Chapter Notes: Ethical dilemmas in obstetrics and gynaecology -1


Introduction
- Those aiming to work in Obstetrics and Gynaecology must share key qualities common to all medical professionals.
- There is a tradition of practice that relies on a solid body of knowledge.
- This body of knowledge must be regularly updated based on the best available evidence.
- Practitioners must stay informed about essential aspects of this knowledge to ensure best practice.
- It is important for practitioners to meet necessary standards of competence, care, and conduct.
- Self-motivation alone does not guarantee adequate, let alone high, standards of practice.
- A defining feature of a profession is its regulation by a governing body that all members must belong to.
- In the UK, the Royal College of Obstetricians and Gynaecologists (RCOG) plays a vital role in setting and maintaining care standards to enhance women's health.
- However, RCOG is not a regulatory authority.
- The statutory responsibility for regulation lies with the General Medical Council (GMC) in the UK, with similar organizations in other countries.
- The GMC aims to be recognized for ensuring the highest standards of medical ethics, education, and practice for the benefit of patients and the public.
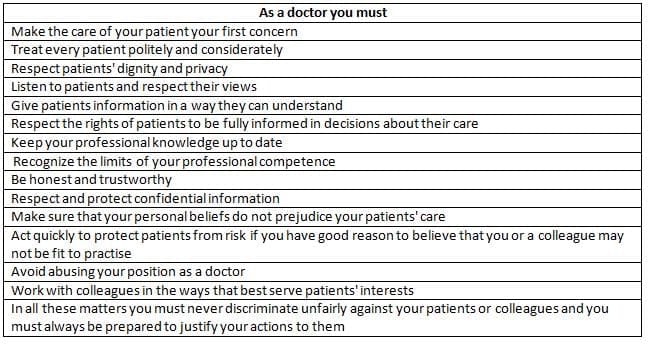
- According to the GMC's document "Duties of a Doctor," it is essential for patients to trust doctors with their lives and well-being.
- To earn this trust, the medical profession must uphold good standards of practice and care, and show respect for human life.
- The GMC outlines these duties, providing further details in the document "Good Medical Practice."
- The focus of this book is appropriately on clinical practice, with contributions from experienced authors offering the best available evidence on managing specific issues in the field.
- The authors explain what can be done and provide guidance on execution, which needs to be developed through hands-on experience.
- They typically do not dictate what should or ought to be done but will clarify what should not be done when necessary.
- The term can refers to what is factually possible, while should and ought imply obligation, with ought conveying a stronger sense of duty.
- This chapter aims to examine the ethical dimensions of obstetrics and gynaecology to enhance ethical awareness and support moral reasoning.
- It serves as a guide for thinking ethically rather than a strict rulebook dictating specific actions or thoughts.
- Duty involves moral actions, and failing to fulfill it can lead to blame.
- For instance, if a woman collapses on the antenatal ward and the on-call obstetrician does not respond without a valid reason, they would be neglecting their duty of care, resulting in moral and potential legal consequences.
- Moral actions can also be selfless and go beyond what is required, known as supererogatory actions.
- An example of this is a junior doctor who stays late to assist a colleague struggling with their workload.
- The GMC places a high importance on medical ethics over education and practice.
- Examining the "Duties of a Doctor," several terms reflect strong moral values, including honesty, trust, and respect for human life, dignity, privacy, and patient rights.
- Avoiding unfair discrimination is also crucial, highlighting that ethics is fundamental to being a doctor, especially a good one.
- This includes a firm commitment to these duties, with accountability for failing to meet them.
Duties of a doctor
The Foundation of Ethics
- Ethics, also known as moral philosophy, is the study that helps us make decisions about what is right and wrong.
- It addresses important questions such as:
- How do we know what is good?
- What is the right thing to do?
- What is justice?
- Ethics aims to provide a clear way to understand the complicated nature of moral choices.
- Morals are not just the specific beliefs or rules of different groups but also the actions that result from these beliefs.
- To better understand ethics and morals, we can compare them to DNA and the proteins that it codes for within cells.
- Ethics can be seen as a way of thinking that influences how people act in society, promoting the well-being, health, and happiness of both individuals and communities.
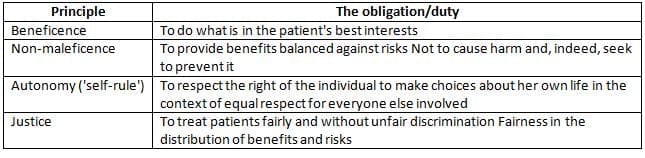
- There are essential principles of medical ethics, which are summarized in a specific table.
- People often think of ethics as simply common sense learned from experience; however, common sense is not always as common as it sounds.
- A challenge arises when trying to figure out what should be done in various situations.
- To explore this issue, we can examine a made-up clinical scenario using common sense
Case 1
- Mrs. AB, 34 years old, has been trying to get pregnant for 6 years and finally becomes pregnant with triplets through assisted conception.
- An ultrasound scan reveals that she has a serious condition called placenta praevia, and the possible effects of this condition are discussed with her.
- Both she and her husband have strong religious beliefs against receiving blood transfusions and have clearly stated in writing that she should not receive blood in any situation.
- She is admitted to the hospital for a long stay after experiencing several episodes of vaginal bleeding.
- At 34 weeks, she suffers a serious bleeding event known as antepartum haemorrhage, which is severe enough to require a Caesarean section under general anaesthetic.
- She gives her consent for the surgery but repeats her strong refusal to accept a blood transfusion, even when warned that she could die without it if the bleeding continues.
- All three babies are born in good health, but she continues to bleed after the delivery.
- The doctors explain to her husband that she might die due to her decision, and he chooses to support her wishes despite the risks involved.
- The situation raises a question: What would an ordinary person think?
- Many might say, "This couple has struggled for 6 years to start a family and has gone through assisted conception. If she dies, the three babies will be left without a mother. Surely, no one would want to die in this situation. Her refusal to accept blood seems irrational! Common sense would suggest she should receive blood!"
- Some might argue, "Let's give her the blood without telling her!"
- However, this practical approach poses a serious issue: administering a transfusion would go against her clear wishes and would legally be considered an assault.
- Thus, resolving this dilemma involves more than just common sense.
Case 1: Outcome
- You advise the hospital's legal team that there isn't enough time to take the case to court if they want to save the woman's life.
- The lawyer believes that the woman was capable of making her own decisions when she originally chose not to receive blood. He thinks that, legally, blood cannot be given to her.
- You agree with this legal perspective.
- The woman's bleeding cannot be stopped, and Mrs. AB unfortunately passes away.
- Considering this situation, was the decision made the 'right' or 'wrong' choice from an ethical standpoint?
- The late Professor Gordon Dunstan suggested that the practice of Ethics in Medicine should include:
- Good moral theories
- Clear principles that can be referred to, whether they are stated directly or implied
- Logical reasoning to create strong arguments and identify weak ones
- Skill in moral reasoning
- Careful use of language without relying on clichés
- Wisdom, which is essential above everything else
- This understanding goes beyond just common sense.
- The goal of this chapter is to help you grasp ethical theories so you can make better moral choices in clinical situations, like the one involving Mrs. AB.
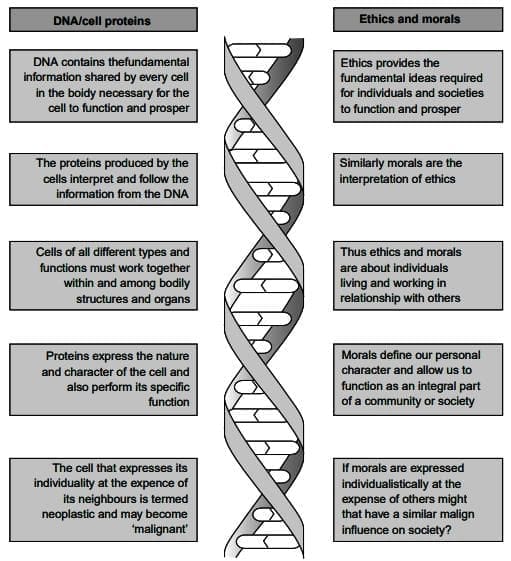
The similarities between ethics/morals and DNA/cell proteins
Diversity of Moral Theory
- Dealing with uncertainty can be tough and stressful, both in medicine and in everyday life.
- A key trait of humans is our need to make sense of uncertainty by organizing and categorizing what we believe we know.
- This need has led to many different theoretical approaches to ethics.
- It has been proposed that the variety of ethical theories is as broad as the ways we understand our connection with the environment.
- Just like sailors need maps to navigate the seas, we need frameworks to guide us through life in society.
- While principles offer important general guidance, we must also consider other aspects of a problem to move from a moral question to a moral answer.
- The two most commonly discussed systematic theories about what makes actions morally right or wrong are:
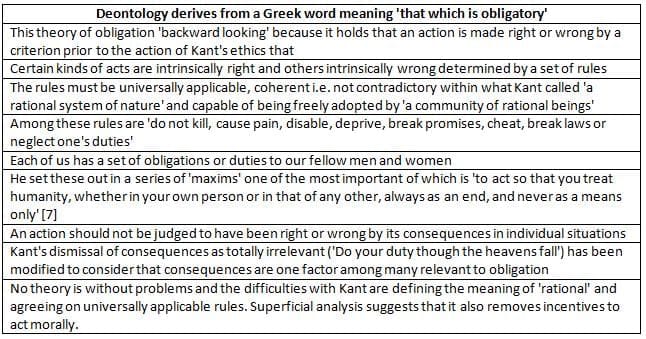
- Deontological theories (which focus on duty in actions).
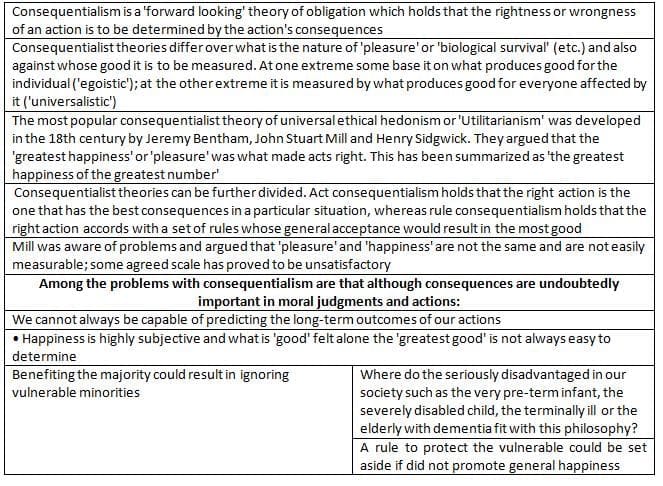
- Consequentialist theories (which emphasize the outcomes of actions).
- These theories alone are not enough to solve real-life clinical problems, leading to the development of several other perspectives to address their limitations.
Some essentials of medical ethics
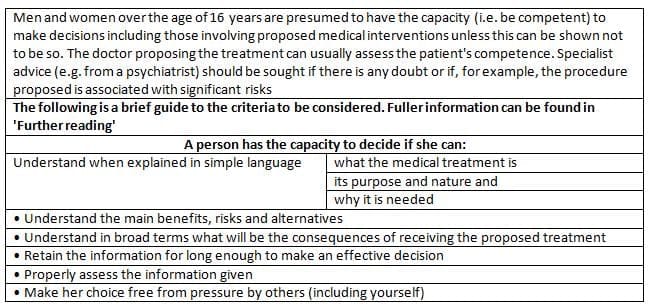
Competence a brief guide
Four Principle Approach:
- The Four Principle Approach (also known as Principlism) was created to help solve problems in Medical Ethics.
- Many of us find these principles easier to understand because the obligations linked to them are familiar in our work as obstetricians and gynecologists.
- However, these principles are sometimes used without critical thinking and are wrongly believed to provide simple solutions to all issues.
- As we look at specific clinical problems later in the chapter, we will see that these principles can often conflict with each other.
- The idea of autonomy needs more attention. Dunstan pointed out that the commonly accepted view of autonomy suggests that it gives people the right to make their own decisions about their lives without outside interference.
- There is a growing belief that this individualistic idea of autonomy is seriously flawed.
- Properly understood, medical ethics should always consider relationships and community.
- An alternative idea of patient autonomy, known as a 'principled' version, is based on moral philosophy and is thought to better fit the ideal relationship between patients and doctors.
Deontological theories or 'Duties in Action'
- In this model, patients who can make well-considered choices about their medical treatments do so in a way that takes others into account, after receiving clear and understandable information and enough time to think.
- Thus, principled autonomy suggests that individuals come to a thoughtful decision about what is best for their long-term interests while also considering the interests and autonomy of others, including healthcare providers.
- Unfortunately, there is no single theory that fits every situation.
- Sherwin suggests that different theoretical views can act as lenses, helping to clarify complex moral issues.
- Each lens can offer a better understanding of a situation, depending on the context.
Consequentialist and utilitarian theories
- Despite criticisms, the Four Principles can help analyze ethical issues if we recognize their limitations and include other perspectives, such as:
- Narrative ethics: This approach considers the context, emotions, and relationships of both the patient and clinician.
- Virtue ethics: Instead of asking, "How should I act?" it asks, "How should I live?" This approach seeks to define the qualities of character or behavior that people or groups should strive for.
- Feminist ethics: This view highlights that women have faced and continue to face oppression, which is seen as morally wrong. It aims to balance the traditionally male-centered ethics with a more female perspective, focusing on caring for individuals and ensuring respect and personal regard in ethical decisions.
The Four Principles
Making Ethical Judgements
- Medical ethics is not just about moral theories; it is about relationships and practical actions.
- Some ethical problems we encounter can be resolved fairly easily.
- However, other issues are very complicated and might not have clear solutions, leading to true dilemmas.
- This raises the question: how should we make ethical decisions in a clinical setting?
The nature of ethical judgements in medicine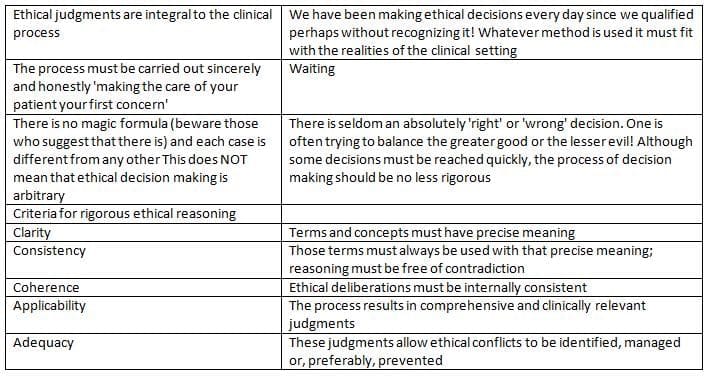
Making ethical judgements - 1: Analysis
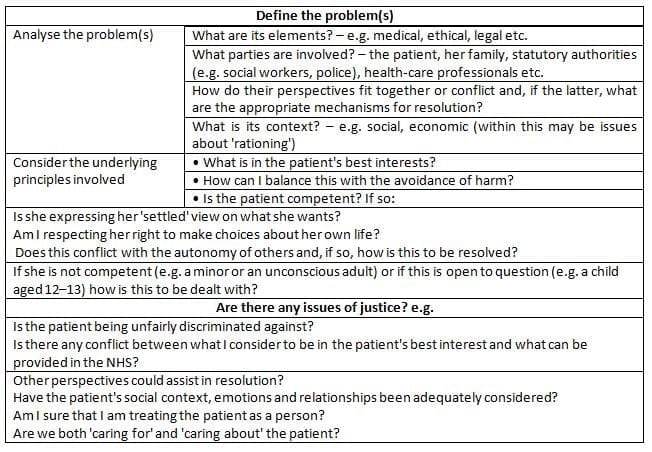
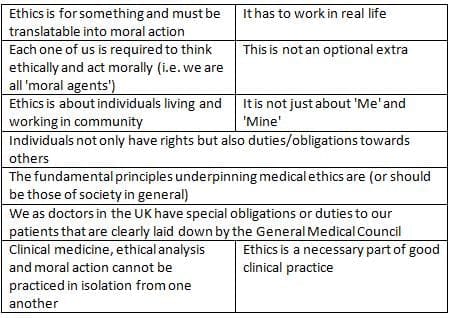
- Some important features of ethical judgments and the main criteria for thorough ethical analysis are presented in Table.
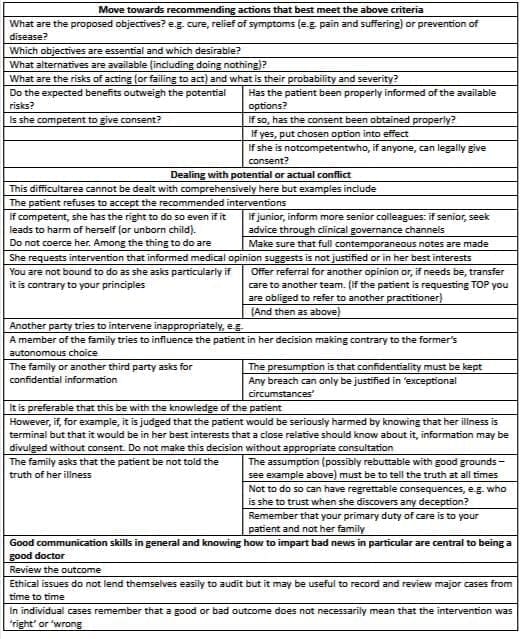
- A useful method for transitioning from ethical analysis to clinical action can be found in Tables.
- It is crucial to note that this process is not a simple mathematical task where you can just add up positives and negatives to find the right choice.
- Each situation must be addressed based on its unique context and with empathy for everyone involved.
- Some hospitals have created clinical ethics committees to help tackle particularly challenging issues, such as end-of-life decisions.
- These committees also work on developing guidelines for best practices in handling such situations.
Making ethical judgements - 2: Action
The impact of law on ethics
- The connection between ethics and the law is explored. Ethics relates to moral judgments, while the law is about public policy.
- At a basic level, the law defines what actions are allowed or not allowed to prevent legal penalties. For instance, healthcare providers must always follow the laws related to induced abortion.
- The terms "should" and "ought" in legal contexts suggest a requirement that the law can enforce.
- When these terms are used in an ethical sense, they indicate a moral duty, which is not always governed by law.
- For example, a healthcare provider not disclosing the truth about a patient's condition may not break the law, but it is often considered unethical.
- Thus, ethics covers much broader issues than the law. Ethics can help define what is "right" in terms of being "good", while the law focuses on what is allowed or forbidden.
- It can be concluded that labeling something as unethical does not automatically mean it should be illegal, and just because something is legal, it does not mean it is good ethics.
- In practice, the law often aids in making clinical decisions by providing guidelines that benefit both the patient and the clinician.
Specific Issues in Obstetrics and Gynaecology
- Reproduction is unique in medical practice due to its complexity and the potential conflict between a woman's right to make decisions about her body and the moral obligations towards unborn children.
- The diversity of moral opinions and public views on reproductive matters contributes to the ongoing ethical debates faced by obstetricians and gynaecologists.
- Some issues may never be resolved to everyone's satisfaction and will remain subjects of continuous discussion.
General Principles in Reproductive Ethics
Is there a 'Right' to Procreate?
- To address this question, it's crucial to distinguish between a negative right and a positive right.
- A negative right pertains to the freedom from interference, such as the protection against forced sterilization, which would violate an individual's right to procreate.
- Article 12 of the European Convention on Human Rights affirms that 'Men and women of marriageable age have the right to marry and found a family according to the national laws governing the exercise of this right.' This article is interpreted as a negative right, emphasizing the absence of interference in personal reproductive decisions.
- However, a question arises whether Article 12 also implies a positive right, suggesting that health services or the State should assist those who cannot conceive without assistance.
- Philosopher Warnock argues that procreation is neither an inherent right nor a universal necessity that generates a right.
- Additionally, UK courts have consistently determined that no legal obligation exists to provide such assistance, as reflected in recent legal precedents.
- The subsequent section delves into various topics that present ethical dilemmas within the realm of procreation and reproductive choices.
- While this list is not exhaustive, it aims to underscore significant issues and offer guidance for potential resolutions.
- Addressing these dilemmas should be facilitated by consulting relevant Tables that provide additional context and information.
- Most topics are accompanied by hypothetical scenarios to stimulate consideration and discussion.
- The proposed resolutions are not definitive ethical conclusions, and further reflection, as well as discussions with colleagues, are encouraged to explore different perspectives.
Contraception
Case Study 2: Providing Contraception to a Girl Under 16
- A 14-year-old girl visits a Family Planning Clinic seeking oral contraception.
- She is currently in a sexual relationship with an 18-year-old man.
- The girl wants to keep this consultation a secret from her parents and her general practitioner (GP) because she feels she cannot trust him not to inform her parents.
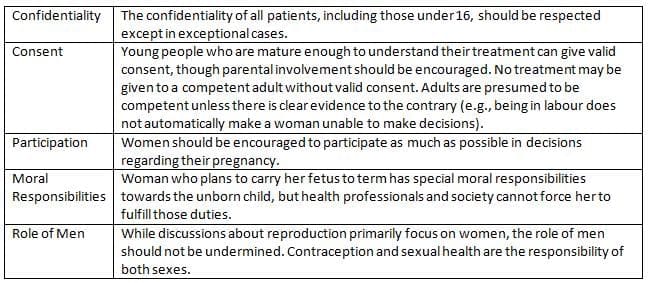
- There are important ethical considerations that affect the decision-making in this situation:
- Competence: A minor can be considered competent if the doctor believes she understands the consultation's nature and the proposed treatment after careful thought.
- Confidentiality: The girl's privacy should be respected, even if the doctor thinks parental involvement would be beneficial.
- Best Interests: The doctor's duty is to consider what would be best for the girl in this situation.
- According to a legal decision made in 1985, if the doctor judges the girl mature enough to understand her situation, her autonomy and confidentiality should be upheld.
- The doctor should encourage her to involve her parents but must keep the consultation confidential if she refuses.
- The Fraser Guidelines outline what health professionals should consider before providing contraception to young people:
- Ensure the patient understands the risks and benefits of the treatment.
- Confirm that the patient understands the advice given.
- Talk about the importance of parental support and explore why the patient might not want to inform her parents.
- Assess whether the patient is likely to engage in sexual intercourse without contraception.
- Evaluate if the patient's physical or mental health could be harmed without contraceptive advice or treatment.
- Determine if the patient's best interests require providing contraceptive advice or treatment without parental consent.
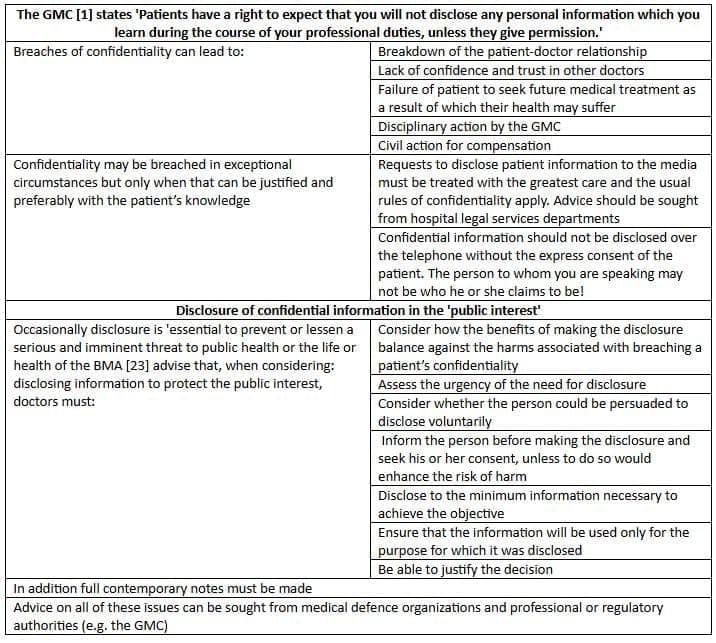
- The British Medical Association (BMA) Handbook states that even if a doctor feels the patient is not mature enough to receive contraception, they still have a general duty to maintain confidentiality unless there are serious reasons to disclose information.
- Such serious reasons might include situations involving sexual exploitation, incest, or other forms of sexual abuse.
- In these exceptional cases, the doctor has a duty to protect the patient, which might lead to breaking confidentiality, although with proper support, the patient may agree to disclose information.
- It is crucial for doctors to avoid making absolute promises about secrecy while ensuring that confidentiality is a standard principle for all consultations.
Confidentiality
Case 2: Outcome
- You assess that the benefits of prescribing an oral contraceptive pill outweigh the risks for BC.
- You strongly recommend that she discuss this with her parents, but she refuses.
- You ask for her consent to inform her GP and explain your reasons, but she declines again.
- You respect her wishes and plan to follow up with her in 6 weeks to maintain a good clinical relationship.
- You consider that your promise of confidentiality may be subject to local laws regarding mandatory reporting.
Sterilization
Case 3: Sterilization of Women with Learning Disabilities
- A GP has referred a 26-year-old woman named CS to your gynaecological clinic for possible sterilization:
- CS has severe learning difficulties and has been assessed to have the mental capacity of a 5-year-old child.
- She also has a heart condition known as atrial septal defect (ASD).
- Her mother, who is unable to care for her due to severe rheumatoid arthritis, accompanies her to the clinic.
- CS lives at home but attends a day centers for people with learning disabilities during the week.
- She has a social worker assigned to help her at the centers.
- CS is friendly and innocent but is also sexually aware.
- She has received sexual advances from other young men with similar learning difficulties at the day centers.
- Her mother is concerned about CS having intimate relationships but is also fearful that CS might get pregnant.
- CS's menstrual cycle is very irregular and her bleeding is quite heavy.
- During her periods, she becomes very agitated, making it hard for her mother to manage, including incidents of smearing blood on the walls.
- Her mother believes that sterilization could stop her periods and thus solve both issues.
- Attempts have been made to use a combined oral contraceptive pill, but CS would not take it.
- The GP also suggested a long-acting depot for contraception and managing her menstrual cycle, but CS refused the injection.
- Considerations for how to proceed include ethical and legal factors that will affect your decision.
- One important principle is that people with learning difficulties should be encouraged to make their own decisions as long as they understand the implications.
- People with learning disabilities have the right to enjoy sexual relationships in private; CS's mother does not want to take this away from her.
- The primary clinical issue to address is contraception:
- Another principle states that contraceptive services should not limit a person's autonomy more than necessary to prevent unwanted pregnancies.
- Given the previous experiences of the GP, options are limited.
- An intrauterine device (IUD) is not considered appropriate due to fitting issues and menstruation problems.
- Next, consider discussing tubal occlusion (sterilization).
- Sterilization of individuals who cannot give valid consent is a controversial issue:
- The Re F case in 1989 established legal guidelines for treating adults who cannot consent.
- The courts cannot give consent on behalf of an adult, and any treatment must be in the patient's best interest.
- This means the treatment must be necessary to save the person's life or improve their health.
- Interventions must also follow accepted medical practices and require court permission unless they are for therapeutic reasons.
- In CS's case, consider the following:
- Explain all aspects of the procedure to her mother, including the small risk of failure and that it may not solve menstrual issues.
- Evaluate if the intervention is in CS's best interest, with benefits outweighing risks.
- Reflect on whether your actions serve CS's interests or primarily those of her mother and caregivers.
Case 3: Outcome
- The consultation concludes because you need to talk to the hospital's legal department.
- Seek more details from CS's general practitioner (GP) and social worker, especially regarding any potential increased risk of CS facing sexual abuse after sterilization.
- Consider any extra risks related to her surgery due to her overall health and Autism Spectrum Disorder (ASD).
- The assessment shows that:
- Sterilization is believed to be in CS's best interests.
- Her GP states that menstruation causes CS a lot of distress, so it is also clearly in her best interests to avoid having periods.
- The social worker believes there is no increased risk of sexual abuse.
- The anaesthetist thinks that laparoscopy should not be done.
- An application is submitted to the court, and after careful review, you are allowed to proceed with the interventions that you think are best for CS.
- Following the above points, you meet with CS and her mother again to discuss the possibility of doing a subtotal hysterectomy.
- The subtotal hysterectomy is then performed without any issues.
- Was this procedure ethically justified in your opinion?
Moral Status of the Human Embryo and Fetus
- Before delving into specific issues of reproductive ethics, it is crucial to understand the moral status of the embryo and fetus.
- There are various strongly held and passionately defended views on this topic. An additional layer of complexity arises from the question of when persons come into existence.
- The term "person" is often used in ways that can be confusing, echoing Humpty Dumpty's assertion that words can mean whatever one chooses.
- While exploring the definition of a person is important, this section primarily addresses moral status directly. It also poses questions such as, "How should we treat the embryo or fetus?" and "When should the embryo or fetus be seen as a patient?"
- The main philosophical views on when the conceptus achieves significant or full moral status can be summarized as follows:
- The conceptus has full moral status from the time of fertilization.
- Full moral status is attained at various points during development or at birth.
- Moral status gradually increases throughout pregnancy.
The Conceptus Has Full Moral Status from the Time of Fertilization
- A key aspect of having full moral status is the right to life. Proponents of this view argue that moral status arises from the conceptus being fully human from the moment of fertilization.
- Finnis argues that, based on biological and philosophical criteria, fertilization marks a substantial change, and no subsequent development constitutes a real substantial change.
- This perspective suggests that from fertilization, the embryo should be treated like a fully grown human.
- While acknowledging the difficulty of equating an intelligent adult with a single-cell zygote, Finnis asserts that there is no event or principle to differentiate a typical adult, newborn, or mid-term unborn child from the one-cell zygote that began their personal history. In essence, science and philosophy agree that every living human should be regarded as a person with full moral status.
- Iglesias differentiates between developing into a person and developing as a person, arguing that there is never a stage in pregnancy when the conceptus or fetus is not a person.
- She concludes that even at the earliest developmental stage, they deserve absolute respect. While the argument may be consistent, Finnis's reliance on reason can lead to moral dilemmas in real clinical situations. Consider the following cases:
Case 4: Ectopic Pregnancy
- Mrs. FW, a 40-year-old woman who has never had children, comes to the early pregnancy unit.
- She is 8 weeks pregnant but is experiencing:
- Left-sided lower abdominal pain
- Slight vaginal bleeding
- She has been trying to have a child for 10 years and is very anxious to become a mother.
- Mrs. FW is a devout Roman Catholic.
- There is a strong suspicion of a left tubal ectopic pregnancy, which is confirmed by seeing a heartbeat in the embryo.
- You suggest performing a laparoscopy to remove the ectopic pregnancy.
- You explain the risks of the procedure, including the potential danger to her life if the fallopian tube ruptures.
- You recommend that the laparoscopy be done immediately for her safety.
- Mrs. FW asks about the chances of the pregnancy continuing successfully, and you inform her that the chances are very low.
- Despite understanding this, she worries that it would be like killing the embryo.
- According to a conservative view, both Mrs. FW and the embryo hold equal moral status.
- Even if there is a very small chance of a positive outcome, the embryo should be given a chance at life.
- The need for laparoscopy cannot be justified at this moment based on the situation.
- Most people who hold this conservative belief would still agree that the laparoscopy is in the mother's best interest.
- This situation cannot be justified by the principle of double effect.
- The only reasonable explanation is that, while the embryo has moral value, the mother's life is considered more important than that of the early embryo.
- Another scenario related to this situation will be discussed next.
The principle of double effect:
- This applies when the primary intention of one's actions is to produce a good effect but that this also contributes to or brings a bouta secondary unintended bad effect The principle permits one to perform such acts if the bad effect is:
- Truly unintended,
- Not disproportionate to the intended good effect, and Unavoidable if the good effect is to be achieved
Case 5
- In this scenario, you find yourself in a Reproductive Medicine laboratory where a fire has broken out, and there are critical decisions to make.
- You notice a container with fifty embryos meant for future transfer to a mother's uterus, but the situation is dire with smoke and flames threatening both the container and a technician who has collapsed due to smoke inhalation.
- You face an ethical dilemma: save the technician or the embryos, as time does not allow for both to be rescued.
- The moral choice seems to favor saving the technician. However, if one believes that the embryos and the technician hold equal moral value, the argument could be made to save the fifty embryos instead of one technician.
- This raises questions about the moral worth of the individuals involved in such scenarios.
- The intuitive responses to these cases suggest that the lives of the mother and the technician, respectively, hold greater moral weight than that of an early embryo.
- This aspect will be explored further, particularly in relation to the concept of potentiality.
Significant Moral Status is Gained at One of Several Points During Development or at Birth
- The idea proposed by some that moral status is linked to the development of sentience, which is the ability to feel and perceive.
- For instance, Singer argues that a conceptus lacks moral rights until brain function begins, but there is no consensus on when this occurs, with estimates ranging from 6 to 28 weeks of gestation.
- Strong suggests that while sentience is necessary for personhood, it may not be sufficient.
Self-Consciousness and Moral Status:
- The concept of self-consciousness as a criterion for full moral status is supported by thinkers like Tooley and Singer.
- They argue that moral status depends on a being's ability to reflect on its own existence. Since embryos and fetuses lack self-consciousness, they do not possess full moral status.
- Singer further contends that the moral worth of a fetus is comparable to that of a non-human animal with similar levels of rationality and self-awareness.
- This leads to the controversial implication that infants, the elderly with dementia, and patients in a persistent vegetative state may also lack moral worth due to their diminished self-consciousness.
Birth and Moral Status:
- Birth is a legally recognized milestone for personhood, but Singer challenges its moral significance, arguing that the fetus and newborn are the same entity with comparable human features and capacities, regardless of their location.
- This raises questions about the moral distinction between pre-term infants and fetuses of differing gestational ages, suggesting that location should not dictate a being's right to life.
Potential Viability and Moral Status:
- Potential viability has been proposed as a criterion for when a fetus acquires full moral status, helping to bridge the moral gap between pre-viable fetuses and post-birth infants.
- While viability is not an absolute requirement for moral standing, it is a significant factor that distinguishes fetuses from pre-viable cases.
- Similar to self-consciousness, viability may play a crucial role in determining moral standing, but fetuses can possess moral standing regardless of their viability.
Moral Status Gradually Increases Throughout Pregnancy
- Campbell et al. express the idea that biological development is a continuum, meaning it progresses gradually without clear divisions marking when full moral status is achieved.
- They argue that there is no specific moment in development, even very early on, when an embryo or fetus lacks the potential for personhood, no matter how basic that potential may be.
- This perspective grants the conceptus and fetus a degree of claim to life and respect.
- As development continues, this claim becomes stronger, especially by the third trimester, where the implications of ending a fetus's life may be similar to those of ending a life of an actual person, whether they are a child or an adult.
- Therefore, by the last trimester, the fetus should be regarded as a patient.
- This view aligns with how most people feel in real life, recognizing a distinction between the accidental loss of an embryo or early fetus and the birth of a stillborn child.
- The authors acknowledge that their potential person position does not completely satisfy either the conservative view, as it is considered too liberal, or the liberal view, as it is deemed too conservative.
- However, they believe that the gradualist approach resonates with many, based on biological, philosophical, intuitive, and practical reasons.
- This perspective can also help address the specific ethical issues discussed in this chapter.
Induced Abortion and Pregnancy Reduction
- Induced abortion is a contentious ethical issue with two opposing views: the pro-life stance, which supports the rights of the unborn, and the pro-choice stance, which advocates for the mother's right to choose.
- Both sides are often unwilling to consider each other's perspective, believing their position to be absolutely correct.
- This division oversimplifies complex moral discussions into a choice between two extremes, hindering effective clinical practice.
- Doctors must navigate their duty of care to patients while respecting their colleagues' differing values.
- The BMA Handbook of Ethics and Law presents key arguments from both sides, including a middle ground.
- When evaluating requests for pregnancy termination, it is crucial to consider various ethical factors, including:
- Compliance with laws
- The wishes of the pregnant woman
- Ethical considerations regarding the fetus
- The stage of fetal development
- Conflicting ethical views on abortion in society
Ethics and the Law on Induced Abortion
- The law specifies what is permissible but does not necessarily reflect what is morally right.
- It is crucial to determine the most ethically acceptable option in each challenging situation.
- While the law does not provide a comprehensive ethical perspective on induced abortion, it influences public opinion.
- The 1967 Abortion Act in the UK legalised abortion under certain conditions, enhancing its social acceptance despite ongoing ethical controversies.
- Legal interpretations should be carried out with ethical integrity.
- Current UK legislation prohibits termination solely based on fetal sex, except in cases of severe sex-linked disorders, which the British Medical Association deems unethical and unlawful.
Requests for Termination After 24 Weeks:
- The Abortion Act (1990) allows for termination after 24 weeks if there is a "substantial risk" of serious physical or mental abnormalities.
- However, the terms "substantial risk" and "seriously handicapped" are not clearly defined in the law, leading to ambiguity.
- For instance, the lack of clear definitions can complicate decision-making in specific cases.
FAQs on Chapter Notes: Ethical dilemmas in obstetrics and gynaecology -1
| 1. What are some common ethical dilemmas faced in obstetrics and gynaecology? |  |
| 2. How is moral status determined during pregnancy? | |
| 3. What legal considerations are involved in induced abortion? | |
| 4. What ethical issues arise when providing contraception to minors, particularly those under 16? | |
| 5. What are the ethical considerations when sterilizing women with learning difficulties? | |



