedure might put the fetus at higher risk of HIV if the skin of the presenting part is scratched during labor.
- With an unfavorable cervix, amniotomy is often not technically feasible.
Intravenous Oxytocin with Amniotomy
- The use of intravenous oxytocin combined with amniotomy is a common practice.
- This method is typically applied to women who have a cervix that is in a favorable condition for labor.
- Intravenous oxytocin is a hormone that helps to stimulate contractions during childbirth.
- Amniotomy involves artificially breaking the amniotic sac to help speed up labor.
- The combination of these two approaches can enhance the labor process for women who are ready to give birth.
- This treatment is often considered when the cervix is already softened and dilated enough for labor to progress.
Misoprostol
- Misoprostol is a stable form of prostaglandin E1 that can be taken orally.
- It is commonly used in Obstetrics and Gynecology, although its approval varies by country.
- The American College of Obstetricians and Gynecologists recommends using misoprostol at a dose of 25 µg every 3 to 6 hours for effective labor induction, based on level A evidence.
- A higher dose of 50 µg every 6 hours may be appropriate in some cases, but it carries a greater risk of complications, as indicated by level B evidence.
Various Methods of Labour Induction
The outcomes observed when comparing different methods of labor induction to vaginal PGE2, which is considered the 'gold standard,' are as follows:
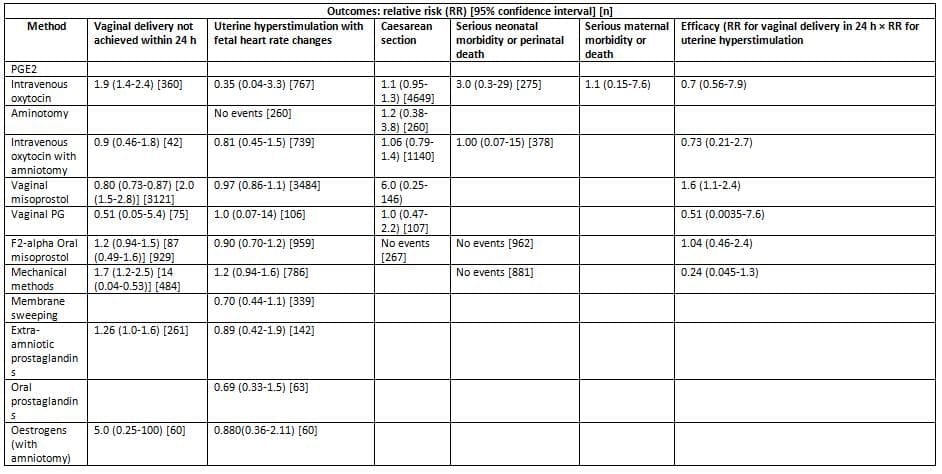
The values presented indicate the relative risks associated with each method, along with 95% confidence intervals and sample sizes [n]. A relative risk of less than 1 suggests that the outcome occurred less frequently with the method compared to PGE2.
Effectiveness of Misoprostol
- In most dosage regimens, misoprostol is at least as effective as standard methods of inducing labour.
- Doses above 25 µg every 4-6 hours vaginally result in fewer failures to deliver vaginally within 24 hours compared to dinoprostone.
- The improved effectiveness of misoprostol is linked to quicker cervical ripening.
Oral versus Vaginal Route of Administration of Misoprostol
- Oral Administration of Misoprostol:
- 400 µg misoprostol taken orally leads to:
- Shorter time to peak serum level: 34 minutes (compared to 80 minutes for vaginal use).
- Higher peak serum level: Faster initial increase in uterine tone.
- Shorter duration of activity: Resulting in a quicker but less lasting effect.
- Dosing Schedule:
- Due to the short action of oral misoprostol, a dosing schedule of:
- Every 2 hours, starting with 20 µg, and increasing to 40 µg after 2-3 doses if needed.
- Preparation of Doses:
- To ensure accurate dosing, 200 µg of misoprostol was dissolved in 200 mL of water and mixed well before each dose.
- The solution was discarded after 12 hours.
- Clinical Trial Comparison:
- In a multicentre randomised trial with 695 women, oral misoprostol was found to be as effective as vaginal dinoprostone 2 mg (repeated every 6 hours) in terms of:
- Effectiveness, uterine hyperstimulation, Caesarean section rates, and perinatal outcomes.
- Dose Adjustment:
- To align with standard dosages:
- Adjusted the dose to 25 µg every 2 hours.
- In nulliparous women, the dose may be increased to 50 µg every 2 hours only if necessary.
- Systematic Review Findings:
- A systematic review of randomised trials comparing oral and vaginal routes found that:
- Oral route was linked to slower labours but fewer Caesarean sections.
Buccal or Sublingual Misoprostol
- The sublingual route provides a rapid onset similar to the oral method, while also offering a prolonged effect and superior absorption compared to the vaginal route.
- The buccal route should be used with caution, as dosages may need to be significantly reduced for safety.
Rectal Misoprostol
- A small study suggested that the effectiveness of labor induction is comparable whether misoprostol is administered vaginally or rectally.
Dosage of Vaginal Misoprostol
- A systematic review examined lower dosages (ranging from 25 µg every 6 hours to 50 µg every 4 hours) of vaginal misoprostol in comparison to higher dosages.
- The findings indicated that lower dosages necessitated more oxytocin, had similar rates of delivery within 24 hours, and comparable rates of Caesarean sections.
- Lower dosages were associated with significantly reduced instances of uterine hyper-stimulation.
- There is robust evidence supporting the use of a small dose (e.g., 25 µg. at least initially.
Complications Associated with Misoprostol
- The primary safety concerns with misoprostol involve uterine hyperstimulation and its potential impacts on both the mother and the baby.
- A systematic review indicated that vaginal misoprostol, at the dosages commonly used, was associated with a higher incidence of uterine hyperstimulation accompanied by non-reassuring fetal heart rate changes when compared to PGE2.
- Misoprostol's greater potency as a uterine stimulant complicates the assessment of whether the observed differences are due to its pharmacological characteristics or merely the dosage administered.
Meconium-Stained Liquor
- The occurrence of meconium-stained liquor is significantly higher with labour induction using misoprostol compared to either vaginal or intracervical PGE2.
- It has been proposed that certain myometrial stimulants might cross the placenta and stimulate the fetal bowel, leading to the passage of meconium.
- However, studies show that misoprostol and dinoprostone have comparable effects on the rat ileum relative to their myometrial effects.
- Another possible reason for the increased meconium passage during misoprostol induction is that misoprostol is resistant to placental 15-hydroxyprostaglandin dehydrogenase, allowing it to enter fetal circulation more readily than PGE2.
Precipitate Delivery
- Precipitate delivery, defined as labour lasting less than 2 hours, has been noted as a potential complication of misoprostol induction.
- However, most reviews and trials have not documented its occurrence, and the 'mean time to delivery' is often highlighted as a key outcome measure.
- Precipitate deliveries may contribute to seemingly favourable mean induction to delivery times without being recognised as negative outcomes.
- The significance of precipitate delivery lies in its potential indication of an excessive uterine response to misoprostol, raising concerns about the risk of uterine complications.
Rupture of the Unscarred Uterus
- Numerous cases have reported the rupture of an unscarred uterus following induction with misoprostol, including incidents of maternal death occurring shortly after induction with a single 50 µg dose in healthy women with uneffaced cervices.
- Without a reliable comparative framework, it remains unclear whether the risk of uterine rupture with misoprostol is higher or lower than with other induction methods.
Women with Previous Caesarean Section
- Several instances of uterine scar rupture have been documented following misoprostol induction in women with a history of Caesarean section.
- A recent retrospective study found a significantly higher incidence of uterine rupture or dehiscence with misoprostol compared to oxytocin or prostaglandin E2.
- As a precaution, misoprostol should not be used in women with uterine scars.
Caesarean Section
- The relationship between misoprostol use and the rate of Caesarean sections is complex and not straightforward.
- Randomised trials have indicated an increase in Caesarean sections due to fetal heart rate abnormalities associated with misoprostol use, while there has been a decrease in Caesarean sections for slow labour progress, leading to an overall reduction in Caesarean rates.
Perinatal Outcome
- Despite the increased incidence of uterine hyperstimulation with misoprostol, most reviews and trials have not shown a significant difference in perinatal outcomes when compared to other induction methods.
Post-Partum Haemorrhage
- A retrospective study observed a higher rate of post-partum haemorrhage with misoprostol induction compared to the general obstetric population.
- A randomised trial found a greater occurrence of post-partum haemorrhage with vaginal misoprostol 50 µg compared to 25 µg administered every 4 hours.
Conclusion
- Misoprostol is an effective agent for inducing labour, but there are concerns regarding potential complications such as uterine hyperstimulation, precipitate labour, meconium-stained liquor, uterine rupture, and post-partum haemorrhage.
- The risks associated with misoprostol induction may be reduced with smaller dosages, with a recommended starting dose not exceeding 25 µg either vaginally or orally.
- There is limited evidence supporting the use of the oral route over the vaginal route for misoprostol administration.
- Further large-scale randomised trials comparing low-dose misoprostol regimens with conventional induction methods are necessary to gain a better understanding of the rates of rare adverse outcomes.
Mechanical Techniques for Inducing Labor, Including the Extra-Amniotic Foley Catheter
- Mechanical methods for cervical ripening are among the oldest techniques used for labor induction.
- These methods work by physically stretching the cervix and stimulating its internal mechanisms to release endogenous prostaglandins, which play a crucial role in preparing the cervix for labor.
- The use of an extra-amniotic balloon catheter, such as a Foley catheter or the 'Atad' double balloon catheter, is generally slower in effect compared to PGE2 (prostaglandin E2).
- This method is associated with a lower risk of uterine hyperstimulation and fewer alterations in fetal heart rate.
- Additionally, it results in fewer cesarean sections.
- When compared to misoprostol (50 µg every four hours), there are no significant differences in terms of cervical ripening or the overall success of labor induction.
- Furthermore, the use of an extra-amniotic balloon catheter is linked to fewer issues related to uterine contractions and instances of meconium-stained liquor.
Extra-Amniotic Saline Infusion
- The extra-amniotic balloon catheter 's stimulating effect may be enhanced by infusing normal saline into the extra-amniotic space at a rate of 50 ml/h.
- In a randomised study, extra-amniotic saline infusion via a Foley catheter was compared to vaginal misoprostol(25 µg every 4 hours).
- This method was associated with:
- A shorter time to delivery
- Fewer instances of abnormal fetal heart rate tracings
- Less frequent tachysystole.
- There were no differences in delivery routes or neonatal outcomes
- Oxytocin was used as needed in both groups
Effectiveness and Safety
- Limited data from randomised trials suggest that extra-amniotic saline infusion is an effective method for labour induction and may be safer than methods involving exogenous uterine stimulants.
Membrane Separation Procedure
- Separating the membranes from the lower uterine segment by making a circular motion with a finger inserted through the cervix is a common practice to facilitate labour.
- This procedure is linked to:
- An increase in circulating prostaglandins, and
- A decrease in the necessity for formal labour inductions.
- However, this procedure can be uncomfortable and is not feasible when the cervix is closed or positioned very posteriorly.
Castor Oil, Baths, and/or Enemas
- Castor oil, baths, and enemas are traditional methods used to help initiate labour.
- However, only one randomised trial has investigated the use of castor oil, and the results were inconclusive.
- There is a potential link between castor oil, which functions as a laxative, and the occurrence of meconium passage, possibly due to a direct impact on the baby's intestines.
Other Methods
- The following labour induction methods lack sufficient evidence to support their effectiveness, and it is also unclear how they compare to the previously mentioned methods:
- Extra-amniotic prostaglandins
- Intravenous prostaglandins
- Oral prostaglandins
- Mifepristone
- Estrogens
- Corticosteroids
- Relaxin
- Hyaluronidase
- Acupuncture
- Breast stimulation
- Sexual intercourse
- Homeopathic methods
Induction of Labour Following a Previous Caesarean Section
- A retrospective study examining the rates of uterine scar rupture found the following:
- 2.5% for labours induced with prostaglandins
- 0.77% for other methods of labour induction
- 0.52% for spontaneous labour
- The American College of Obstetricians and Gynecologists' Committee on Obstetric Practice determined that the use of various prostaglandin agents for labour induction significantly increases the risk of uterine rupture during attempts at vaginal birth after a Caesarean section. Therefore, their use is discouraged. Considering the evidence related to uterine hyperstimulation, the following methods are regarded as the safest for labour induction after
- Caesarean section:
- Extra-amniotic saline infusion.
- Amniotomy alone when the cervix is favourable.
- At present, there is no direct evidence to validate this assumption.
Preterm Labour Induction
- Inducing labour before the due date often means the cervix isn't prepared yet.
- A recent study found that preterm labours are usually shorter.
- Preterm labours also have fewer cases of serious post-partum haemorrhage compared to those induced at term or post-term using PGE2 gel.
Augmentation of Labour
- Spontaneous labour typically begins with a latent phase, which can vary in length.
- This is followed by an active phase where the cervix dilates rapidly.
- The active phase usually commences when the cervix is 3 cm dilated and fully effaced.
Enhancing the Latent Phase of Labour
- Identifying the latent phase of labour in advance can be challenging, as late pregnancy may involve painful contractions that resemble true labour but do not progress to the active stage.
- As a result, deciding to augment the latent phase is more akin to inducing labour rather than augmenting the active phase.
- It is crucial to consider the potential benefits and risks while also taking into account the emotional stress caused by the uncertainty of when labour will begin.
- Amniotomy followed by oxytocin infusion, either simultaneously or if the response to amniotomy alone is insufficient.
- For women whose HIV status is not confirmed, either oxytocin alone or prostaglandins may be used, depending on the circumstances, similar to labour induction.
- Extra-amniotic saline infusion might be considered if the cervix is narrow enough to accommodate the Foley catheter bulb.
Enhancing the Active Phase of Labour
- Active Management of Labour: This approach, introduced by O'Driscoll and colleagues in the 1960s, can routinely enhance the active phase of labour or be used selectively when progress is insufficient due to poor uterine efficiency.
- It involves:
- Strict criteria for diagnosing labour
- Amniotomy (artificial rupture of membranes)
- Oxytocin infusion
- Ensuring one-to-one support from a healthcare team member for the woman in labour
- Aiming for quicker delivery
- Routine Amniotomy: Linked to shorter labour duration (typically 1-2 hours).
- Oxytocin Use: Associated with lower 5-minute Apgar scores and a higher likelihood of Caesarean sections.
- Continuous Support During Labour Cochrane systematic review found that continuous support leads to:
- Less use of analgesia
- Fewer operative deliveries
- Greater satisfaction with the childbirth experience
- Non-significant reduction in labour duration
- Continuous support is recommended for all women during labour.
Diagnosing Ineffective Uterine Activity: This is crucial for augmenting labour. It can be challenging to differentiate between a prolonged latent phase and slow progress in the active phase. A careful diagnosis helps clarify these stages. - Monitoring Labour Progress: Best tracked using a graphical representation of cervical dilation and descent of the presenting part over time, known as the partograph. Various modifications of the partograph exist.
- Criteria for Inadequate Labour Progress: Labour progress is considered inadequate when cervical dilation is delayed by 2 or 4 hours beyond the expected rate (1 cm/h).
- Presuming Inadequate Uterine Activity: If there is no sign of fetopelvic disproportion, inadequate uterine activity is presumed, and labour is augmented.
- Monitoring Uterine Activity: Intrauterine pressure monitoring can provide an objective assessment of uterine activity. Optimal contractions are considered to be every 3 minutes, lasting 45 seconds, with intrauterine pressures of 60-80 mmHg.
- External Assessment of Uterine Contractions: This can be done through palpation or indirect tocography to track duration and frequency, but not intensity.
- Labour Augmentation in Women with Previous Caesarean Sections: This is a controversial issue. In cases of breech presentation, poor progress in the active phase may indicate fetopelvic disproportion, where a Caesarean section is preferred over augmentation.
- Methods of Augmentation: When augmentation is necessary, the usual methods include:
- Amniotomy (after excluding HIV)
- Oxytocin infusion
- Considerations for Labour Induction: The focus should be on whether to induce labour rather than how to induce it. Potential benefits and risks for both mother and baby, including physical and emotional aspects and the condition of cervical tissue, should be carefully considered.
- Induction Methods: When the cervix is not ready, methods such as oxytocin infusion and/or artificial rupture of membranes are less likely to be effective.
FAQs on Chapter Notes: Induction and augmentation of labour
| 1. When should labour be induced during pregnancy? |  |
| 2. What is meant by the 'ripeness' of the uterine cervix? | |
| 3. What are the Royal College of Obstetricians and Gynaecologists guidelines on induction of labour? | |
| 4. What methods are used for the induction of labour with a favourable cervix? | |
| 5. How do prostaglandins compare to intravenous oxytocin for labour induction? | |



