NEET PG Exam > NEET PG Notes > Gynaecology and Obstetrics > Chapter Notes: Primary amenorrhoea
Chapter Notes: Primary amenorrhoea

Introduction
- Menstruation is the final step in puberty for most girls, marking sexual maturity.
- It results from a series of events starting with hypothalamic maturation in late childhood.
- Primary amenorrhoea occurs when there is a failure in this process, affecting organs involved in puberty.
- Managing primary amenorrhoea requires understanding female embryology, pubertal endocrinology, and a holistic assessment of the adolescent girl.
Definition
- Primary amenorrhoea is the absence of menstruation in a girl who has not yet menstruated.
- It is challenging to define due to the wide age range (10-18 years) when menstruation typically begins.
- It should be considered in the context of overall pubertal development, not as an isolated event.
- Investigation is recommended if no secondary sexual characteristics develop by age 14 or if menstruation does not occur within 2 years of secondary sexual characteristic development.
- Any parental concern about delayed puberty or menstruation warrants investigation, often due to comparisons with siblings.
- Confirming normality through investigation is as important as diagnosing abnormalities.
- The term "delayed puberty" is more practical than primary amenorrhoea, as it covers the entire process of reaching sexual maturity.
Normal Puberty
- Puberty is the period when a person becomes capable of reproduction, involving physical and psychological changes.
- It includes five secondary sexual characteristics in girls: breast development, pubic hair, axillary hair, growth spurt, and menstruation, followed later by ovulation.
- Breast development (Tanner classification, 5 stages) starts around age 9 and takes about 5 years to complete; absence by age 13 is unusual.
- Pubic hair development (5 stages) occurs alongside breast development.
- Axillary hair (3 stages) develops later, around age 13.
- The growth spurt occurs between ages 10-14, with peak height velocity around 12.1 years.
- Menstruation begins in 95% of UK girls by age 13, though delays up to age 16 are considered normal.
Investigative pathway for a patient with normal sexual characteristics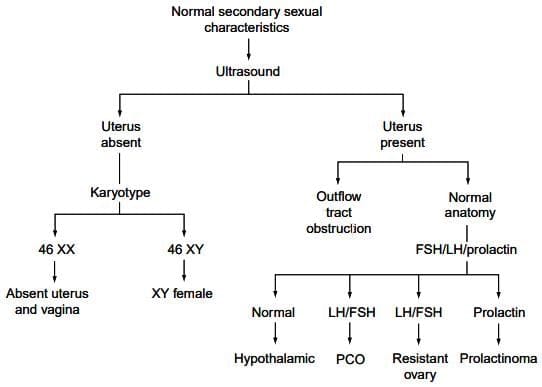 Investigative pathway for a patient with no secondary sexual characteristics
Investigative pathway for a patient with no secondary sexual characteristics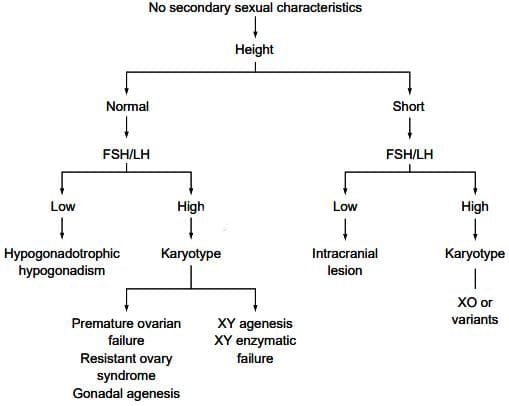
- Pubertal changes result from endocrine maturation, with low gonadotrophin levels in childhood increasing as the hypothalamus matures, releasing gonadotrophin-releasing hormone (GnRH).
- Ovarian stimulation begins around age 8.5, producing oestradiol, which drives breast development and menstruation.
- Adrenarche (rise in androgens like DHEA and DHEAS) starts around age 6, peaks by age 12, and triggers pubic and axillary hair growth.
Aetiology of Primary Amenorrhoea
- Causes are classified based on the presence or absence of secondary sexual characteristics and the presence of heterosexual development.
Classification of Primary Amenorrhoea
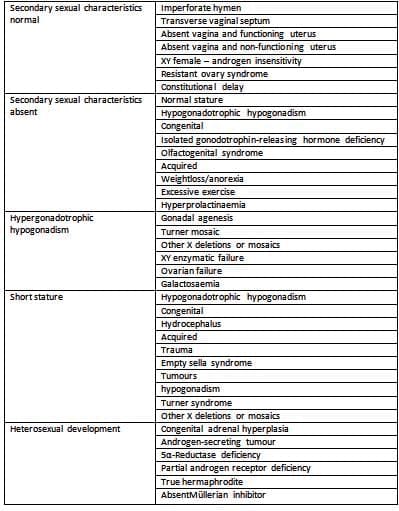
Secondary Sexual Characteristics Normal
Imperforate Hymen
- Presents in early childhood with a bulging hymen due to mucus accumulation (mucocele) or at puberty with cyclical abdominal pain from menstrual blood accumulation (haematocolpos).
- Rarely, blood accumulates in the uterus (haematometra) due to its muscular nature.
- Large masses may cause difficulty with urination or defecation.
- Examination shows an abdominal swelling and a tense, bluish hymen at the introitus.
Transverse Vaginal Septum
- Caused by failure of vaginal canalization, leading to separation of upper and lower vagina.
- Presents with cyclical abdominal pain due to haematocolpos.
- Examination shows a blind-ending, pink vagina (not bluish), with possible hymenal remnants.
- May occur at lower, middle, or upper third of the vagina; significant separation may result in no introital swelling, detectable by rectal exam.
- Requires careful assessment before management, unlike imperforate hymen.
Absent Vagina and Functioning Uterus
- Rare condition where the uterine body develops normally, but the cervix and upper vagina do not.
- Presents with cyclical abdominal pain but no pelvic mass due to absent vagina.
- Retrograde menstruation may lead to endometriosis and pelvic adhesions.
Absent Vagina and Non Functioning Uterus
- Second most common cause of primary amenorrhoea (after Turner syndrome), known as Meyer-Rokitansky-Kuster-Hauser (MRKH) syndrome.
- Normal secondary sexual characteristics due to intact ovarian function.
- Examination shows normal female external genitalia but a blind-ending vaginal dimple (≤1.5 cm deep).
- Uterine development is rudimentary, often with small uterine remnants on pelvic side walls.
- 40% of patients have renal anomalies (15% major, e.g., absent kidney), and skeletal abnormalities are common.
XY Female
- Caused by failure of testicular development, enzymatic failure to produce testosterone, or androgen receptor defects (androgen insensitivity).
- In androgen insensitivity, a non-functional androgen receptor prevents masculinization, resulting in a female phenotype with normal breast development (due to peripheral androgen-to-oestrogen conversion).
- Pubic hair is scanty, vulva is normal, but the vagina is short, and uterus/tubes are absent.
- Testes are usually in the lower abdomen or occasionally in hernial sacs, detected during childhood surgery.
Resistant Ovary Syndrome
- Rare condition with elevated gonadotrophins despite normal ovarian tissue.
- Some secondary sexual characteristics develop, but oestrogen levels are insufficient for menstruation.
- Believed to result from absent or malfunctioning FSH receptors in ovarian follicles.
Constitutional Delay
- Normal secondary sexual characteristics with no anatomical or endocrine abnormalities.
- Caused by immature pulsatile GnRH release, confirmed by 24-hour serial sampling.
- Patients eventually menstruate spontaneously as hypothalamic maturation progresses.
Secondary Sexual Characteristics Absent (Normal Height)
Isolated GnRH Deficiency (The Olfactogenital Syndrome, Kallman Syndrome)
- Hypothalamus fails to produce GnRH, causing hypogonadotrophic hypogonadism.
- Pituitary responds normally to exogenous GnRH.
- Caused by maldevelopment of hypothalamic arcuate nucleus neurones, derived from the olfactory bulb.
- Some patients have anosmia (Kallman syndrome) due to mutations in KAL1 or FGFR1 genes, affecting olfactory and GnRH-secreting neurones.
Weight Loss/Anorexia
- More common in secondary amenorrhoea but can occur prepubertally, preventing GnRH activation.
- Results in persistent hypogonadotrophic state; growth spurt is unaffected, but secondary sexual characteristics are absent.
Excessive Exercise
- Excessive exercise (e.g., in ballet dancers, athletes, gymnasts) reduces body fat, disrupting puberty.
- Body weight may remain normal due to muscle mass, so weight alone is not a reliable indicator.
- May lead to amenorrhoea or progress to anorexia nervosa.
Hyperprolactinaemia
- Rare cause of primary amenorrhoea, more common in secondary amenorrhoea.
- May be due to a prolactinoma or idiopathic; imaging may reveal pituitary anomalies.
Gonadal Agenesis
- Complete failure of gonad development in 46XX or 46XY individuals.
- In 46XX, caused by autosomal recessive genes (location unclear); phenotype is female regardless of genotype.
- In 46XY or 45X/46XY, absence of testicular determining factor or its receptor prevents testicular development.
- No androgen or Müllerian inhibitor is produced, leading to regression of Wolffian structures and persistence of Müllerian structures.
- Menstruation occurs with oestrogen administration; external genitalia are female, and height is normal.
- In 46XY, lack of androgen/oestrogen delays epiphyseal closure, potentially causing excessive height.
Ovarian Failure
- Caused by chemotherapy or radiotherapy for childhood malignancies, leading to ovarian destruction.
Galactosaemia
- Inborn error of galactose metabolism due to deficiency of galactose-1-phosphate uridyl transferase.
- Accumulation of galactose metabolites causes ovarian cellular destruction, possibly via apoptosis, leading to hypogonadotrophic hypogonadism.
Gonadal Dysgenesis
- Abnormal gonad formation, most commonly Turner syndrome (45X karyotype, missing X or Y chromosome).
- Other causes include mosaics (e.g., 45X/46XX) or X chromosome deletions affecting gonadal development.
- In Turner syndrome, ovaries develop normally until 20 weeks gestation, but massive atresia occurs later, leaving stromal ovaries unable to produce oestrogen.
- Normal female phenotype and internal genitalia, but short stature due to loss of height genes on the X chromosome.
- In mosaics, severity depends on the proportion of 45X cells.
- In XY individuals, dysgenetic gonads with enzymatic failure prevent testosterone production, leading to Müllerian atrophy and female external phenotype with a short vagina.
Secondary Sexual Characteristics Absent (Short Stature)
Congenital Infection
- Hydrocephalus from childhood/neonatal infections damages the hypothalamus, impairing GnRH secretion and causing hypogonadotrophic hypogonadism.
Trauma
- Skull base trauma may impair hypothalamic GnRH secretion, preventing puberty.
Empty Sella Syndrome
- Rare condition with congenital absence of part or all of the pituitary gland, leading to gonadotrophin deficiency and absent secondary sexual characteristics.
Tumours
- Pituitary tumours, such as craniopharyngioma, destroy the gland, causing hypogonadotrophic hypogonadism.
- Patients often present on maintenance therapy for other hormonal deficiencies.
Turner Syndrome
- 45X karyotype causes short stature and ovarian failure.
- Patients present in teenage years due to absent secondary sexual characteristics or are referred from growth clinics for puberty induction.
- Improving height is challenging.
Heterosexual Development
Congenital Adrenal Hyperplasia
- Caused by enzyme deficiency in adrenal steroid synthesis (see Chapter 34), requiring steroid replacement.
- Poor compliance with steroid therapy delays puberty, necessitating strict control for normal pubertal development.
Androgen-Secreting Tumours
- Rare ovarian tumours (e.g., arrhenoblastoma) produce excessive androgens, causing virilization.
- Tumour removal resolves the issue.
5α-Reductase Deficiency
- XY individuals with enzyme deficiency cannot convert testosterone to 5-hydroxytestosterone, required for male external genitalia development.
- Results in female external genitalia, normal male internal genitalia, and amenorrhoea due to Müllerian agenesis.
True Hermaphrodite
- Presence of both ovarian and testicular tissue, either separately or within the same gonad.
- Causes intersex issues at birth and amenorrhoea at puberty due to androgen production disrupting the menstrual cycle.
Absent Müllerian Inhibitor
- Rare condition in XY individuals where lack of Müllerian-inhibitory substance leads to persistence of Müllerian and Wolffian structures.
- Results in dual internal genitalia and amenorrhoea.
Evaluation and Management
- Constitutional delay is the most common cause, but serious conditions must be excluded first.
- Take a detailed history and examination, focusing on secondary sexual characteristics (Tanner staging) and height.
Normal Secondary Sexual Characteristics
- Suggests possible outflow tract obstruction, the most common cause in this group.
- Avoid pelvic exams in adolescents; use pelvic ultrasound to assess anatomy.
- If ultrasound is inconclusive, use MRI or CT.
- If uterus is absent, perform karyotype:
- 46XX suggests MRKH syndrome.
- 46XY indicates XY female.
- If uterus is present with haematocolpos/haematometra, consider reconstructive surgery.
- If pelvic anatomy is normal, check gonadotrophin and prolactin levels:
- Normal levels suggest constitutional delay.
- Elevated LH/FSH ratio may indicate polycystic ovaries.
- Elevated gonadotrophins suggest resistant ovary syndrome.
- Elevated prolactin suggests prolactinoma.
Management
- Absent uterus (e.g., MRKH syndrome) requires psychological counselling and management in a specialized centre with psychosexual and gynaecological expertise.
- Address future sexual activity and infertility concerns; vaginal creation possible with dilators (85% success) or surgery.
- For XY females, counsel about 30% malignancy risk in gonads; perform gonadectomy after counselling, timing based on patient-clinician relationship.
- Share karyotype information when appropriate, based on patient readiness.
- For imperforate hymen, a cruciate incision allows drainage of menstrual blood.
- Transverse vaginal septae require complex reconstructive surgery for functional vagina.
- For constitutional delay with complete secondary sexual characteristics, annual review is sufficient; a single cycle of oral contraceptive pill may reassure by inducing menstruation.
- Resistant ovary syndrome requires ovarian biopsy to confirm absent oocytes.
- Elevated prolactin warrants pituitary imaging (CT/MRI) for microadenoma; treat with bromocriptine.
Absence of Secondary Sexual Characteristics
- Assess height:
- Normal height with low gonadotrophins indicates hypogonadotrophic hypogonadism.
- Normal height with high gonadotrophins prompts karyotyping:
- 46XX: Premature ovarian failure, resistant ovary syndrome, or gonadal agenesis.
- 46XY: Gonadal agenesis or testicular enzymatic failure.
- Short stature with low gonadotrophins suggests intracranial lesion.
- Short stature with high gonadotrophins and karyotyping usually indicates Turner syndrome or mosaic.
Management
- For hypogonadotrophic hypogonadism, treat underlying causes (e.g., weight restoration) or use hormone replacement therapy to induce secondary sexual characteristics.
- Inform patients of infertility; ovulation induction is possible later with fertility treatments.
- Hormone replacement involves oestrogen alone for 2 years, then gradual progestogen introduction over 2-3 years to mimic normal breast development.
- Avoid high oestrogen doses to prevent abnormal breast growth.
- For XY dysgenesis or enzymatic failure, perform gonadectomy to prevent malignancy.
- Consider chronic medical illnesses that delay puberty in differential diagnosis.
The document Chapter Notes: Primary amenorrhoea is a part of the NEET PG Course Gynaecology and Obstetrics.
All you need of NEET PG at this link: NEET PG
FAQs on Chapter Notes: Primary amenorrhoea
| 1. What is primary amenorrhoea and how is it defined? |  |
Ans.Primary amenorrhoea is defined as the absence of menstruation in a female by the age of 16 years, or the absence of secondary sexual characteristics by the age of 14 years. It indicates that the menstrual cycle has not begun, which can be due to various underlying causes that may involve genetic, anatomical, or hormonal factors.
| 2. What are the common causes of primary amenorrhoea? | |
Ans.Common causes of primary amenorrhoea include genetic conditions such as Turner syndrome, anatomical abnormalities like Mullerian agenesis, and hormonal disorders such as hypogonadotropic hypogonadism. Other factors may include chronic illnesses, excessive physical activity, and nutritional deficiencies that impact the hypothalamic-pituitary-gonadal axis.
| 3. How is primary amenorrhoea evaluated in a clinical setting? | |
Ans.Evaluation of primary amenorrhoea typically involves a thorough medical history and physical examination, followed by laboratory tests such as serum hormone levels (FSH, LH, estrogen, and prolactin) and imaging studies like ultrasound to assess the reproductive anatomy. Karyotyping may also be performed to identify chromosomal abnormalities.
| 4. What management options are available for primary amenorrhoea? | |
Ans.Management of primary amenorrhoea depends on the underlying cause. Hormonal therapy may be initiated to induce menstruation in cases of hypogonadism, while surgical intervention may be necessary for anatomical abnormalities. Lifestyle modifications, such as weight management and stress reduction, may also be recommended for amenorrhoea related to excessive exercise or nutritional deficiencies.
| 5. Why is it important to address primary amenorrhoea early? | |
Ans.Addressing primary amenorrhoea early is crucial because it may be indicative of underlying health issues that can affect future fertility and overall health. Delayed diagnosis and treatment can lead to complications such as osteoporosis, psychosocial issues, and increased risk of cardiovascular diseases. Early intervention can help in managing symptoms and improving quality of life.
About this Document

4.78/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: Chapter Notes: Primary amenorrhoea for NEET PG 2026 is part of Gynaecology and Obstetrics preparation. The notes and questions for Chapter Notes: Primary amenorrhoea have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Primary amenorrhoea covers topics like and Chapter Notes: Primary amenorrhoea Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Primary amenorrhoea.
Introduction of Chapter Notes: Primary amenorrhoea in English is available as part of our Gynaecology and Obstetrics for NEET PG & Chapter Notes: Primary amenorrhoea in Hindi for Gynaecology and Obstetrics course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: Chapter Notes: Primary amenorrhoea
Description
Chapter Notes: Primary amenorrhoea of Gynaecology & Obstetrics with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET PG exam.
Information about Chapter Notes: Primary amenorrhoea
In this doc you can find the meaning of Chapter Notes: Primary amenorrhoea defined & explained in the simplest way possible. Besides explaining types of Chapter Notes: Primary amenorrhoea theory, EduRev gives you an ample number of questions to practice Chapter Notes: Primary amenorrhoea tests, examples and also practice NEET PG tests


Related Searches
pdf , ppt, Semester Notes, Objective type Questions, Chapter Notes: Primary amenorrhoea, shortcuts and tricks, past year papers, Viva Questions, Exam, study material, video lectures, Free, MCQs, Sample Paper, mock tests for examination, practice quizzes, Extra Questions, Chapter Notes: Primary amenorrhoea, Important questions, Chapter Notes: Primary amenorrhoea, Previous Year Questions with Solutions, Summary;