NEET PG Exam > NEET PG Notes > Gynaecology and Obstetrics > Chapter Notes: Epithelial ovarian cancer
Chapter Notes: Epithelial ovarian cancer


Introduction
- Ovarian cancer is a common type of solid tumor and is the top cause of death among gynecological cancers.
- This disease is particularly serious when it is at advanced stages, leading to frequent tumor recurrences and having a negative effect on both the quality and duration of life.
- The progression of the disease and the decline in the health of patients usually result from locoregional peritoneal dissemination rather than from visceral metastatic disease.
- This situation creates opportunities for therapy research that are not possible for some other types of cancer.
- Some patients can be completely cured, even those with advanced ovarian cancer, through multimodality therapy.
- As a result, there is significant research interest in finding ways to reduce the incidence of this disease and improve the prognosis for patients.
Aetiology, Epidemiology, and Genetics
- The risk of developing ovarian cancer in a woman's lifetime is about 1 in 48, with an incidence rate of approximately 22 cases per 100,000 individuals.
- This disease mainly affects older women, with the highest incidence occurring at around age 67.
- In the UK, there are roughly 7,000 new cases of ovarian cancer each year, leading to about 5,400 deaths.
- The overall 5-year survival rate is around 30% in most medical centres.
- Ovarian cancer is more common in northern Europe and the United States, while it is less frequent in Africa and Japan.
- The exact causes of ovarian cancer are not fully understood, but one important factor seems to be incessant ovulation.
- Large case control studies suggest that factors affecting ovulation can impact the risk of developing this cancer.
- For example:
- Using the oral contraceptive pill may lower the risk of ovarian cancer by 50%.
- Other factors include early onset of menstruation (menarche), late onset of menopause, pregnancy, childbirth, breastfeeding, infertility, and the use of drugs that stimulate ovulation (hyperovulating drugs).
- Conversely, the risk of ovarian cancer can be reduced by:
- Mechanical sterilisation and hysterectomy (removal of the uterus).
- Pelvic inflammatory disease (PID), an inflammatory condition, is associated with an increased risk of ovarian cancer.
- Chronic inflammation may play a significant role in the development of ovarian cancer, as suggested by studies on perineal dusting with talc. Additionally, factors like cytokines and outside-in signalling molecules could be important in this process.
- Endometriosis is also linked to certain types of ovarian cancer, particularly endometrioid and, to some extent, clear cell Mullerian adenocarcinomas, especially when endometriosis occurs on the ovarian surface.
- Environmental factors are crucial in the causes of ovarian cancer.
- For instance, the daughters of Japanese migrants to the United States have similar rates of ovarian cancer as the US population, which contrasts with the much lower rates observed in Japan.
- Genetic factors are important in ovarian cancer, although only 5-10% of cases are associated with an autosomal dominant syndrome Involving inherited defects in:
- BRCA1 and BRCA2 genes, which are linked to site-specific ovarian cancer and breast-ovarian cancer syndromes.
- Mismatch repair genes associated with type 2 Lynch syndrome or hereditary non-polyposis colorectal cancer (HNPCC).
- There is ongoing discussion about the relevance of these genes to non-inherited breast cancer. Furthermore, somatic methylation and other epigenetic mechanisms may contribute to the inactivation of these genes in many common cases of epithelial ovarian cancer.
- The molecular basis of sporadic ovarian cancer is being gradually uncovered, with P53 mutations being a common molecular alteration, particularly in serous ovarian cancer.
- While these mutations are significant in the disease's development, their clinical implications for diagnosis, prediction, prognosis, or treatment remain uncertain.
- K-ras mutations and PTEN disruptions are associated with clinical endometrioid ovarian cancer.
- Research using mouse models has demonstrated the progression from normal ovarian surface epithelium to endometriosis with K-ras mutation, and then to endometrioid adenocarcinomas with PTEN knockout.
- The PTEN knockout is crucial in a disrupted PI3K pathway, with common activations of PI3K and AKT pathways in ovarian cancer, presenting potential targets for treatment.
- Additionally, the activation of tyrosine kinases is frequently observed in ovarian cancer, indicating a reliance on growth factors.
- This includes members of the EGF receptor tyrosine kinase family, such as EGFR and HER2, with c-fms also often upregulated in ovarian cancer.
- Ongoing scientific advancements are expected to refine the molecular classification of ovarian cancer and enhance the understanding of therapeutic targets that could influence disease progression.
Screening and Prophylactic Oophorectomy
- Successful screening refers to an intervention that decreases mortality rates in those screened compared to those not screened.
- Presently, there is no evidence that screening either the general population or specific at-risk groups reduces mortality.
- Effective screening requires high sensitivity and specificity.
- High sensitivity improves survival chances, while high specificity reduces the risk of false positives, which can lead to unnecessary surgeries.
- The challenge lies in the rarity of ovarian cancer; to identify one case, approximately 99.6% specificity is necessary, meaning only 10% of those testing positive will actually have the disease. However, lower specificity (such as 92% for BRCA1 mutant ovarian cancer) can still provide a good positive predictive value in high-risk groups where the disease is more prevalent.
- Prophylactic oophorectomy, regardless of screening, nearly eliminates ovarian cancer in individuals with BRCA1 and BRCA2 mutations. It also significantly reduces breast cancer rates in those who have undergone this surgery compared to those who haven't (as noted in a NEJM article).
- This approach is becoming the preferred option for high-risk patients who can understand the cost-benefit balance. Typically, prophylactic bilateral salpingo-oophorectomy is performed after childbearing is complete, and hormone replacement therapy is initiated until natural menopause, around age 50 (as discussed in a JCO article by Armstrong).
- UKCTOCS Trial: This trial in the United Kingdom aims to recruit 200,000 womenat average risk for ovarian cancer.
- Participants are randomly assigned to one of three groups:
- Control Group (Group 3): Unscreened group.
- Group 1: Annual CA125 tests followed by transvaginal ultrasound if results are abnormal.
- Group 2: Annual transvaginal ultrasound followed by CA125 tests if results are abnormal.
- UKFOCSS Study: This study focuses on women at higher genetic risk, exploring the benefits of screening for 5,000 women with annual transvaginal ultrasounds alongside CA125 tests. The objectives include early detection and reducing cancer mortality.
- The practicality, effectiveness, and cost-efficiency of screening the general population for ovarian cancer remain uncertain.
- Given the clear advantages of prophylactic oophorectomy for specific groups, it is questionable whether even effective screening will match the benefits of removing ovaries after childbearing.
- Nevertheless, advancements in proteomics claim to achieve nearly 100% specificity and sensitivity for diagnosing ovarian cancer.
- If validated, this could transform screening prospects for both the general public and targeted groups.
- However, caution is advised, as the field of proteomics is currently contentious, grappling with sample quality control issues related to preanalytical (collection and storage) and analytical (daily variations in complex equipment) factors.
Clinical Presentation
- Ovarian cancer typically presents with non-specific symptoms, which can include:
- Abdominal bloating and discomfort
- Pressure symptoms such as nausea and an early feeling of fullness
- Colicky abdominal pain
- These symptoms often indicate advanced disease.
- However, there are more specific symptoms that may suggest an earlier stage of the disease, including:
- Postmenopausal bleeding, especially when associated with endometrial carcinoma
- Pelvic pressure symptoms, which can manifest as:
- Frequent urination
- Pelvic pain due to ovarian torsion or bleeding
- Rectosigmoid symptoms such as constipation or diarrhoea
- Signs of Ovarian Cancer
- Possible signs of ovarian cancer include:
- Gaseous abdominal distension
- A palpable pelvic mass
- Abnormal bowel sounds
- Presence of ascites
- Palpable abdominal masses
- Lymphadenopathy
- Pleural effusion
- An umbilical mass, known as a Sister Mary Joseph nodule
- Rarely, intra-abdominal organomegaly
- Recent research indicates that it is not only the symptoms themselves but also their frequency after onset that may be associated with a diagnosis of ovarian cancer, although this finding is based on a retrospective survey.
- Analyses of referrals by General Practitioners (GPs) show that different medical specialties respond to the reported symptoms in various ways, leading to different management pathways.
- It remains unclear whether delays in primary care affect outcomes in the management of ovarian cancer.
- There are many unknown factors, such as whether there is a specific point at which a tumour becomes inoperable, even if it was initially operable.
- Increasing awareness among women and healthcare professionals is crucial for the early referral of all stages of ovarian cancer, as this could ultimately impact survival rates.
Pathobiology of Epithelial Ovarian Cancer
- The surface of the ovaries is covered by a polarized cuboidal epithelial layer, which is connected to the peritoneal mesothelium.
- Epithelial ovarian cancer can develop from this surface, either directly or from trapped cells within inclusion cysts.
Is There an Early Ovarian Cancer Lesion?
- Unlike cervical and colorectal cancers, there are no clear early anatomical stages for ovarian cancer that would allow for screening of pre-cancerous or pre-invasive conditions.
- There is uncertainty about whether there are stages of progression, but some evidence suggests that malignant ovarian tumors can advance from the ovary's surface to stage III disease without passing through defined FIGO stages.
- This raises questions about screening methods based on anatomical features, similar to those used for breast cancer.
- Recent research indicates that some ovarian cancers may start from surface epithelial inclusion cysts. If this is confirmed and applies to most cases, it could lead to a potential way to prevent ovarian cancer by identifying a precursor lesion.
Borderline Lesions and Invasive Cancer: Evolving Concepts
- Borderline epithelial tumors of the ovary, which have a low potential for malignancy, exhibit different characteristics compared to epithelial ovarian cancer.
- One of the main distinctions of borderline tumors is their inability to invade the basement membrane.
- The conversion rate from borderline tumors to ovarian cancer is extremely low.
- These lesions typically allow for extended survival, whether they spread as a monoclonal or polyclonal process.
- There is a possibility of a biologically aggressive subgroup of borderline tumors, and research is ongoing to identify these particular traits.
- Potential characteristics of aggressive borderline tumors include histological signs of a 'proliferative state' and the presence of aneuploidy.
- In some instances, borderline tumors may progress to invasive ovarian cancer.
- It is essential to establish clear management protocols for this clinical condition.
- Notably, serous borderline tumors are associated with a significant incidence of up to 10% of new primary peritoneal carcinoma.
Pathology of Epithelial Ovarian Cancer
- Most ovarian cancers are of serous histology, resembling their origin from the fallopian tubes, and often contain psammoma bodies .
- The next most common types are endometrioid adenocarcinomas and clear cell carcinomas, while mucinous carcinomas are less frequent.
- Occasionally, there are ovarian carcinosarcomas, which are epithelial tumours with sarcomatous differentiation .
- Research indicates that clear cell and mucinous ovarian cancers are significantly less responsive to chemotherapy compared to serous and endometrioid types.
- A key aspect of histological classification is the grade of cancer, which ranges from:
- Well differentiated (Grade 1)
- Moderately differentiated (Grade 2)
- Poorly differentiated (Grade 3)
- Borderline tumours have uncertain malignant potential and are usually not classified as invasive cancers.
- This discussion will not explore these tumours further.
Patterns of Spread of Ovarian Cancer
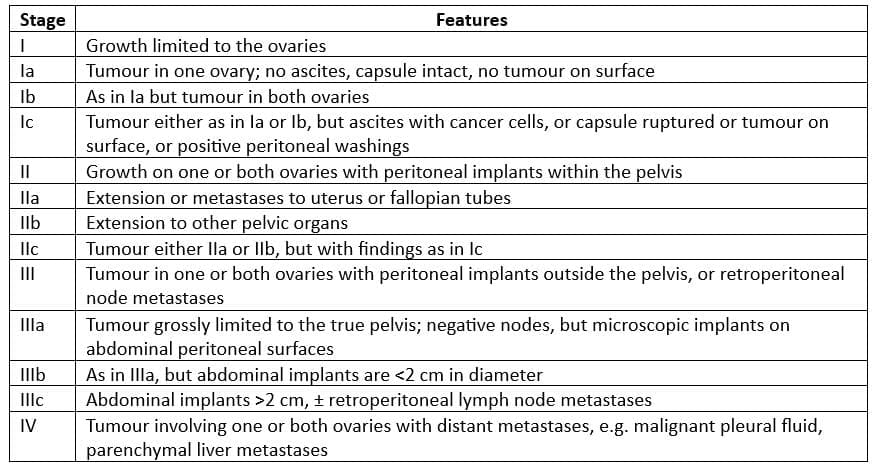
- The FIGO classification for ovarian cancer is presented and is determined through surgical staging.
- Like other types of malignant tumors, ovarian cancer can spread through local, lymphatic, and blood routes.
- There are specific patterns of spread that are typical for ovarian cancer as well as for its different histological subtypes.
- In the most common type, serous ovarian carcinomas, the main pattern of spread is through the peritoneal cavity, often leading to large amounts of disease in the abdomen.
- This usually affects the omentum and other surfaces inside the abdomen.
- Ovarian cancer may also cause malignant ascites, which is fluid buildup in the abdomen.
- Aside from malignant pleural effusion (fluid in the lungs) and spread to the umbilicus from the umbilical vein, it is rare for ovarian cancer to spread to other organs.
- Unlike other gynecological cancers, such as breast or cervical cancer, ovarian cancer usually does not cause liver, lung, brain, or bone metastases.
- However, lymph node involvement is fairly common and classifies the patient as stage IIIc.
FIGO staging for ovarian cancer
Diagnosis
- Diagnosing ovarian cancer primarily depends on histopathological methods. Large medical centres typically require detailed histopathological information to manage patients effectively.
- Key factors such as histopathological type, tumour grade, and FIGO stage are determined through sufficient biopsies.
- These biopsies may be obtained through various methods, including:
- Radiologically guided core biopsy
- Laparoscopic biopsy
- Formal staging laparotomy
- Many centres, including the West London Gynaecological Cancer Centre, consider a diagnosis based on CA125 levels, CEA levels, and cytological analysis of an ascitic sample to be insufficient for managing ovarian cancer patients.
- CA125 is a glycoprotein serum marker that is not used as a diagnostic or screening tool for ovarian cancer.
- Its levels can be elevated in various benign and malignant conditions. While CA125 is useful for prognostication approximately three months into chemotherapy, its primary purpose is to assess treatment response rather than for initiating therapy.
- It plays a role in managing relapsed cases of the disease.
Prognostic Factors
- Most patients with ovarian cancer experience a relapse and ultimately succumb to the disease.
- While the prognosis for stage I ovarian cancer is quite favorable, with earlier lower-grade stages having a cure rate exceeding 90%, the overall prognosis needs improvement.
- The survival rates for ovarian cancer are as follows:
- 1-year survival: 70%
- 2-year survival: 50%
- 5-year survival: 30%
- 10-year survival: 20%
- Research involving large cohorts of newly diagnosed patients with meticulously collected clinical data has pinpointed prognostic factors that have been validated in other clinical studies.
- The key factors predicting survival include:
- Performance status
- FIGO staging
- Tumour grade
- Surgical debulking status
- Histological subtype
- Age at diagnosis
- Albumin levels
- The variation in sample populations, particularly concerning treatment effects, has posed challenges in applying these findings to real patient groups.
- Ongoing research is now focused on whole genome molecular profiling and individual characterization of molecular targets to enhance predictive and prognostic models.
- In cases of recurrent ovarian cancer, certain factors can indicate a positive response to platinum retreatment.
- These factors include:
- Serous histology
- Disease bulk of less than 5 cm
- Number of tumour sites: Less than 3
- The traditional definition of platinum sensitivity, which closely correlates with residual disease bulk, is an interval since the last chemotherapy of greater than 6 months.
Treatment for Recently Diagnosed Ovarian Cancer
Integrated Multidisciplinary Care for Ovarian Cancer
- Ovarian cancer is most effectively treated by centralized, integrated multidisciplinary teams, which have been shown to enhance patient outcomes.
- Typically, this team includes:
- A surgical oncologist
- A non-surgical oncologist
- A radiologist
- A pathologist specializing in ovarian cancer
- A specialist nurse who offers support and communication throughout the patient's journey
- A palliative care specialist, as needed, at all stages of the disease
- Multidisciplinary teams are increasingly developing integrated care pathways that link hospital and community services within a single framework.
Surgery
- The aim of surgery is to achieve total macroscopic debulking of the tumor, which helps reduce its size before further non-surgical treatment.
- This procedure is beneficial only if the disease can be reduced to a maximum diameter of less than 2 cm, as this significantly impacts survival rates. Optimal cytoreduction varies based on surgical skill and experience.
- Studies indicate that the percentage of patients achieving optimal debulking can range widely, while still maintaining acceptable operative risks. Definitions of "optimal debulking" can differ among institutions.
- For instance, at the West London Gynaecological Cancer Centre, it is defined as a maximum size of <1 cm.
- If macroscopic debulking is deemed realistic, the surgeon typically performs a midline incision.
- After evaluation, the following procedures are carried out:
- Bilateral Salpingo-Oophorectomy: Removal of both ovaries and fallopian tubes.
- Total Abdominal Hysterectomy: Removal of the uterus along with the cervix.
- Omentectomy: Removal of the omentum, a layer of fatty tissue that may harbor cancer cells.
- Removal of All Visible Tumor Deposits: Ensuring that all visible signs of the tumor are excised.
- If total macroscopic debulking is not feasible, optimal debulking may still be achievable, depending on the circumstances.
The Importance of Surgery in Ovarian Cancer
- Historical Context: In the past, before the use of chemotherapy, patients with advanced ovarian cancer who did not undergo surgery had a survival rate of only 12-14%. This highlights the potential significance of surgery in improving outcomes.
- Retrospective Studies: Some small studies conducted in the past suggested that optimal debulking surgery might be associated with better survival rates for patients with advanced ovarian cancer.
- Key Research: Notable study by Van Den Berg and colleagues investigated the impact of interval debulking surgery in patients who initially had suboptimal debulking. The study found that those who underwent interval debulking surgery had improved survival rates, suggesting a potential benefit of surgical intervention.
- SCOTROC1 Trial: Recent important study was the surgical component of the SCOTROC1 chemotherapy trial. In this trial, all post-operative patients received carboplatin and were randomised to receive either Paclitaxel or Docetaxel, with the goal of improving progression-free survival. The surgical data from this trial allowed for comparisons between surgical practices in the United Kingdom and other countries, as the case mix and chemotherapy were the same across all centres.
- Findings from SCOTROC1: The surgical data from the SCOTROC1 trial revealed several important findings:
- Debulking Rates: The United Kingdom had lower rates of complete debulking compared to non-UK centres.
- Surgical Procedures: While similar rates of TAH BSO and omentectomy were performed in the UK, there were significantly fewer bowel resections and para-aortic/pelvic lymphadenectomies in UK patients, especially those who were optimally debulked.
- Operating Time: Operating time per patient was shorter in the UK compared to non-UK centres across all stages of the disease.
- Prognostic Factors: Residual disease greater than 2 cm was identified as an independent prognostic factor for progression-free survival, with an adverse hazard ratio of 1.6. However, the impact of residual disease depends on the extent of pre-surgical disease. In cases of less extensive disease, optimal debulking is associated with a significant survival benefit.
- UK vs. Non-UK Outcomes: UK patients who were completely debulked did not have the same level of success as those who were completely debulked in non-UK centres. However, in cases of optimal or suboptimal debulking, there was no negative impact associated with being treated in the United Kingdom.
Lymphadenectomy in Ovarian Cancer
- Lymphadenectomy, the surgical removal of lymph nodes, in the context of ovarian cancer remains a contentious issue.
- In the UK, this procedure is not commonly performed for ovarian cancer, regardless of whether it is in the early (limited) or advanced stage.
Lymphadenectomy in Early (Limited) Stage Ovarian Cancer
- There is a prevailing belief that lymphadenectomy during early-stage ovarian cancer leads to increased complications without improving patient survival rates.
- For patients with tumours that are not Grade 3, the risk of upstaging is considered to be low.
- In countries such as the United States, Australia, and parts of Europe, lymphadenectomy is usually performed as it provides better staging, although there is no demonstrated survival benefit.
- Studies like the ICON1/ACTION research indicated that all early ovarian cancer patients benefited from chemotherapy, implying that lymphadenectomy does not aid in identifying higher-risk groups.
- Chemotherapy itself carries significant risks of complications and mortality.
- Analyses of the ACTION study revealed that patients who underwent complete debulking with lymphadenectomy did not gain any advantage from chemotherapy.
- It has been proposed that patients with stage Ia and Ib disease, where lymphadenectomy confirms the staging and rules out stage IIIc, and who have Grade 1 or Grade 2 carcinoma, might be able to skip chemotherapy.
- This practice is currently being followed at the West London Gynaecological Cancer Centre.
Lymphadenectomy in Advanced Ovarian Cancer
- In the UK, lymphadenectomy for advanced ovarian cancer is not typically considered significant.
- However, recent findings from the SCOTROC1 surgical study (Crawford et al.) indicate that it could potentially impact patient outcomes, suggesting a need for further investigation in this area.
- At our center, this procedure is not routinely performed for advanced ovarian cancer unless there are clearly affected bulky lymph nodes.
Interval Debulking
- Interval debulking surgery, which involves re-operating after three cycles of chemotherapy in patients who have not been optimally debulked, has shown benefits in some studies.
- For instance, a European study demonstrated a significant survival advantage for patients undergoing this procedure, although the exact duration of the benefit was not specified.
- However, subsequent research indicated that if the initial surgery was performed by a specialist gynaecological oncologist, interval debulking may not offer any advantages.
- This discrepancy leaves the effectiveness of interval debulking surgery open to debate.
Advanced Ovarian Cancer
Front-line Chemotherapy Post-Surgery: Benefit and Toxicity:
- The approach to chemotherapy for advanced ovarian cancer is evolving, with a focus on balancing toxicity and benefit.
- There are some established facts about ovarian cancer chemotherapy that form the basis for current discussions.
- First, systemic platinum agents given after surgery are the most crucial drugs in ovarian cancer treatment, whether used alone or in combination.
- Second, carboplatin is as effective as cisplatin but has a better toxicity profile, making it a preferred option.
- Third, the combination of cisplatin with paclitaxel is superior to cisplatin with cyclophosphamide, although it may not be better than platinum-based therapy alone.
- Almost all other aspects of ovarian cancer chemotherapy are currently subjects of debate.
Carboplatin and Paclitaxel as First-Line Treatment
- For patients who are healthy, have no major other health problems (especially those that could worsen with treatment), and can handle combination chemotherapy particularly after optimal surgery the suggested treatment is carboplatin and paclitaxel.
- This recommendation comes from two important studies: the GOG111 study from 1996 and the OV10 study from 2000.
- These studies show similar survival results and clearly demonstrate that cisplatin with cyclophosphamide is less effective than cisplatin and paclitaxel. Furthermore, the AGO study in 1999 suggested that carboplatin and paclitaxel are as effective as cisplatin and paclitaxel, making carboplatin and paclitaxel the preferred option for advanced ovarian cancer.
Response Rates by Cancer Type:
- Serous and Endometrioid Ovarian Cancers: These types have high response rates (around 70-80%) with carboplatin and paclitaxel, similar to single-agent carboplatin and cisplatin.
- Mucinous and Clear-Cell Cancers: Advanced cases of these cancers have a low response to single-agent platinum, about 12-14%. However, the combination of carboplatin and paclitaxel shows a better response rate of 23-25%.
- This indicates that single-agent platinum is not an appropriate choice for patients with these rare and less favorable cancer types.
Side Effects of Carboplatin-Paclitaxel Combination Chemotherapy
- The standard treatment of carboplatin and paclitaxel comes with several significant side effects:
- Alopecia: Hair loss occurs early in treatment and is unavoidable, but it is reversible. While most patients do not retain their hair with the pre-treatment 'cold cap,' a few have reported success in doing so.
- Hypersensitivity: The hypersensitivity reaction caused by the cremaphor vehicle requires the use of dexamethasone. This can lead to substantial weight gain and may worsen diabetic control, particularly in patients with diabetes, especially during episodes of neutropenic sepsis.
- Neurotoxicity: Paclitaxel can cause peripheral nerve issues in the fingers and toes of about one-third of patients.
- While this neurotoxicity is usually mild and resolves after treatment, it can be severe in some cases and significantly impact daily activities.
- Joint-Pain Syndrome: This condition, characterized by joint pain, typically appears three days after chemotherapy and lasts for about three days. It commonly affects the small joints of the hands, knees, and feet. The pain can be severe and may require relief measures such as paracetamol or ibuprofen.
- Nausea and Neutropenic Sepsis: Nausea is a possible side effect, particularly in younger patients, although vomiting is rare. There is also a risk of neutropenic sepsis associated with this combination chemotherapy.
Single Agent Carboplatin as Front-Line Therapy
- In several countries, including those in Europe, Australasia, and North America, the standard treatment for ovarian cancer is carboplatin combined with paclitaxel.
- This treatment approach is supported by better outcomes observed in the paclitaxel and cisplatin groups in the GOG111 and OV10 studies.
- However, the control group in these studies, which received cyclophosphamide and cisplatin, had worse results compared to the single-agent platinum groups in the GOG132 and ICON3 trials.
- The GOG132 and ICON3 trials found no significant difference in outcomes between using just platinum or combining it with Taxol.
- As a result, the current NICE guidelines recommend that doctors discuss treatment options with patients, allowing them to choose between single-agent carboplatin and combination therapy.
- Many centres in the UK now consider carboplatin a standard treatment for a significant number of patients.
- At the West London Gynaecological Cancer Centre, approximately 60% of patients receive the combination of paclitaxel and carboplatin, while 40% receive only carboplatin.
Are Higher-Dose Intensity or More Cycles Better?
- Various studies have explored whether more cycles of chemotherapy (higher total dose) are better than fewer cycles with higher doses (greater dose intensity).
- Generally, these studies indicate that neither a higher total dose nor increased dose intensity offers an advantage.
- Regarding total dose, research by Bertelsen in 1993 and Lambert and colleagues in 1997 found no significant differences between different numbers of cycles.
- In terms of dose intensity, most trials comparing different intensities did not show survival differences, except for a few.
- Two randomised controlled trials of high-dose chemotherapy also found no survival difference compared to standard doses.
- However, dose density, which involves reducing the interval between chemotherapy cycles, remains a topic of interest.
- Increased dose density has been associated with improved survival in breast and cervical cancer, but its impact on ovarian cancer is still being studied.
Neoadjuvant Systemic Therapy and Primary Medical Treatment of Ovarian Cancer
- Traditionally, upfront surgery has been the gold standard for treating ovarian cancer.
- However, there is ongoing research, including the CHORUS and EORTC trials, to investigate whether neoadjuvant chemotherapy could be beneficial.
- If neoadjuvant chemotherapy does not harm survival rates, it might help by controlling the disease before surgery, potentially making the primary operation easier and more effective.
- It is crucial to approach this cautiously and wait for the results of these trials before widely adopting neoadjuvant chemotherapy.
- There are concerns that chemotherapy may be less effective in cases with a high tumour burden.
- Surgical debulking could enhance the effectiveness of chemotherapy by reducing resistant cancer cell clones and creating a more favourable environment for treatment.
Intraperitoneal Therapy
- Ovarian cancer primarily spreads within the abdominal cavity, making local control crucial for managing advanced cases. Intraperitoneal therapy has been used for over 30 years to address this issue.
- In the past decade, several randomised trials have compared intraperitoneal (IP) chemotherapy with intravenous (IV) chemotherapy, showing promising results for IP therapy.
- Meta-analyses of these trials indicate a significant reduction in hazards for IP chemotherapy, with improved median overall survival compared to IV chemotherapy.
- The GOG 172 trial reported a notable difference, with IP chemotherapy showing a median overall survival of 67 months compared to 49 months for the IV group.
- Despite its benefits, IP chemotherapy is associated with increased toxicities, including neuropathy, gastrointestinal issues, and myelotoxicity.
- Nevertheless, it is likely to become a standard option for women with optimally debulked ovarian cancer in the near future.
Treatment of Recurrent Ovarian Cancer
- Recurrent ovarian cancer is currently considered incurable, but effective chemotherapy and a comprehensive clinical approach can Improve survival rates. Key aspects of care include:
- Palliation and enhancing quality of life through effective symptom management.
- Utilizing chemotherapy, radiotherapy, and surgery.
- Integrating palliative care in both community and hospice settings.
- Aiming to limit treatment toxicity during therapy.
- The timing for restarting treatment in cases of ovarian cancer recurrence is a debated topic. This will hopefully be clarified by a crucial trial,
- MRC-OVO5, which has closed to recruitment.
- In this trial:
- Patients in complete remission with normal CA125 levels are monitored.
- When CA125 levels double the upper limit of normal, patients are randomised to either:
- Receive immediate treatment after informing the physician.
- Delay treatment until clinical symptoms appear.
- Current UK guidelines suggest not treating until symptomatic recurrence occurs, as there is no evidence that early treatment improves outcomes.
- This approach may also help maintain the quality of life for patients with asymptomatic marker recurrence. At the West London Gynaecological Cancer Centre, our policy is to delay treatment until early symptomatic progression.
- However, this requires careful monitoring, which may increase patient anxiety.
- If early symptoms progress or if there is a risk of significant anatomical damage, known as prophylactic palliation, treatment can begin. This typically involves:
- Chemotherapy, and in some cases,
- multimodal therapy that may include surgery or radiotherapy.
- Recurrent ovarian cancer can be classified as:
- Platinum refractory: Indicating a poor response to initial chemotherapy, making further standard treatments unlikely to be effective.
- Resistant or potentially sensitive.
- Patients with platinum-refractory ovarian cancer usually have an aggressive form of the disease and a poor prognosis.
- They may be considered for phase I and some phase II trials if they are sufficiently fit.
Chemotherapy
Platinum-sensitive recurrence
- Platinum-sensitive recurrence refers to the return of ovarian cancer that requires treatment more than 6 months after the last chemotherapy.
- Patients in this category may respond well to further platinum-based chemotherapy.
- The chance of a positive response increases with time:
- Over 18 months since the last treatment: up to 94% chance of response.
- Within 6 months: about 10% chance of response.
- Research by Eisenhauer and colleagues identified key factors for predicting responses to chemotherapy:
- Serous histology
- Tumour size (< 5)
- Number of disease sites
- Interestingly, the treatment-free interval did not appear significant in their findings.
- The MRC ICON4 trial studied patients relapsing over 6 months after their last chemotherapy:
- Examined the effect of adding paclitaxel to carboplatin.
- Results showed a significant improvement in survival for those with platinum-sensitive recurrent ovarian cancer.
- Hazard ratio of 0.82, with a 7% absolute survival benefit at 2 years.
- Median survival improved by 5 months.
- Paclitaxel is usually well tolerated, but caution is advised for patients with certain conditions, such as severe neuropathy or advanced diabetes.
- More studies are needed for those relapsing between 6-12 months and those who previously received paclitaxel-carboplatin.
- For patients who are platinum-sensitive but allergic, pegylated liposomal doxorubicin (Caelyx) is a viable option.
- This has shown a survival advantage over topotecan in platinum-sensitive cases.
- At the West London Gynaecological Cancer Centre, combination chemotherapy is offered to all platinum-sensitive recurrent patients unless contraindicated.
- Carboplatin monotherapy remains an effective and low-toxicity alternative.
Platinum-Resistant Recurrence
- Platinum-resistant recurrence is often defined as a return of the disease that needs treatment within 6 months after finishing the last chemotherapy.
- For patients in this category, using standard platinum treatments is unlikely to be effective, with less than 10% chance of a positive response.
- These patients tend to have similar outcomes regardless of the type of traditional chemotherapy they receive.
- Single-agent therapies have an overall response rate of 10-20%.
- Combining chemotherapy drugs at standard doses does not seem to enhance survival or response rates.
- Potential treatment options include:
- Caelyx
- Topotecan
- Oral etoposide
- Paclitaxel
- Gemcitabine
- If the cancer has strong positive estrogen and progestin receptors, it may be possible to stabilize the disease with endocrine therapy, often using tamoxifen or a progestin.
- Patients who are platinum-resistant should be considered for phase II and some phase I clinical trials.
- For those who are platinum-resistant, showing symptoms, and are in good health, the Rustin/Van der Berg regimen may be an option.
- This regimen increases the frequency and intensity of platinum doses to tackle resistance, administering 60-70 mg/m² of cisplatin weekly, which is double the usual dose of 25-33 mg/m², for six cycles over 7 weeks, alongside daily oral etoposide.
- In two studies using this regimen, platinum-resistant patients had a 46% response rate, significantly better than the 10-20% response seen with traditional single-agent therapies and much higher than the expected less than 10% response rate with standard platinum treatments.
Surgery for Recurrent Ovarian Cancer
- The role of surgery in recurrent ovarian cancer is still being debated due to a lack of sufficient evidence.
- Typically, patients with malignant bowel obstruction are not candidates for chemotherapy.
- However, they may benefit from a palliative surgical procedure to relieve the bowel obstruction, after which chemotherapy can be continued.
- In certain instances, isolated recurrences can be entirely removed through surgery, resulting in positive individual outcomes.
- The German AGO group is in the process of validating a model that predicts factors influencing the success of secondary debulking surgery.
- This evidence-based approach aims to clarify the role of surgery in cases of recurrent ovarian cancer.
- Radiotherapy is generally reserved for palliative treatment of symptomatic disease, including pelvic recurrence, cutaneous, and intracerebral disease.
Future Developments
Cytotoxic Regimes Developments
- Ongoing research is focused on developing and improving cytotoxic chemotherapy combinations for ovarian cancer.
- Recent clinical trials exploring the addition of a third drug, epirubicin, to standard regimens of paclitaxel and carboplatin have not shown any significant benefits.
- The ICON5/GOG trial is anticipated to provide insights by comparing various combination regimens, although the toxicity associated with triple therapy is substantial.
- Feasibility studies are currently investigating a treatment sequence involving four cycles of carboplatin alone, followed by a combination of paclitaxel and gemcitabine.
- There is a growing recognition of the histological heterogeneity within ovarian cancer, which plays a crucial role in treatment outcomes.
- Specific subtypes, such as clear cell and mucinous carcinomas, as well as carcinosarcoma of the ovary, have demonstrated poor response rates to standard treatments.
- In response to these challenges, the Gynaecological Cancer Intergroup (GCIG) has initiated a phase III clinical trial comparing cisplatin and irinotecan with the standard paclitaxel-carboplatin regimen in advanced clear cell carcinoma of the ovary.
- There are also plans for similar trials in advanced mucinous carcinoma of the ovary, potentially utilizing bowel cancer-type chemotherapy regimens against the standard paclitaxel-carboplatin approach.
- The encouraging outcomes from intraperitoneal therapy are expected to further our understanding of the biology and immunology of the peritoneum, paving the way for advancements in intraperitoneal chemotherapy.
Biotherapeutic Targets
- Antiangiogenic Agents: Bevacizumab, an antiangiogenic agent, is being explored as a promising treatment for ovarian cancer. A front-line trial (MRC-ICON 7) will soon test its effectiveness when combined with paclitaxel and carboplatin compared to chemotherapy alone.
- EGF Receptor Tyrosine Kinase Inhibitors: Research in lung cancer has provided insights into potential responders and survivors based on the mutation and expression status of the EGF receptor tyrosine kinase. Inhibitors like Tarceva and Iressa have shown promise in this regard.
- PTEN/AKT Pathway Manipulation: Targeting the PTEN/AKT pathway is expected to offer significant therapeutic advantages in ovarian cancer. The PI3K pathway, often disrupted in various ways across different histological subgroups and treatment states of ovarian cancer, is a key focus.
- Disruptions in PI3K Pathway:
- PTEN Disruption: Common in endometrioid and clear cell ovarian cancers.
- PI3K and AKT Activation: Frequently observed in serous carcinomas of the ovary.
- Clinical Platinum Resistance: PI3K activation is implicated in clinical platinum resistance in ovarian cancer. Therefore, inhibitors targeting PI3K, AKT, and mTOR are being considered, especially when successfully combined with chemotherapy.
- New Targeted Agents: There is an impressive range of new targeted agents available for single or combined use. The challenge lies in integrating these molecular therapies with both systemic and intraperitoneal chemotherapy in the coming years to improve the prognosis of ovarian cancer.
- Expected Improvement in Survival Rates: There is anticipation of significant improvement in survival rates, particularly for optimally debulked patients, over the next 5 to 10 years. However, it remains uncertain whether similar improvements will be observed for suboptimally debulked patients.
The document Chapter Notes: Epithelial ovarian cancer is a part of the NEET PG Course Gynaecology and Obstetrics.
All you need of NEET PG at this link: NEET PG
FAQs on Chapter Notes: Epithelial ovarian cancer
| 1. What are the early lesions associated with ovarian cancer? |  |
Ans. Early ovarian cancer lesions can include atypical hyperplasia and borderline tumors, which are characterized by abnormal cell growth that does not yet invade surrounding tissues. These lesions may not present any symptoms, making early detection challenging.
| 2. How do borderline lesions differ from invasive ovarian cancer? | |
Ans. Borderline lesions, or atypical tumors, exhibit abnormal cells but lack the invasive characteristics of cancer, meaning they do not penetrate surrounding tissue. Invasive ovarian cancer, on the other hand, shows infiltration into adjacent structures, presenting a more serious prognosis and requiring aggressive treatment.
| 3. What roles do surgery and lymphadenectomy play in the management of ovarian cancer? | |
Ans. Surgery is pivotal in the management of ovarian cancer, often involving tumor debulking to remove as much cancerous tissue as possible. Lymphadenectomy, the surgical removal of lymph nodes, is performed to assess and treat potential spread of cancer, which can be critical in determining the stage of the disease and planning further treatment.
| 4. What are the patterns of spread associated with ovarian cancer? | |
Ans. Ovarian cancer typically spreads through direct extension to surrounding organs, transcoelomic spread within the abdominal cavity, and hematogenous spread to distant sites. This multifaceted spread can complicate treatment and affect prognosis, emphasizing the need for thorough staging.
| 5. Why is integrated multidisciplinary care important for patients with ovarian cancer? | |
Ans. Integrated multidisciplinary care brings together specialists from surgery, oncology, radiology, and supportive care to provide comprehensive treatment tailored to each patient's needs. This collaborative approach can improve outcomes, enhance symptom management, and support the emotional and physical well-being of patients throughout their treatment journey.
About this Document

4.82/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: Chapter Notes: Epithelial ovarian cancer for NEET PG 2026 is part of Gynaecology and Obstetrics preparation. The notes and questions for Chapter Notes: Epithelial ovarian cancer have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Epithelial ovarian cancer covers topics like and Chapter Notes: Epithelial ovarian cancer Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Epithelial ovarian cancer.
Introduction of Chapter Notes: Epithelial ovarian cancer in English is available as part of our Gynaecology and Obstetrics for NEET PG & Chapter Notes: Epithelial ovarian cancer in Hindi for Gynaecology and Obstetrics course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: Chapter Notes: Epithelial ovarian cancer
Description
Chapter Notes: Epithelial ovarian cancer of Gynaecology & Obstetrics with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET PG exam.
Information about Chapter Notes: Epithelial ovarian cancer
In this doc you can find the meaning of Chapter Notes: Epithelial ovarian cancer defined & explained in the simplest way possible. Besides explaining types of Chapter Notes: Epithelial ovarian cancer theory, EduRev gives you an ample number of questions to practice Chapter Notes: Epithelial ovarian cancer tests, examples and also practice NEET PG tests


Related Searches
study material, pdf , ppt, Chapter Notes: Epithelial ovarian cancer, mock tests for examination, video lectures, Extra Questions, Chapter Notes: Epithelial ovarian cancer, Chapter Notes: Epithelial ovarian cancer, Viva Questions, Objective type Questions, Sample Paper, Important questions, MCQs, shortcuts and tricks, Summary, past year papers, Previous Year Questions with Solutions, practice quizzes, Free, Exam, Semester Notes;