Chapter Notes: Benign disease of the vulva


Introduction
- Many women with vulval symptoms actually have vulval skin complaints rather than gynaecological or venereological issues. It's important for gynaecologists to understand these skin conditions well, especially since primary care doctors often refer these patients to them.
- This chapter aims to help gynaecologists accurately identify common vulval skin conditions and use simple, safe, and appropriate treatments. By doing so, they can benefit their patients and find the work rewarding.
- Some hospitals have set up combined clinics to assess and manage patients with vulval symptoms in a single appointment, saving time and costs.
- These clinics also act as important referral centers for other specialists.
- Despite improvements in open communication, many patients, including younger ones, still feel embarrassed about their vulval symptoms and delay seeking help.
- It's crucial to address this issue by adopting a gentle, open, and tactful approach, as it is not only good professional practice but also the essential first step in providing effective assistance.
History Taking
- To make the patient feel more comfortable and reduce embarrassment, start by asking about their past dermatological history.
- This includes questions about:
- Skin colour
- Sensitivity to soaps and irritants
- History of atopy, such as childhood eczema, asthma, and hay fever
- Allergies, particularly to nickel (a common allergen linked to contact dermatitis), as well as perfumes, creams, and latex
- History of psoriasis, which is characterized by scaly patches on the scalp, knees, and elbows
- Symptoms indicating seborrhoeic dermatitis, such as dandruff and rash around the nose
- Once these questions are asked, the patient is likely to feel more at ease, making it easier to discuss the current issue.
- Key questions to ask during the history taking include:
- Is the main symptom itch or pain ?
- How often does it occur?
- Have there been any noticeable skin changes?
- Are there lesions in other areas?
- Has there been any vaginal discharge. If so, what does it look like?
- What medications or other treatments have been tried, and what was the outcome?
Examination
- For a proper examination, it is essential to have good lighting, a trained chaperone, and a correctly positioned examination couch.
- While some experts use a colposcope, a 4× lens magnifying loop works just as well.
- It is recommended to take a systematic approach, beginning with a general view of the vulva, which includes the skin and hair of the mons pubis and labia majora.
- General view
- Hairs:
- Distribution and extent (e.g., alopecia areata, evidence of virilization)
- Quality and condition (e.g., colour, broken hairs from friction)
- Infestation
- Skin colour:
- Pigmentary disturbance (e.g., vitiligo, other conditions)
- Inflammation present or absent
- Skin texture:
- Abnormal thickness (e.g., lichenification or atrophy)
- Skin surface:
- Integrity
- Excoriation
- Erosions
- Palpation
- Tenderness or underlying masses (e.g., cysts) in the
- Labia minora:
- Presence or absence of developmental abnormalities
- Clitoral area:
- Hood
- Clitoris. normal size and surface
- Vestibule:
- Urethral opening
- Vaginal aperture
- Epithelial surface, colour, texture, and palpation with cotton tipped swab
- Perianal area:
- A complete examination of the vulva must include an inspection of the entire perineum, which includes the perianal skin, embryologically derived from the cloaca.
- Hairs:
Biopsy of the Vulva
- A vulvar biopsy is a simple procedure that involves taking a small sample of tissue from the vulva for examination.
- Here are the key points about the procedure:
- Local Anaesthetic: The procedure requires a local anaesthetic to numb the area.
- Outpatient Treatment: It is usually done as an outpatient treatment, meaning the patient can go home the same day.
- Duration: The procedure takes about 10 minutes to complete.
- Punch Biopsy: Punch biopsy is typically sufficient for this procedure. A dermatopunch with a diameter of 3 or 4 mm is used to collect the tissue sample.
- Site Specification: It is crucial to specify the exact site of the biopsy on the vulva because the histological findings can vary depending on the area sampled.
- Indications for Biopsy:
- Vulvar biopsy may be indicated in the following situations:
- When there is difficulty in establishing a clinical diagnosis.
- For all blistering disorders, a separate punch biopsy for immunofluorescence should be performed and placed in special transport media.
- For all pigmented lesions.
- For inflammatory lesions that do not respond as expected to anti-inflammatory drugs, to rule out neoplasia.
- For persistently erosive lesions.
Procedure
- Ten minutes before the biopsy, apply a local anesthetic cream such as lignocaine combined with prilocaine or lidocaine gel. starting from the interlabial sulcus inward. This helps to minimize the pain from the injection.
- Clean the area using diluted chlorhexidine antiseptic.
- Instill plain lidocaine (1%), with or without epinephrine, using a fine needle.
- Surgical procedure:
- Carry out a punch biopsy using a punch size of 3 or 4 mm, which is typically adequate.
- Insert the punch through the epithelial surface, ensuring it goes through to full thickness.
- Gently press the surrounding skin; this will cause the plug to pop outwards.
- Use a fine needle to retrieve the plug, being careful not to damage the overlying epithelium.
- Lift the plug and cut it off at the base with scissors.
Inflammatory Skin Diseases of the Vulva
Lichen Sclerosus
Terminology
- The terms kraurosis vulvae, leukoplakia, and leukoplastic vulvitis are outdated but were likely used for cases of lichen sclerosus, lichen planus, and cicatricial pemphigoid in the past.
- Terms like vulval dystrophy and vulval squamous cell hyperplasia are also considered unhelpful and should not be used.
Definition
- Lichen sclerosus is a damaging inflammatory condition that mainly affects the genital skin.
Aetiology
- There is increasing evidence that lichen sclerosus is an autoimmune disorder, particularly in those with a genetic predisposition.
- In one study, 44% of patients had significant auto-antibodies, 22% had a family history, and 21% had another autoimmune disease.
- Conditions like vitiligo and alopecia areata are not uncommon in vulval clinics, and myxoedema is often seen in follow-up patients.
Pathophysiology
- The autoimmune response involves lymphocytes attacking the upper dermis, leading to damage at the dermo-epidermal junction and in the dermis.
- There is liquefactive degeneration of the basal cell layer, destruction of melanocytes, and a significant increase in collagen in the upper dermis.
- This results in visible signs such as bright whitening and scarring, with the 'primary' lesion appearing as a white spot, often with follicular indentation.
- Sometimes, the epidermis thickens in response, leading to hyperkeratosis.
- This ongoing damage from the autoimmune attack and the continuous repair process may increase the risk of squamous cell carcinoma in those with lichen sclerosus.
Incidence
- Lichen sclerosus can occur in both genders, at any body site, and across all races, but it most frequently affects the genital skin of white women.
- The condition typically presents in childhood and around or after menopause.
- The true incidence is not known; prevalence estimates range from 1 in 300 to 1 in 1000 of the population.
Presentation in Childhood
- In young boys, phimosis caused by lichen sclerosus is the main reason for needing circumcision.
- In females, lichen sclerosus can affect the perianal skin, causing fissures that lead to painful defaecation and constipation.
Presentation in Adults
- Women with this condition typically experience itching, with pain or dyspareunia occurring rarely.
- It is often misdiagnosed as 'recurrent candidiasis,' leading to long delays in the correct diagnosis.
- Many patients have long histories and physical signs that develop over many years.
Clinical Findings
- Initial changes occur on the labia minora and clitoral hood, with normal skin becoming swollen and taking on a dull creamy colour.
- Similar changes may also affect the fourchette, leading to small tears.
- If not treated, inflammation can damage melanocytes and cause scarring.
- The entire perineum and genitocrural folds may appear bright white, with normal vulval structure shrinking.
- The labia minora may become flattened, and the clitoris can be obscured as the hood tightens over it.
- The skin's surface may wrinkle, leading to 'cigarette-paper scarring' and fragile blood vessels that can rupture, causing purpura and ecchymoses.
- Such symptoms can be misinterpreted as signs of sexual abuse in young girls.
- As the labia minora continue to shrink, the vaginal opening may tighten significantly, but the vaginal mucosa remains unaffected and can be used in surgical procedures.
- Every review of a patient with lichen sclerosus should include a careful examination of the skin over scarred areas to check for potential squamous cell carcinoma.
- This rare occurrence may start as persistent erosion, hyperkeratotic papule, or a firm nodule that could ulcerate or grow deeply.
- Any suspicious areas or ongoing erosions should be biopsied.
- About one-third of patients present with a thickened epidermis (Hypertrophic lichen sclerosus), which usually resolves with proper treatment, although this is where squamous cell carcinoma often develops.
- Histological Pattern of Lichen Sclerosus:
- When lichen sclerosus is linked with squamous cell carcinoma, the histological pattern shows
- Epidermal hyperplasia
- Differentiated intraepithelial neoplasia (Dysplastic changes confined to the basal layers)
Current Treatment
- The preferred treatment now is a very strong topical corticosteroid, like clobetasol propionate ointment.
- The exact treatment plan is crucial:
- Use small tubes of ointment (30 gm).
- The first tube should last for three months.
- Apply a small amount (pea-sized) at night to the vulva.
- Follow this schedule:
- Nightly for four weeks
- Every other night for four weeks
- Twice a week for four weeks
- During a review after three months, if symptoms return, the patient should use the medication for 2-3 nights in a row.
- Those who do not respond should be evaluated carefully, as they might have other conditions that are harder to treat, such as lichen planus or cicatricial pemphigoid.
- Topical Agents:
- Topical testosterone is not useful.
- Caution is needed with agents that could accelerate cancerous changes.
- The use of newer non steroidal anti-inflammatory immuno-modulating topicals, like tacrolimus and pimecrolimus, is still debated and should probably be restricted to rare cases where patients do not respond to super potent topical corticosteroids.
Extra Genital Lesions
- Lichen sclerosus is uncommon in men but can be found in 5-10% of women.
- Typical locations for lichen sclerosus lesions include:
- Upper back
- Shoulders
- Hips
- Areas under pressure
- Lichen sclerosus is classified as one of the Koebnerizing dermatoses, meaning it appears at sites of previous skin injury, such as:
- Scars
- Vaccination sites
- Areas treated with radiation Skin lesions may exhibit follicular hyperkeratotic plugs, creating a 'nutmeg grater' texture.
- After removing these plugs, noticeable follicular 'delling' becomes apparent, aiding in differentiating lichen sclerosus from other white lesions like morphoea, scleroderma, scars, or vitiligo.
Histological
- The most prominent change observed is a pale area of acellular hyaline scarring in the upper dermis.
- Beneath this scarring, there is a dense bluish band of infiltrating lymphocytes, resulting in a 'sandwich effect'.
- The epidermis above this band is flattened, with a loss of rete ridges and melanocytes; in about 30% of patients, there is overlying epidermal hyperplasia.
Incidence of Vulval Squamous Cell Carcinoma
- Vulval squamous cell carcinoma exhibits a bimodal incidence pattern.
- Younger women with vulval intraepithelial neoplasia (VIN) typically have oncogenic strains of human papillomavirus (HPV), whereas older individuals often show no evidence of HPV infection.
- There is an increased incidence of squamous cell carcinoma in patients with lichen sclerosus, but this has been previously exaggerated and does not warrant prophylactic mutilating surgery.
- In reality, the incidence is below 5%. Pathological examinations of squamous cell carcinoma specimens reveal lichen sclerosus in over 50% of cases.
Lichen Planus
- Lichen planus, often referred to as 'the blue rash,' is a skin condition characterized by small, purplish, polygonal bumps with shiny surfaces. These bumps are usually found on areas such as the inner wrists, armpits, and genital regions.
- The rash is known for its intense itchiness, comparable to the itchiness experienced with scabies.
- Diagnostic indicators of lichen planus include the presence of annular lesions and the Koebner phenomenon, where new lesions appear in areas of recent skin injury or scratching.
Aetiology
- Lichen planus is associated with immune system activity, specifically an attack by lymphocytes on basal keratinocytes at the dermoepidermal junction. However, the exact cause of this condition remains unknown.
- Unlike lichen sclerosus, lichen planus does not result in a hyaline band of dermal scarring.
- In lichen planus, a dense band of lymphocytes is found beneath the basal keratinocytes, with some keratinocytes undergoing apoptosis, leading to the formation of colloid bodies-remnants of dead cells.
- The condition also involves pigmentary incontinence, where pigment is lost from the epidermis and deposited in the dermis by pigment-laden macrophages.
- The overlying skin exhibits a characteristic 'saw-tooth' pattern, and there may be hyperkeratosis (thickening of the outer skin layer), although dysplasia (abnormal cell growth) is not present.
Pathophysiology
- Lichen planus is believed to be an autoimmune disease, where T-lymphocytes attack the basal keratinocytes. It can also be associated with other autoimmune conditions, such as Primary Biliary Sclerosis.
- Similar lichenoid changes may occur in individuals with graft-versus-host disease following a bone marrow transplant.
- Certain medications, including β blockers and gold, can trigger lichen planus.
- Some cases of lichen planus appear to be familial, and there is a potential link to the genetic marker HLA-DR1.
- Diagnostic Checklist for Lichen Planus:
- Look for intensely itchy blue papules that may develop in scratch marks, often presenting as annular lesions.
- Examine the wrists for lesions characteristic of lichen planus.
- Inspect the inner cheeks for a lace-like pattern, which is a diagnostic feature of the condition.
- Identify the primary lesion, which is a flat-topped shiny polygonal papule that may exhibit Wickham's striae (white lines on the surface).
- Note that nail changes associated with lichen planus may occur, but they are considered rare.
- Lichen planus commonly affects individuals in the age range of 25-40 years and is rare in children and the elderly population.
- The clinical setting and evolution of lichen planus typically indicate a good prognosis, with the condition lasting between 9 to 18 months. However, some individuals may experience symptoms for several years.
- Lesions associated with lichen planus can leave behind pigmented tattoos that may persist for 9 to 12 months.
- Management of Lichen Planus:
- A punch biopsy is necessary to confirm the diagnosis of lichen planus.
- Grade I super-potent topical corticosteroids, such as clobetasol propionate, are effective in treating active raised papules.
- If needed, second-line treatment options include topical immunomodulators like tacrolimus (0.1%).
Erosive Lichen Planus
- Vulvo-vaginal-gingival syndrome (also known as the syndrome of Hewitt and Pelisse) is a rare condition that leads to vulval pain due to erosions on the labia minora and vestibule.
- In this condition:
- The labia majora and surrounding skin remain unaffected.
- However, areas such as the anal, oral, and vaginal mucosa are often affected.
- Symptoms may include touch bleeding and erosions, as well as potential shortening of the vagina.
- It may present with visible milky striae at the edges.
- A vaginal examination can be very painful, so a vaginal speculum should be used.
- The underlying cause of this condition is unknown.
- Histological examination reveals an aggressive form of lichen planus.
- Biopsies may show non-specific ulceration unless samples are taken from the advancing edge of lesions.
- Genetic Link. It has been associated with HLA-DQB, 0201.
Aetiology
- Diagnostic check list:
- Severely painful vulva
- Bleeding dyspareunia (Painful intercourse)
- Vaginal discharge
- Eroded inner lips of labia minora and introitus
- Marginal milky striae
- Vaginal erosions, touch bleeding, and possibly synechiae (Adhesions)
- Gingivae (Hums) that are denuded and ulcerated
- Conjunctivae (Mucous membranes of the eyes) are spared, unlike in cicatricial pemphigoid
- Evolution
- Poor prognosis it is a chronic relapsing condition
- Often shows a poor response to treatment
- Burnt-out cases can result in significant scarring
Management
- Vulvo-vaginal-gingival syndrome is extremely challenging to manage. Regular swabs should be taken to check for treatable secondary infections, such as β haemolytic streptococcus or candida.
- Antiseptic emollient soaks can provide relief (e.g. Emulsiderm, Dermal ).
- Specific treatments target the lymphocyte attack, including the use of super-potent topical steroids (e.g. clobetasol propionate or diflucortolone 0.3%. Nerisone forte oily cream).
- These steroids can be applied generously to dissolvable seaweed dressings (e.g. Sorbsan ), directly to the vulva, or wrapped around a tampon inserted into the introitus for 15-30 minutes.
- Daily visits to a specialist dermatological nursing day care may be very beneficial.
- Newer non-steroidal treatments, such as topical tacrolimus, may help some patients but can irritate others. There are concerns that these could potentially lead to neoplastic changes.
- Administering steroids vaginally can vary in complexity, with options such as introducing cream with an applicator, using steroid suppositories, or applying steroid foams (e.g. hydrocortisone acetate foam 10% ).
- Management of vaginal synechiae and stenosis involves collaboration between gynaecologists and dermatologists, using postoperative topical or sometimes oral steroids along with dilators to prevent re-sealing.
Systemic Treatment
- Oral steroids may be attempted but often do not yield satisfactory results.
- Standard immunosuppressive treatments, including azathioprine and ciclosporin, have not shown significant effectiveness.
Eczema
- Eczema and dermatitis refer to conditions that cause inflammation of the skin. This inflammation is non-scarring and can be reversed.
- Unlike urticaria, where there is a sudden leakage of fluid leading to the formation of wheals (hives), eczema involves the accumulation of fluid in the epidermis, a condition known as spongiosis.
- In severe cases of eczema, this can result in oozing, referred to as 'wet eczema,' or the development of vesicles, known as vesicular eczema. Inflammatory cells such as lymphocytes, eosinophils, basophils, and polymorphic leukocytes infiltrate both the epidermis and dermis.
- Epidermal macrophages, especially Langerhans cells, play a crucial role in managing this inflammation.
- As a consequence, the epidermis becomes hyperproliferative and parakeratotic, leading to noticeable scaling. In moist vulval areas, this scaling can manifest as a greyish-white dulling of the normal pink color.
- Vulval eczema is a common condition that can arise in various situations, including:
- Atopic skin disease
- Seborrhoeic eczema
- Irritant dermatitis
- Contact allergic dermatitis
- Frictional eczema, such as lichen simplex chronicus
Seborrheic Dermatitis
- Seborrheic dermatitis is a condition marked by an itchy, red, and scaly rash, primarily affecting the face and scalp.
- Patients with this condition often have a prolonged history of dandruff, presenting with ill-defined red patches in seborrheic areas, including:
- Scalp
- Behind the ears
- Sideburns
- Nasolabial folds
- Scaling may also occur in other moist regions such as the chest, armpits, perineum, and groin.
- Women experiencing vulval itching may be misdiagnosed with chronic candidiasis, even in the absence of discharge.
- In subtle cases, diagnosing seborrheic dermatitis can be challenging, necessitating inspection beneath the hair in the labium majora for signs of thickened, dry, and scaly dermatitis.
- Severe instances may extend to the pubic mound and genitocrural folds.
Aetiology
- There is likely a genetic predisposition to seborrheic dermatitis in over 15% of the population, with the condition capable of arising at any age.
- It typically peaks in infancy (cradle cap) and early adulthood.
- Emerging evidence suggests a link between seborrheic dermatitis and an individual's reaction to lipophilic yeasts, particularly Malassezia furfur, which are most prevalent in oily and confined areas of the body.
Treatment
- Effective management of seborrheic dermatitis involves:
- Avoiding irritants
- Utilizing anti-inflammatories, such as soap substitutes and topical corticosteroids (grade III or II)
- Reducing the yeast population with antifungal treatments, such as imidazole topicals
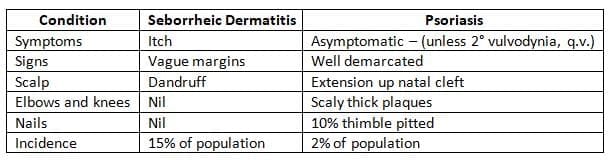
Seborrheic dermatitis versus psoriasis
- Textbook examples of different skin conditions show clear differences in physical signs, but in areas where skin folds, like the vulva, a mix of appearances can be seen.
- Chronic plaque psoriasis presents as well-defined, dry, and scaly patches on the outer surfaces of the body, such as:
- Elbows
- Knees
- Sacrum
- Scalp
- In areas where skin folds, the scales can become soft and less noticeable, but the lesions remain well-defined.
- This clear definition is an important clue for diagnosing psoriasis.
- In contrast, seborrheic dermatitis lesions blend into the surrounding normal skin without clear boundaries.
- Pure seborrheic dermatitis typically causes itching, while psoriasis may be:
- Asymptomatic (not causing any symptoms)
- Sometimes painful, especially when there are cracks (fissures)
- These fissures can extend into the natal cleft.
When faced with a red perineum, the following points may assist in distinguishing between these conditions:
 Irritant Dermatiyis
Irritant Dermatiyis
- The vulval skin is more porous and sensitive to irritants compared to skin in other areas.
- Common causes of irritant dermatitis in the vulva include:
- Bubble baths
- Disinfectants
- Deodorants
- Infective vaginal discharges
- Faeces
- Medicines, such as anti-wart treatments
- Diagnosing irritant dermatitis may be challenging, as patients might not readily share relevant history.
Treatment involves:
- Identifying and eliminating the irritant
- Using emollient soap substitutes like aqueous cream BP or Emulsiderm
- Applying a grade IV or sometimes III topical corticosteroid for a duration of 7 to 10 days
Contact Allergic Eczema
- Contact allergic eczema is often overlooked, as it is less common than in perianal skin. However, the pubic mound and labia majora can still exhibit contact dermatitis.
- Delayed (type IV) hypersensitivity is evaluated through patch tests read at 48 hours.
- Potential allergens include:
- Medicaments such as neomycin, local anaesthetics, and ethylene diamine
- Certain corticosteroids like hydrocortisone acetate and clobetasol propionate
- Rubber materials, such as those found in condoms
- Other chemicals like spermicides and perfumes
- Management of contact dermatitis involves appropriate patch testing by specialist dermatological units and avoiding the culprit allergen.
- In severe cases (Grade II), topical corticosteroids are required, while Grade I can be used for less severe cases.
- In very severe situations, systemic steroids, such as prednisolone 30 mg a day for 5 days, may be necessary.
- For acute weeping eczema, potassium permanganate soaks for a few days can be very helpful.
Allergic Contact Urticaria Of The Vulva
- Contact urticaria from latex is becoming more common, especially among healthcare workers who frequently wear rubber gloves.
- Patients often recognize the condition themselves, noticing swelling of the lips right after blowing up balloons. In these individuals, using latex condoms can lead to immediate urticarial swelling of the labia.
- Contact urticaria can also result from seminal fluid, either due to the semen itself or medications and allergens like penicillin present in the fluid.
- Specific immunotherapy targeting semen has been reported.
Lichen Simplex Chronicus
- A negative cycle can develop where scratching leads to thickened, itchy patches of skin.
- Further scratching exacerbates the condition, and a subconscious habit of scratching can form.
- This cycle can be triggered by:
- Heat (e.g., at night, after hot baths)
- Irritants (e.g., soaps, bubble baths)
- Psychological factors
- Breaking this habit is challenging, especially since patients are often unaware of their behavior.
- Common areas affected by lichen simplex chronicus include:
- Right side of the back of the neck
- Right calf
- Right labia majorum
- Right side of the scrotum
- Typically, a patient presents with pruritus vulvae and appears to have a normal vulva upon initial examination.
- However, a closer inspection of the labium majorum may reveal a characteristic lichenified, thickened, dark red, scaly patch.
- When asked to identify the worst area, the patient can usually pinpoint the lesion.
- Management involves reassuring the patient and explaining the 'itch-scratch' cycle, which often worsens during stressful periods.
- A confrontational approach is generally unhelpful. Using an emollient and short-term Grade I or II topical corticosteroids can help break the scratching habit.
- Behavioral therapy can be particularly effective in assisting individuals to stop the scratching habit.
Psoriasis
- Psoriasis is commonly associated with scaly plaques on extensor surfaces like knees, elbows, and scalp, rather than the perineum.
- However, genital psoriasis is prevalent, with a genetic predisposition in about 5% of the population and a point incidence of around 2%.
- Body psoriasis is generally not itchy, but individuals with vulval lesions may experience discomfort or pain, along with secondary vulvodynia.
- Diagnosing lesions can be challenging as the typical silvery scales may become macerated in this occluded area, appearing as inflamed, 'beefy-red' lesions.
- The edges remain well-defined, and the plaques usually have a symmetrical appearance.
- Any area in the perineum can be affected, but the vaginal mucosa is typically spared. The perianal skin may extend up the natal cleft, leading to painful fissures.
- It is important to look for corroborative lesions elsewhere. In patients with vulval symptoms, examining the scalp may reveal well-demarcated scaly plaques. Checking classical psoriatic areas such as elbows, knees, sacrum, and scalp is also crucial.
- Nails may exhibit signs of psoriasis in about 10% of patients, with symptoms like thimble pitting, sub-ungual hyperkeratosis, and onycholysis.
- However, for some individuals, genital lesions may be the only indication of psoriasis.
Etiology and Management
- The exact cause of psoriasis is unknown, although there is a genetic predisposition. Lesions can be triggered by factors such as streptococcal infection (often in guttate psoriasis) and trauma (the Koebner phenomenon).
- Histopathological examination shows significant thickening of the epidermis (acanthosis), with deep projections of the epidermal ridges into the dermis.
- Non-nuclear atypia is observed. The thickened epidermis may also exhibit patches of spongiosis with neutrophil infiltration and overlying parakeratosis.
- Dilated blood vessels in the underlying tissue, surrounded by chronic inflammatory cells, are a common finding.
- It is essential to provide a thorough explanation and reassurance about the non-infectious nature of psoriasis.
- Patients should be informed that scratching exacerbates the condition and that using emollients and soap substitutes can alleviate lesions in this warm, occluded area.
- Rarely, secondary infections such as those caused by Candida albicans may occur.
- Topical treatments for psoriasis like dithranol and calcipotriol may be too irritating for this sensitive area.
- However, other treatments such as tar, tacalcitol, calcitriol, and topical corticosteroids not stronger than Grade II (e.g., 1:4 Betnovate ointment RD with or without 5% coal tar solution) can be beneficial.
- For individuals with severe and extensive psoriasis, systemic treatments may be considered.
- These include:
- Oral methotrexate taken weekly
- Retinoids
- Ciclosporin
- It is expected that flexural areas will respond similarly to these treatments.
- However, patients should be under the care of a specialist clinic when considering such prescriptions.
- Some medications can worsen psoriasis, including:
- Lithium
- Chloroquine
- Beta blockers
- Reiter's syndrome, also known as reactive arthritis, is linked with symptoms such as:
- Uveitis (inflammation of the eye)
- Arthritis (joint inflammation)
- These symptoms are crucial for diagnosis. While circinate balanitis is commonly recognized, the related vulvitis is less common.
- Lesions associated with this condition may be:
- Eroded
- Ulcerative
- Scaly
- Histologically, the changes observed are similar to those seen in pustular psoriasis.
Pigmentary Changes of Vulval Skin
White Patches
- Vitiligo is a common autoimmune condition that leads to bright white patches on the skin due to a complete loss of pigment. These patches often appear symmetrically around the genital area.
- While vitiligo can be cosmetically concerning, especially when it affects visible areas like the face and hands, it is not harmful.
- Lichen Sclerosus can also cause white patches on the vulva, but it is different from vitiligo because it is associated with scarring and purpura (purple spots).
Dark Patches
- Post-inflammatory pigmentation is the most common cause of dark patches on the vulva. This condition usually occurs after damaging inflammation from diseases like lichen planus and, less frequently, lichen sclerosus.
- In post-inflammatory pigmentation, pigment is deposited in the dermis by macrophages, which release the pigment slowly over time.
- Larger and asymmetrical dark patches can also develop following a fixed drug eruption, and these patches can persist for many months.
- Another type of pigmentation, known as Laugier's pigmentation, is an idiopathic acquired condition that occurs without prior inflammation. This type of pigmentation is confirmed through a biopsy, which shows increased pigmentation at the basal level and pigmentary incontinence (the presence of pigment in the dermis without melanocytic proliferation).
- This indicates that the condition is benign and not harmful.
Ulcerating and Blistering (Bullous) Disorders
- These conditions typically result in pain rather than itching, and many of them are rare.
- It is important to examine other mucous membranes for indications of illness.
- In certain instances, a biopsy may be required to confirm a diagnosis, and seeking dermatological expertise is recommended.
Aphthous Ulcers
- While oral aphthous ulcers are well-recognized, their counterpart in the vulva is often neglected or mistaken for 'recurrent herpes.'
- Vulval ulcers are typically characterized by:
- Being single and round
- Having a yellowish base
- Featuring a red border
- Treating recurrent aphthous ulcers can be quite difficult.
- The following treatments can offer relief:
- Five percent Lignocaine Ointment for symptomatic relief
- Some patients may benefit from topical tetracycline
Erythema Multiforme
- Erythema multiforme is a rapid skin response that usually lasts for about two weeks.
- Some instances are confined to the mucous membranes, including the mouth, eyes, and genitals. However, these cases typically also feature small, round red spots on the hands and feet that resemble targets.
- In more severe cases, large blistering sores may form, leading to potential long-term scarring, a condition known as Stevens-Johnson Syndrome. This severe form is often seen in individuals with HIV.
- Erythema multiforme can manifest 8 to 10 days after an antigenic trigger, such as a viral infection like herpes simplex or a reaction to medication.
Management
- However, in about half of the cases, no specific cause can be identified.
- Identifying the triggering antigen is crucial.
- If necessary, long-term low-dose Aciclovir should be given to prevent recurrent infections of the herpes simplex virus.
- Both oral and ocular involvement should be evaluated and treated appropriately.
- Skin lesions can be treated with a grade I topical corticosteroid for a duration of 1 to 2 weeks.
- Short courses of systemic steroids, such as prednisolone at 40 mg daily tapered over 6 days, can help reduce fever, toxicity, and alleviate local pain.
Toxic Epidermal Necrolysis (TEN) (Lyell's Syndrome)
- TEN is a severe form of superficial reactive infarction that can result in significant skin loss and can be fatal.
- These lesions are commonly observed in patients with HIV.
- The usual trigger is a hypersensitivityto certain drugs, including:
- Non steroidal anti inflammatory drugs (NSAIDs)
- Carbamazepine
- Phenytoin
- Co-Trimoxazole
- Dapsone
- Sulpha drugs
- Management of TEN requires:
- Early diagnosis and prompt discontinuation of the triggering drug
- Rapid transfer of patients to a high-dependency treatment unit
- Previously, high-dose systemic steroids were used in treatment, but their use has been associated with higher mortality due to severe infections.
- Intravenous immunoglobulin is currently being investigated as a potential treatment option.
- Skilled nurses are necessary for managing local skin lesions, particularly in sensitive areas such as the eyes and genitals, to prevent complications like synechiae and permanent scarring.
- TEN has a high mortality rate.
- A less severe and more superficial variant of skin damage, known as Staphylococcal Scalded Skin Syndrome, is observed in children.
- This condition is caused by the exotoxin produced by staphylococcal bacteria.
Fixed Drug Eruption (FDE)
- FDE leads to irregular patches of intense inflammation on the skin and mucosal surfaces when the triggering drug is consumed.
- Patients often fail to link the rash with the medication, which can include common drugs such as codeine in pain relievers or phenolphthalein in laxatives.
- Other drugs implicated include paracetamol, non-steroidal anti-inflammatory drugs, tetracycline, griseofulvin, and cytotoxic medications.
- A challenge with the drug typically triggers a reaction at the same sites, starting within 24 hours each time.
- After healing, many patients are left with darkly pigmented patches for several months.
Management
- Diagnosis is indicated by the patient's history and physical signs, but pinpointing the specific drugs may take time.
- Hypersensitivity to these drugs is generally lifelong.
Bullous Pemphigoid
- Bullous pemphigoid is a rare autoimmune skin condition that impacts both the skin and mucous membranes, including areas like the vulva.
- While it is more commonly seen in older women, bullous pemphigoid can also occur in children.
- The disease is triggered by an antibody in the blood that attacks the dermo epidermal junction, which is the area where the outer layer of skin (epidermis) meets the underlying layer (dermis).
- Diagnosis of bullous pemphigoid can be achieved through indirect or direct immunofluorescence techniques, which help identify the presence of specific antibodies.
- There is a noted association between bullous pemphigoid and other autoimmune diseases, such as lichen sclerosus, which involves similar immune system dysregulation.
- When it comes to treatment, it is crucial to consult a dermatologist for appropriate management.
- Strong topical steroids can be very effective in controlling the condition and reducing inflammation.
- However, in many cases, systemic steroids are necessary to manage bullous pemphigoid, and these may be used in combination with cytotoxic drugs to suppress the immune response more effectively.
Cicatricial Pemphigoid
- Cicatricial pemphigoid is a rare form of pemphigoid that primarily affects the mucous membranes.
- This condition leads to scarring, particularly in areas like the vulva and conjunctivae.
- It mainly impacts older women.
- While circulating antibodies may not always be present, direct immunofluorescence from a biopsy typically yields positive results.
Pemphigus Vulgaris
- Pemphigus vulgaris is a rare and severe skin condition triggered by the immune system, resulting in the formation of blisters.
- These blisters are fragile and have a short duration, often leading to painful erosions that require medical intervention.
- The condition is most commonly seen in young adults, with a higher prevalence among Indian and Semitic populations.
- Seeking advice from a dermatologist is crucial, as treatment plans need to be tailored to individual patients.
- Typical treatments may include high-dose systemic steroids, cytotoxic medications, or mycophenolate mofetil.
Benign Familial Pemphigus (Hailey-Hailey Disease)
- This is a rare genetic disorder where friction causes skin erosions, especially in areas like the neck, armpits, and vulva.
- The diagnosis is confirmed through histological examination.
Benign Tumours of Vulval Skin
Congenital Tumours
Vascular Birthmarks
- These birthmarks are relatively common and are present at birth.
- Capillary naevi, a type of vascular birthmark, do not fade away over time.
- Typically, they do not cause any functional issues.
- Treatment options, such as laser therapy, are usually considered for cosmetic reasons rather than medical necessity.
Cavernous Haemangioma (Strawberry Naevus)
- These lesions usually manifest within the first six weeks of life and can exhibit rapid growth.
- They may occur in genital areas and, in some cases, can break down, leading to serious infections.
- Generally, these lesions resolve on their own over a period of approximately ten years, although the timeline can vary for each individual.
- Early Evaluation
- It is advisable to seek early evaluation in specialised Dermatological Laser Units when lesions present functional or cosmetic concerns.
Angiokeratomata
- Angiokeratomata are small vascular growths that are dark red or blue in color and have a thickened outer layer.
- These growths occur in approximately 2% of women.
- Similar angiokeratomata can also be found on the scrotal skin in males.
Acrochordia (Skin Tags)
- Acrochordia, commonly known as skin tags, are frequently found in areas where skin rubs against itself, including the axillae (armpits), eyelids, and groins.
- These skin tags can grow to a considerable size and may twist, leading to painful thrombosis (blood clot formation).
- Treatment for acrochordia involves scissor amputation to remove the skin tags.
Vestibular/Labial Papillomatosis
- Vestibular/labial papillomatosis is a normal variant characterized by noticeable thickening and folding of the labial skin.
- This condition can be triggered by puberty or pregnancy.
- The changes observed in vestibular/labial papillomatosis can be mistaken for an HPV infection due to the 'aceto-whitening' effect seen when 4% acetic acid is applied.
- Unlike warts, which are asymmetrical and scattered, the lesions in vestibular/labial papillomatosis can confuse biopsy results.
Keratinous Cysts
- Keratinous cysts, including closed and open comedones, are commonly found on the labia majora.
- Inflammation resembling acne (acniform inflammation) or calcification may occur in association with these cysts.
Venous Varicosities
- Venous varicosities are usually asymptomatic but may enlarge during pregnancy and shrink after childbirth.
Vestibular Mucinous Cysts
- Vestibular mucinous cysts are not uncommon in adults and can occasionally appear in adolescents.
- These cysts are harmless and do not pose any health risks.
Papillary Hidradenomata
- Papillary hidradenomata are adenomas of sweat glands with apocrine features.
- These lesions commonly occur in the ano-genital region of middle-aged white women.
- A firm, painless papule or nodule may develop on the labia majora or elsewhere in the perineum.
- In some cases, multiple lesions may be present.
- Excision of the lesions is necessary for histological confirmation of the diagnosis.
Syringomata
- Syringomata are rare tumors of eccrine ducts that are typically asymptomatic, multiple, and symmetrical.
- These tumors occur on the labia majora.
- Electro-desiccation under local anesthesia can be used to destroy syringomata.
Giant Venous Ectasia
- Giant venous ectasia is a prominent type of venous varicosity affecting the labia.
- These ectasias can dilate further during pregnancy and may pose complications during delivery.
Vulval Cutaneous Manifestations Of Underlying Systemic Disease
Crohn's Disease
- Crohn's disease can cause ulceration, fissuring, sinuses, and fistulae in the perineum.
- These perineal symptoms may occur years before the actual diagnosis of inflammatory bowel disease.
- Skin lesions in the ano-genital area are quite common in Crohn's disease, affecting up to 30% of patients.
- When these lesions are located away from the anal margin, they are referred to as 'metastatic lesions.'
- Vulval lesions in Crohn's disease often present as chronic unilateral labial oedema, with the potential for ulceration and fistulae to develop later.
- Histological examination usually shows granulomatous inflammation, but this finding is not always specific, which complicates the diagnosis.
- Hidradenitis suppurativa is characterized by bridged comedones and typical lesions found in the axillary and retro-auricular regions.
- Treatment for this condition can be challenging. Local care involving antiseptic soaks and topical steroids may provide some relief.
- However, systemic treatments are often necessary and may include oral steroids, azathioprine, or cyclosporin.
- There have been promising reports regarding the use of Infliximab as a beneficial treatment option.
Pyoderma Gangrenosum
- Pyoderma gangrenosum typically leads to the development of purulent ulcers on the shins, but lesions can also manifest on the vulva.
- The exact cause of pyoderma gangrenosum is unknown; however, lesions have the tendency to extend rapidly following surgical interventions.
- Approximately 50% of cases are associated with underlying inflammatory conditions such as rheumatoid arthritis, ulcerative colitis, or Crohn's disease.
- Histological examination reveals an inflammatory pattern that is non-specific, making the diagnosis primarily clinical.
- The condition generally responds well to systemic steroids, although other medications like dapsone or azathioprine may be required in some cases.
Behcet's Syndrome
- In the 1930s, Dr. Behçet identified a combination of symptoms including oral and genital ulcers along with ocular uveitis.
- Behcet's syndrome can impact various body systems, and the criteria for diagnosis have been updated over time.
- To diagnose this condition, recurrent oral ulcers are essential and must be accompanied by two of the following:
- Recurrent genital ulceration
- Eye lesions
- Cutaneous (skin) lesions
- A positive pathergy test (a skin reaction)
- The exact cause of Behçet's syndrome may be viral, and the formation of lesions is likely related to vascular factors.
- In certain regions, there is a link between the syndrome and a genetic marker called HLA-B5.
- Typically, the onset of Behçet's syndrome occurs before the age of fifty.
- Oral ulcers in this condition resemble recurrent aphthous ulcers.
- Vulval ulcers commonly occur on the labia minora, are persistent, recurrent, painful, and have the potential to cause scarring.
- Cutaneous (skin) manifestations may involve sterile pustules following trauma (pathergy) or pyodermatous plaques and erythema nodosum.
- Histological examination may show non-specific ulceration, but in some cases, thrombosed arterioles (clotted small blood vessels) may be observed beneath the lesions.
- The primary goal of treatment is to prevent progression to blindness and neurological complications.
- Vulval ulcers may improve with the use of topical tetracycline and corticosteroids.
- Severe cases of ulceration that do not respond to other treatments often heal with low doses of thalidomide, although this medication is challenging to obtain and poses serious risks if taken during pregnancy due to potential birth defects.
- Treatment can be complicated by neuropathy (nerve damage) and should be managed in specialized centers with experience in handling such cases.
- Recently, a treatment involving intralesional administration of recombinant human granulocyte/macrophage colony-stimulating factor (rhGM-CSF) has shown promise in healing large ulcers.
Necrolytic Migratory Erythema (Glucagonoma Syndrome)
- Necrolytic migratory erythema is a very rare condition characterized by a unique migrating skin rash, particularly around the mouth and genital area. This rash is linked to a type of pancreatic tumor called glucagonoma.
- Severe lesions are usually found in the perineum, with some occurring around the mouth. Patients with this condition often experience glossitis, which is inflammation of the tongue, and they commonly have diabetes.
- Diagnosis of necrolytic migratory erythema is made by measuring glucagon levels in the blood. This condition most often affects middle-aged women, but the exact connection between pancreatic function and skin symptoms is still not fully understood. Possible underlying causes include a deficiency of amino acids, fatty acids, and zinc.
- Necrolytic migratory erythema is primarily seen in middle-aged adults.
- It manifests as red, eroded, vesicular, and pustular lesions mainly affecting the genital area and around the mouth.
- A deficiency of zinc is the main cause of this condition, and lesions tend to heal rapidly when zinc is provided.
- Zinc deficiencies can result from inherited defects or acquired conditions, such as:
- Total parenteral nutrition
- Prematurity
- Gut bypass surgery
- Penicillamine treatment for Wilson's disease
Acanthosis Nigricans
- Acanthosis nigricans is a condition that can affect individuals who are obese, regardless of whether they have insulin resistance or not.
- This condition is thought to be caused by a growth hormone-like effect on the skin.
- Acanthosis nigricans is characterized by the appearance of smooth, velvety, brown, and thickened skin that is symmetrical.
- The skin changes typically start from the labia majora and spread to the groins and around the anus.
- Similar lesions can also be found in the axillae (armpit area).
- In some cases, there may be skin tags present along with these changes.
- Acanthosis nigricans is rarely observed in individuals who are thin.
- While this condition can be associated with underlying malignancies in some cases, not everyone with Acanthosis nigricans has cancer.
Understanding Vulvodynia and Vestibulodynia
- Over the past decade, there has been extensive discussion and analysis regarding various pain syndromes, including vulvodynia and vestibulodynia.
- General practitioners, specialists, and patients have often been puzzled by the presence of severe discomfort in these conditions, despite the absence of visible or microscopic abnormalities.
- Neurologists and pain specialists have made significant contributions to the understanding of these pain syndromes, which are named based on the affected area, such as glossodynia (mouth), anodynia (perianal), vulvodynia (vulva), and vestibulodynia (vulval vestibule).
- The perception of touch and pain involves intricate neurological pathways that originate from skin receptors, travel through sensory nerves and spinal ganglia, and reach central pain processing areas in the brain.
- These pathways can be influenced by emotional factors, such as the fear of pain, which can exacerbate the experience of discomfort.
- Although the pain experienced by patients is genuine, identifying its cause and finding effective relief can be challenging.
- Patients without clear pathological findings typically fall into two categories:
- Older women who are not sexually active often report severe, intermittent symptoms described as burning or aching sensations. They may struggle to sit on hard surfaces for extended periods. During examinations with cotton buds, tenderness is usually not observed. This group is referred to as experiencing dysaesthetic vulvodynia.
- Younger women frequently experience vulval pain triggered by touch, with examinations revealing tenderness in the vulval vestibule at the 5 to 7 o'clock position. These individuals may suffer from superficial dyspareunia (pain during intercourse) and difficulties using tampons, leading to the diagnosis of vestibulodynia. Some patients in both groups also report urethral pain and dysuria (painful urination), which can be mistaken for recurrent urinary tract infections, as cultures typically show no evidence of infection. These urethral symptoms are believed to be related to the same pain syndrome.
- Furthermore, experienced vulvologists have come to recognize that vulvodynia can be triggered by a previous inflammatory skin condition, such as lichen planus or psoriasis.
- This phenomenon is referred to as secondary vulvodynia.
Management
- To support patients dealing with vulvodynia and vestibulodynia, it is crucial to have experience and approach their symptoms with careful listening, gentleness, and confidence.
- Excessive diagnostic tests can be counterproductive, and unnecessary procedures like biopsies or cystoscopies may lead to increased post-operative pain. A neurological sensory explanation can be beneficial in understanding the condition.
- Topical local anesthetics, such as Lidocaine 5% ointment, can provide relief and boost patients' confidence, allowing them to maintain sexual relationships.
- Treatment often involves the use of older tricyclic antidepressants and other centrally acting medications, including Gabapentin and Carbamazepine. Amitriptyline, Imipramine, and Nortriptyline are preferred choices. It is helpful to explain to patients that these medications are used in higher doses for treating depression, but lower doses can effectively manage vulval pain.
- Patients typically start with 10 mg at night, gradually increasing the dosage by 10 mg weekly until pain relief is achieved.
- If there is no response at 90 mg, the medication should be discontinued, and an alternative should be considered.
- Once pain relief is achieved, the dosage should be maintained for 3 to 6 months before gradually tapering off.
- Patients can benefit from understanding that pain specialists use these medications to alleviate pain in various contexts, and consulting with these specialists can also be advantageous.
- Generally, younger patients tend to respond well to topical treatments alone, and over time, medications can be discontinued. Older women may require longer treatment durations.
FAQs on Chapter Notes: Benign disease of the vulva
| 1. What are the common inflammatory skin diseases of the vulva and their characteristics? |  |
| 2. What are the pigmentary changes that can occur in vulval skin? | |
| 3. What are the characteristics of ulcerating and blistering (bullous) disorders of the vulva? | |
| 4. What are some benign tumors of vulval skin that can be encountered? | |
| 5. How can vulval cutaneous manifestations indicate underlying systemic diseases? | |



