NEET PG Exam > NEET PG Notes > Gynaecology and Obstetrics > Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2
Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2

Case 6
- In this scenario, you have a pregnant woman, Ms. BN, who is 34 weeks along in her pregnancy. You request an ultrasound to assess the fetal growth, and the scan shows that the fetus is growing normally.
- However, it also reveals a left-sided talipes, commonly known as clubfoot. All other tests, including an amniocentesis for fetal karyotype, come back normal.
- You reassure Ms. BN that an isolated case of clubfoot typically has a good outcome. Despite this, she and her partner are deeply concerned and request a termination of the pregnancy. They believe that clubfoot constitutes a serious handicap and worry about the potential suffering their child might endure if surgery is necessary. They also express uncertainty about the possibility of other undiscovered issues with the baby.
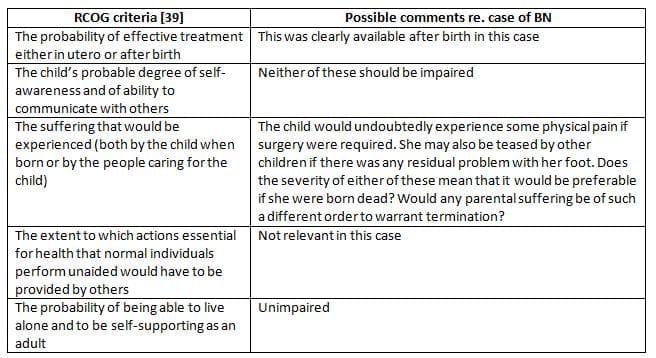
- The term "substantial" refers to something significant, important, or sizeable. In this case, the talipes is clearly visible, indicating its reality. The challenge lies in defining what constitutes "a serious handicap." While there is no legal precedent for this yet, guidance from the Royal College of Obstetricians and Gynaecologists (RCOG) provides criteria for assessing the seriousness of a handicap. These criteria suggest that terminating the pregnancy would be both morally wrong and illegal, regardless of the woman's wishes.
- Such situations, where parents consider termination due to a detected condition, are rare. When they do arise, it is advisable to consult senior colleagues and the hospital's legal department for guidance. Additionally, maintaining detailed notes of the discussions and decisions is crucial for legal and ethical transparency.
The Wishes of the Pregnant Woman
- The principle of autonomy, as discussed in the context of moral theory, involves reaching a settled view by considering what is in an individual's long-term best interests while balancing the interests of others.
- In this case, the relevant interests are those of the embryo or fetus.
- The ethical dilemma arises when there is an attempt to influence a woman to opt for a termination based on the detected condition.
Case 7
- KM is a 23-year-old woman who is unmarried and is attending an antenatal clinic at 16 weeks into her first pregnancy.
- A midwife asks her if she wants a test to check if her baby is healthy.
- Based on this question, KM has a combined test, which indicates a higher risk of Down syndrome.
- She is referred to a fetal medicine specialist for more information.
- After receiving proper counseling, KM expresses her desire to know the results, but she is against abortion.
- The tests reveal that KM is carrying a fetus with Down syndrome and a heart defect.
- Despite this, KM decides not to terminate the pregnancy.
- Her mother tries to convince her to have an abortion, believing KM cannot handle a child with disabilities and that she would have to take care of the situation.
- The mother feels that KM is being irresponsible by considering bringing such a baby into the world.
- KM is sent back to the clinic with the possibility of having an induced abortion.
- During discussions, it becomes clear that KM's feelings haven't changed, but she is worried about not receiving the support she needs from her mother.
- The first issue in this case could have been avoided with better counseling before the test.
- However, it is essential to handle the situation as it currently is, not as it could have been.
- Assume you agree with KM's mother that an abortion is the right choice for her.
- It would be unethical and illegal to force her into that decision.
- Therefore, you must support KM's choice to continue her pregnancy and help ensure she has the necessary support after the baby is born, such as referring her to a social worker.
- What about the autonomy of the woman who asks for an abortion?
- If you have taken on the role of providing counseling or support for these patients, it is crucial to inform the woman from the start that if her request meets the conditions of the Abortion Act, she will make the final decision on whether to proceed.
- Respecting her autonomy does not mean you have to agree with her choices.
Assessment of seriousness of a 'handicap'
The Ethical Demands Made on us by the Fetus and the Stage of Fetal Development
- Abortion requires careful ethical evaluation of the situations of both the woman and the fetus.
- According to Campbellet al., the level of protection given to the fetus should increase as the pregnancy moves forward.
- This aligns with the idea that the moral status of the fetus grows throughout the pregnancy.
- For example, a 28-week fetus deserves much more protection compared to a 3-day-old embryo.
- Sometimes, the interests of the mother and the fetus will clash, and it is important to create criteria that consider the welfare of both.
- In cases where there is a conflict that cannot be resolved, the argument is that decisions should be made in favor of the mother.
- Consider Case 6 again, but now the talipes (a foot deformity) was found at 20 weeks.
- This discovery could change the decision-making process significantly.
- In real situations, if BN requests a termination at 20 weeks, it is much more likely to be approved.
- The reasons for this approval cannot be based on a risk to the mother's life or a change in the criteria regarding serious handicaps.
- Instead, it would need to be justified by stating that continuing the pregnancy poses a greater risk to the physical or mental health of the pregnant woman than terminating it.
- Whether this is ethically acceptable or not, this guideline is often interpreted quite broadly, especially in the case of first trimester abortions.
- Reflect on the significant moral differences between a fetus at 20 weeks and one at 34 weeks in this scenario.
Selective Reduction of Multiple Pregnancy
- This process involves the termination of one or more fetuses before birth to increase the chances of a healthier outcome for the remaining fetus or fetuses.
- The same legal considerations apply as with ending a pregnancy with a single fetus.
- The most common reason for this procedure is in cases of high-order multiple pregnancies (like triplets or more), which have a much higher risk of perinatal death or serious disabilities.
- Therefore, it may be necessary for one or more fetuses to be lost for the sake of the survival of the others.
- This situation creates an ethical dilemma that is typically resolved through a practical approach, often by making a random choice, even if that feels unsatisfactory.
- It is generally considered unethical to choose which fetus to keep based solely on gender, except in cases where there are sex-linked disorders.
- Consider the following hypothetical example to illustrate this issue.
Case 8
- Miss TD, a 22-year-old woman, was born with a serious heart defect that required surgery to correct.
- She does not understand how serious her condition is, and her current heart health is poor, partly because she does not follow medical advice or take needed medications.
- Miss TD has no contact with her family.
- For the past three years, she has been trying very hard to become pregnant.
- She has been diagnosed with bilateral tubal occlusion caused by chronic pelvic inflammatory disease.
- Miss TD has approached multiple fertility clinics for in vitro fertilization (IVF), believing she has a right to have a child, but most have refused due to her heart condition.
- One clinic agrees to perform IVF, and they transfer three embryos (assuming this was acceptable at the time).
- All three embryos successfully implant, and she is referred to your antenatal clinic at 14 weeks with a triplet pregnancy and is close to experiencing heart failure.
- You must consider what actions to take in this situation.
- This case emphasizes the need to address the clinical situation as it exists, rather than how it could or should have been.
- You encounter several dilemmas in this case.
- Based on your opinion and the advice of a cardiologist specialized in congenital heart disease, her medical state indicates that even a single pregnancy poses risks, and continuing a triplet pregnancy significantly increases the risk of maternal death and decreases the chances of healthy outcomes for the babies.
- Your goal is to act in the best interests of Miss TD.
Case 8: (Contd)
- The cardiologist and you discuss at length the risks associated with triplet pregnancy for both her and the fetuses.
- You mention the option of reducing the pregnancy to a singleton fetus. The potential benefits and risks of this are thoroughly discussed.
- She refuses to consider the reduction.
- At 18 weeks, she is admitted with cardiac failure, and for the first time, she fully understands the seriousness of her condition.
- After treatment, her cardiac status improves, and she agrees to selective reduction.
- This procedure is performed at 20 weeks.
- Unfortunately, her membranes rupture, leading to chorio-amnionitis.
- As a result, she miscarries and develops septicaemia, requiring admission to ITU.
- Her condition is critical for several days, but she survives, although her pre-pregnancy cardiac status worsens.
- Contact is lost with her after she is discharged from hospital.
- If faced with such a case, the tragic outcome may lead you to question the validity of your advice. As noted in Show the Table a bad outcome in individual cases does not necessarily mean the intervention was 'wrong'. Given that you acted in what was believed to be in the best interests of both the patient and the randomly selected surviving fetus, selective reduction was ethically justified.
- It would be wise to conduct a detailed review of the case, particularly regarding the technique used for selective reduction. The IVF clinic should also be informed of the outcome. This will be discussed again later.
Conscientious Objection to Induced Abortion
- Doctors have the legal right to refuse participation in termination of pregnancy services.
- However, when a woman requests a termination, they must ensure she can see another doctor without delay.
Case 9
- Role: You are the clinical director of an Obstetrics and Gynaecology unit in a District General Hospital.
- Situation: Dr. SP, a senior house officer (SHO), comes to see you. She mentions that she has a conscientious objection to performing terminations of pregnancy. However, her consultant is pressuring her to help with the clerking of women being admitted for terminations and to be present during surgeries.
- Consultant's Argument: The consultant claims that SP's refusal to participate is unfair to her colleagues and insists that she must attend the theatre list as part of her training.
- Your Response: You inform the consultant that it is not appropriate to pressure SP into attending the theatre list and observing terminations.
- BMA Guidance: The British Medical Association (BMA) states that clerking a patient is considered incidental to the procedure and, thus, is not protected by the conscience clause.
- Proposed Solution: You discuss the situation with SP and suggest that she take on different tasks to help her colleagues in exchange for them handling the clerking of women admitted for termination. SP and her colleagues agree to this arrangement.
- Follow-Up Incident: Two weeks later, the Sister in the gynaecological ward informs you that SP refused to treat a woman who was bleeding after having a termination due to her conscientious objection.
- Outcome: Another SHO attended to the woman, and she did not suffer any harm.
- Your Guidance to SP: You explain to SP that neither the conscience clause nor a doctor's duty of care allows for refusing emergency treatment to a woman who has had an induced abortion.
- GMC Duties: This refusal goes against the General Medical Council's (GMC) guidelines, which state that a doctor's primary concern must be the care of the patient, and personal beliefs must not interfere with patient care.
- Consequences: You advise SP that, even though the woman was unharmed, her refusal represented a failure of her duty of care. You inform her that unless she assures you this will not happen again, she may face disciplinary action.
Assisted Reproduction
- The clinical and legal aspects of assisted reproduction have been discussed in other places, but here we will briefly touch on some important ethical issues that arise.
- The sections titled 'References' and 'Further reading' offer chances for deeper exploration of these topics.
- Significant questions include:
- Is there a right to procreate?
- What is the moral status of the human embryo/fetus?
- These questions are addressed in sections like 'Is there a "right" to procreate?' (see p. 665) and 'Moral status of the human embryo and fetus' (see p. 668).
- The BMA Handbook highlights that practices like using donated gametes or surrogacy challenge our basic ideas of personal identity, family, and the definitions of 'mother' and 'father'.
- Techniques originally created to help those with medical issues who cannot have children are now being used to give people more freedom in their reproductive choices.
- One effect of this is that some women can have children well beyond the usual age for reproduction.
- This brings back the 'can vs. ought' question raised in the 'Introduction' (see p. 658) and leads some to wonder if there are limits that society should not cross.
Who Should or Should Not be Treated Using Assisted Reproduction Techniques?
- Procreation as a Right: There is a debate about whether procreation is an essential right or a universal need that creates a right. Some argue that it is not. However, Warnock believes that those who are infertile and wish to conceive deserve medical assistance, even if they have to pay for it.
- Criteria for Treatment:Decisions about who should receive assisted reproduction treatment can be divided into clinical and non-clinical categories. Clinical decisions often have ethical implications, as illustrated by hypothetical cases like Miss TD, who received IVF despite serious health issues.
- Human Fertilisation and Embryology Act
- A woman shall not be provided with treatment services unless account has been taken of the welfare of any child who may be born as a result of the treatment (including the need of that child for a father), and of any other child who may be affected by the birth
- Principles for Treatment: The BMA suggests two general principles for deciding who should receive assisted reproduction techniques:
- Welfare of Future Child: Doctors involved in initiating a pregnancy have legal and ethical responsibilities to consider the welfare of any future child.
- This principle is part of British law under the Human Fertilisation and Embryology Act (HFEA) - 1990.
- Fair Evaluation: Every individual is entitled to a fair evaluation of their treatment request, meaning cases should be assessed individually rather than applying blanket restrictions to certain groups.
- Non-Identity Problem: The comparison between the existence of a future child and non-existence is complex. The non-identity problem, as referenced by Hope and McMillan, raises ethical questions about reproductive technology.
- Consideration of Child Welfare:. woman should not receive treatment unless the welfare of any child born from the treatment, including the need for a father, and any other child impacted by the birth have been considered.
- Potential Person Obligations: There is debate over whether obligations can be owed to a 'potential person.' While many individuals who face pain or neglect are glad to have been born, it is generally agreed that it would be wrong to create a pregnancy knowing the future child would suffer harm.
- Rare Denial of Treatment: Warnock suggests that denying treatment for non-clinical reasons should be rare, with each case evaluated on its own merits and the reasons for refusal clearly stated. Clinics should have ethics committees to guide these decisions.
- Focus on Duties and Responsibilities: In assisted reproduction, focusing solely on rights without considering duties and responsibilities is incomplete. Doctors' responsibilities are primarily towards the patient before them, but the welfare of the child born from medical intervention must also be considered.
- Respect for Fetus: The BMA suggests that the fetus merits respect but does not have absolute claims that can override those of an autonomous person, typically the mother. In assisted reproduction, the duty is owed not just to the unborn child but also to a child who has not yet been conceived.
- Responsibilities of Doctors: Doctors asked to assist in generating a pregnancy have specific responsibilities to consider the welfare of any resulting child. This duty extends to both the unborn child and the child who has not yet been conceived.
Children:
- When it comes to assisted reproduction, the child is the most vulnerable party involved.
- As a result, doctors have a greater level of responsibility and obligation in these cases compared to situations where they are managing an already existing pregnancy.
Factors for Assisted Reproduction:
- The Human Fertilisation and Embryology Authority (HFEA) provides guidance on the factors to consider when assessing individuals for assisted reproduction.
- These factors include:
- Commitment: Evaluating the individuals' commitment to having and raising a child or children.
- Stable Environment: Assessing their ability to provide a stable and supportive environment for any child resulting from the treatment.
- Medical Histories: Considering their personal and family medical histories.
- Health and Future Ability: Evaluating their health and future ability to care for and provide for a child's needs.
- Ages and Future Capability: Assessing their ages and likely future capability to care for and provide for a child's needs.
- Future Needs: Considering their future ability to meet the needs of any child or children born as a result of the treatment, including the potential for multiple births.
- Risk of Harm: Evaluating any risks of harm to the child or children, including inherited disorders, transmissible diseases, pregnancy complications, and the potential for neglect or abuse.
- Impact on Existing Children: Considering the effect of a new baby or babies on any existing children in the family.
- Making these judgments is not easy. To avoid accusations of unfair discrimination, clinics should refer cases with doubts about suitability to their ethics committee.
- Some argue that couples who conceive naturally do not face such limitations, so why should they apply to couples seeking assisted conception?
- The key difference is that in assisted reproduction, the responsibility for bringing children into the world is shared by both the parents and the healthcare professionals involved in the treatment.
- Essentially, biological parents have the right to be irresponsible, while healthcare professionals have a duty of care not to neglect that responsibility.
Gamete Donation
Case 10
- AL and MF, a 29 year old couple, come to your infertility clinic after 3 years of trying to conceive without success.
- Tests show that AL is likely fertile, but MF has azoospermia due to severe mumps orchitis in childhood.
- After counseling, they decide to proceed with donor insemination (DI).
- You discuss whether to inform any child conceived through DI about their origins, and they choose to wait and see if DI is successful first.
- The sperm donor has agreed to be identifiable.
- AL becomes pregnant, and the pregnancy goes smoothly, resulting in a healthy male infant at full term. They inform you of their decision not to tell the child about his conception.
- Their reasons are:
- 'There really isn't any need to tell him - what good will it do? The news would be too upsetting for him.'
- MF fears it may make people think he 'wasn't quite a man', leading to issues between him and 'his son'.
- The donor's identity should be protected.
- Currently, gamete donation does not raise significant ethical concerns, with the main focus on donor anonymity.
- Key arguments for removing anonymity include:
- Knowing one's genetic heritage is important for emotional and medical reasons.
- It violates Articles 8 and 14 of the Human Rights Act, which protect 'the right of respect for private and family life' and prevent 'discrimination in the enjoyment of that right'. This was a major argument for the recent change in English law.
- If adopted children can access information about their birth parents, why shouldn't those conceived by gamete donation?
- Secrecy within a family is generally harmful.
- Arguments against removing anonymity include:
- It could affect the number of donors. However, countries that have removed anonymity saw a temporary drop in numbers, replaced by altruistically motivated, older, married donors.
- It suggests there should be a relationship between the donor and any donor children.
- Consistent application of any human rights argument would require retrospective disclosure, even when anonymity was promised.
- The debate over anonymity is finely balanced. While knowing one's genetic parents may be desirable, claiming it as a fundamental right in this context is flawed.
- For instance, the human rights argument would imply that disclosure should also be retrospective, despite prior guarantees of anonymity for donors.
- Furthermore, this right would need to apply to all offspring, regardless of how they were conceived.
- This is made irrelevant by the couple's decision not to inform the child about his origins. Research shows that 70 to 80% of parents with donor insemination do not disclose this information to their children, and the couple's reasons reflect common responses.
- Therefore, involving the Human Rights Act could undermine parental discretion.
Surrogate Motherhood
- Requests for surrogacy arrangements, though rare, raise significant ethical concerns. The 1984 Committee of Inquiry into Human Fertilisation and Embryology criticized the idea of a woman using her uterus for financial profit, likening it to treating her body as an incubator for someone else's child.
- This perspective underscores the inherent dignity involved in the process.
- Furthermore, the separation of the roles of carrying and raising a child complicates both emotional and legal perceptions of motherhood. Baroness Warnock, who led the Committee, initially viewed surrogacy as a risky endeavor with potential emotional fallout.
- She now questions whether the legislation that followed her Committee's report was misguided.
- Despite rational arguments and the genuine desire of couples struggling to conceive, the intentional disruption of the intricate bond between a birth mother and her child raises profound ethical dilemmas.
- The financial motives often associated with surrogate mothers further exacerbate these concerns.
- While using family members like sisters or mothers as surrogates may eliminate the financial incentive, it introduces complex family dynamics that can be equally challenging.
- The ethical implications of surrogacy arrangements warrant careful consideration, as they navigate the delicate balance between parental aspirations and the fundamental rights and dignity of all parties involved.
Preimplantation and Prenatal Testing for Genetic or Other Reasons
- Preimplantation and prenatal testing are mainly focused on serious genetic disorders.
- Historically, prenatal testing aimed to help parents avoid having children with significant health issues, a concept that now includes preimplantation testing as well.
- Invasive testing has been avoided by many parents for less severe fetal health concerns due to associated risks.
- As these risks diminish and the scope of genetic information broadens, it is crucial to reassess the ethical foundations of prenatal testing.
- Current ethical guidelines may not fully address the increasing interest in prenatal testing for a wider range of human genes, including those unrelated to diseases or disabilities.
- The Purpose of Preimplantation and Prenatal Testing
While these subjects do not introduce new ethical dilemmas, they complicate existing ones that require our attention. - This section aims to encourage professionals in the field to take a step back and evaluate their practices.
Current Focus of Testing
- Preimplantation and prenatal testing mainly targets serious genetic disorders.
- Murray, in his 1996 book The Worth of a Child, noted that prenatal testing (and likely preimplantation testing, if he were writing today) was developed to help parents avoid having children with significant or devastating problems.
- Traditionally, the invasive nature and risks associated with prenatal testing discouraged parents from using it for anything less than severe health conditions.
- Changing Landscape of Genetic Information
- The barriers to prenatal testing are beginning to lower, leading to an expansion of genetic information available.
- It is essential to reassess the moral foundations of prenatal testing in light of this expansion.
- We must ask if our current understanding of prenatal testing ethics can help navigate the growing demand for testing across a vast range of human genes, many of which may not relate to disease or disability.
- Murray expresses concern that the answer to this question might be no.
- Future Advances in Genetic Testing
- Future developments may include:
- Fetal genetic testing using cellular or free DNA found in maternal plasma.
- Enhanced testing for the future risk of common diseases, such as diabetes, heart disease, and various cancers.
- The capability to predict non-disease traits like height, athletic ability, and potentially intelligence.
- Somatic gene transfer involves using vectors (often viruses) to introduce a human gene into the individual's cells, influencing their gene expression.This chapter briefly mentions germ line gene therapy, which transfers genes to gametes and affects all future generations.
- The ethical risks associated with germ line gene transfer are significant, making it ethically unacceptable due to potential harm to future generations.
- Currently, using viruses as vectors poses various major risks, including:
- Inadvertent incorporation of new genes into the germ line.
- Unpredictable effects on gene expression and the immune system.
- Long-term health issues resulting from the possible latency of viral vectors.
- Ethical Issues Surrounding Genetic Enhancement
- The ethical challenges related to the potential genetic enhancement of children, if gene transfer is deemed safe and effective, mirror those discussed in the quest for the perfect child.
- Murray highlights that prenatal (and now preimplantation) testing aligns with the values found in alternative reproductive technologies, making children more of a result of intentional adult decisions.
- With prenatal testing, the focus shifts towards the decision of whether to have a specific child rather than the general choice of having a child.
What Kind of Child do Parents Want?
- At a basic level, it's clear that parents want a child who is considered 'normal', which often means they prefer a child without disabilities.
- This leads to two important questions:
- First, what do the terms 'normal' and 'disability' really mean?
- Second, what role do health care professionals play in helping parents achieve this wish?
- While we can't explore these questions in depth here, we can consider two made-up situations that relate to them, which are inspired by the work of Hope and McMillan.
Case 11: Deafness in an Embryo
- A couple, EF and GM, both have a genetic condition that leads to deafness. They wish for their child to also be deaf, as they believe being deaf is not a disability but a different ability.
- After the woman becomes pregnant, they visit your clinic to request genetic testing to determine if the fetus has the gene for deafness.
- They provide information about a drug that can induce deafness in a normal fetus without harming the mother or the embryo in any other way.
- If the tests indicate that the fetus is likely to be hearing, they want you to prescribe this drug to ensure the child is deaf.
- Many people argue that causing harm to a fetus raises serious moral concerns, where harm is defined as anything that affects 'species-typical functioning.'
- In this case:
- It may be acceptable to conduct genetic testing to determine if the child will be deaf.
- However, it would be morally wrong to harm the fetus by administering the drug to induce deafness.
- Hearing is a typical human ability, and the drug would alter the child's identity.
- Now, let's consider a different scenario.
Case 12: Selecting an Embryo with Deafness
- HJ and FS are a couple who have the same genetic condition that causes deafness, similar to EF and GM.
- They visit a fertility clinic seeking help with conception and want to use preimplantation diagnosis.
- The purpose of the diagnosis is to find out if the embryos have the gene that causes deafness.
- They ask for only an embryo that has the deafness gene to be implanted, similar to the wishes of EF and GM.
- The question arises:
- Should the clinic grant their request?
- If the answer is yes, the reasoning is based on their desire to have a child with the same condition.
- If the answer is no, it might be due to ethical concerns about the identity of the fetus.
- Hope and McMillan suggest that the main difference between the two situations is that in the first case, the fetus already has an identity and could be harmed.
- In the second case, they argue that the fetus does not have an identity and, therefore, cannot be harmed.
- This idea relates to what they call the 'non-identity problem', which considers who should receive assisted reproduction techniques.
- They place great importance on parental choices regarding reproduction and believe the couple's request should be honored.
- A scenario adapted from Murray challenges their viewpoint and raises questions about their recommendation.
Case 13
- A terrorist hides a time bomb in a nursery school, intending to harm children aged three years or younger. He plans for the bomb to explode in four days.
- When caught, the bomb is found and defused.
- The terrorist is clearly morally responsible and deserves punishment.
- In a different scenario, the same terrorist hides the bomb in the nursery school but sets it to go off in four years, for reasons known only to him. He is apprehended again, and the bomb is discovered and defused. However, the children who would be there in four years have not yet been conceived.
- The question arises:
- Does the terrorist's moral responsibility change in this case?
- The answer is no. Even though the future children do not yet exist and lack identity, moral concepts and the idea of harm can still be applied to them.
- This raises important questions about the nature of moral responsibility and the potential for harm to those who have not yet been conceived.
- In Cases 11 and 12, where the outcome is the same (a child being deaf), it could be argued that creating a 'non-species typical' deaf fetus is equally justifiable in either instance.
- However, Harris argues that it is morally wrong to create a life likely to experience more suffering than other possible lives.
- The discussion is meant to provoke thought rather than provide definitive answers.
Preimplantation Genetic Diagnosis (PGD) and Saviour Siblings
- Current Allowances in the UK: PGD is permitted in the UK for specific medical purposes, including:
- Determining the sex of embryos at risk for sex-linked disorders.
- Detecting single gene defects, such as cystic fibrosis.
- Identifying chromosomal abnormalities like translocations, inversions, and deletions, although not aneuploidy.
- Ethical Justification: Experts like Robertson argue that PGD can be ethically justified for:
- Identifying genetic susceptibility to late-onset diseases.
- HLA matching for organ or stem cell transplants.
- Controversial Uses: The use of PGD for non-medical traits is contentious and should be evaluated based on parental needs and potential harm to embryos, children, and society.
- Saviour Siblings: The concept of "saviour siblings" involves using PGD to select an embryo that is a genetic match for a sick child in need of a stem cell transplant. This practice raises ethical concerns about:
- The best interests of the saviour sibling.
- The potential commodification of unborn children.
- Ethical Perspectives: Some ethicists argue that PGD for the benefit of a relative does not harm anyone and should not be restricted. They advocate for individual freedom in such medical decisions.
Case 14
- Kate develops a rare type of leukaemia when she is just 2 years old.
- She needs a bone-marrow transplant, but there is no matching donor available.
- Her parents, Brian and Sara, decide to use IVF and PGD to create an embryo that matches her HLA type exactly.
- Anna is born as a result of this process.
- Stem cells are collected from Anna's umbilical cord to help treat Kate.
- Sadly, the stem cell treatment only works for a short time.
- Over the years, Anna gives her sister bone marrow multiple times.
- While their parents love Anna for who she is, she begins to feel the weight of her role as a donor.
- Brian and Sara assume Anna will always agree to help Kate, but they never talk about it with her, which means her consent is taken for granted.
- When Kate turns 16, she needs more treatment with cytotoxic drugs, leading to kidney failure.
- The only solution for this is a kidney transplant.
- Now, Anna is 13 years old, and once again, their parents expect her to willingly donate a kidney since she is a perfect match.
- This situation raises several ethical issues.
- The story highlights that being a 'saviour sibling' involves more than just donating cord blood.
- Anna carries a heavy burden regarding whether her sister will live or die, a reality we can learn from in real life as well.
Sex Selection for Non-Medical Reasons
- In1999 Stance by the ASRM Ethics Committee of the American Society of Reproductive Medicine (ASRM) expressed concerns that using IVF for sex selection could foster gender bias and cause social harm.
- They believed that emphasizing a child's genetic traits over their intrinsic value treats the fetus like a commodity.
- The committee warned that if sex selection became acceptable, it might lead to the selection of other traits, such as intelligence or beauty.
1994 FIGO Position on Sex Selection:
- The International Federation of Gynecology and Obstetrics (FIGO) in 1994 permitted sex selection for social reasons, as long as it aligned with societal values.
2001 ASRM Update on Gender Selection:
- By 2001, the ASRM revised its position, allowing gender selection if the process was safe and effective.
- Couples opting for gender selection had to be fully informed of the risks and agree to accept children of any gender if the selection did not succeed.
- Practitioners were not legally or ethically obligated to offer non-medical gender selection.
Ethical Perspectives on Non-Medical Sex Selection:
- There are two primary ethical views regarding non-medical sex selection:
- A complete legal ban on the practice.
- Allowing it under strict conditions, as advocated by the ASRM, with regulation by a licensing authority.
The Pursuit of the Ideal Child
- Murray describes the search for the ideal child as the wish to achieve something that is completely flawless.
- He notes that the search for perfection in Western culture is a very old idea, dating back to Greek philosophy, even before Socrates.
- Throughout much of Western history, this quest took on a spiritual or metaphysical form.
- More recently, the idea of human perfection has connected with science and progress.
- He mentions that the quest for perfection was ready to align with modern science, particularly in the field of genetics.
- He suggests that it is now ready to utilize the growing power of genetic technology.
- Brom age argues that we can view these new obstetric technologies as a way to achieve "aesthetic normalisation", which meets the modern desire for perfection.
- Tong expresses hope that society will be brave enough to address why many parents wish to have "perfect" children.
- She believes that the search for the "perfect child" is not really about ensuring all children have equal chances for a normal life, but rather about making sure one's own child has a better opportunity than others.
- Murray points out that today's parents, feeling the pressure regarding their children, might want to shield themselves from the pain and disappointment that could come from having a child with a disability or disfigurement.
- He questions whether the value of the parent-child relationship should be measured by how well it avoids unpleasant experiences and focuses only on joyful moments.
- He warns that as we start to see our children's traits as a result of choices, we make ourselves more likely to face disappointment.
Attitudes Towards Disability
- The BMA states that society faces the challenge of helping those who want to prevent passing on a genetic disorder to their future children, while also giving full respect and proper support to individuals with disabling genetic conditions.
- Newell emphasizes that the perspectives of people with disabilities, along with those who advocate for social and human rights related to disability, are valuable for examining the field of bioethics.
- Parens and Asch argue in their critique of prenatal genetic testing that the practice followed by selective abortion raises serious moral issues and is influenced by misinformation.
- They identify two main moral concerns:
- Selective abortion reflects negative or discriminatory views, not only about a disabling trait but also about individuals who have it.
- It shows a lack of acceptance for diversity, both in society and within families, which may negatively affect how parents view their children.
- They also point out that prenatal testing is based on a misunderstanding of what life is like for children with disabilities. Recent studies indicate that many healthcare professionals see childhood disability as mainly negative, which contrasts with research showing that people with disabilities and their families can have high levels of life satisfaction.
- Additionally, they note that families with disabled children generally do not fare significantly better or worse than families without disabilities.
- On the other hand, some, like Gillam, believe that although prenatal diagnosis can lead to discrimination against individuals with disabilities, this is not an unavoidable outcome or a necessary part of the process.
- Gillam acknowledges that there is potential for negative impacts on people with disabilities and stresses that if prenatal diagnosis is to be ethically acceptable, it is important to recognize and address these negative effects as much as possible.
- Parens and Asch stress the importance of providing prospective parents with both information about disabilities and a chance to consider the values and aspirations that influence their decisions regarding prenatal genetic information.
- They emphasize that healthcare professionals must respect both the acceptance and rejection of such information by parents.
- Doctors have a moral, ethical, and professional duty to provide information to couples in a fair and unbiased manner, without pushing them towards ending a pregnancy.
Obstetric Interventions
- The clinical aspects of obstetric interventions are covered in their respective chapters. However, the legal implications of performing a Caesarean section on a competent woman without her consent, regardless of the potential consequences for her or her baby, are discussed in Chapter 58.
- Legal judgments consider such an intervention as assault and focus on the woman's capacity to make her own decisions. This topic will not be further explored in this section.
Request for Caesarean Section in the Absence of Medical Indications
- The latest guidelines from the National Institute for Clinical Excellence in the UK state that just wanting a C-section is not enough reason to have one.
- Some other experts believe that maternal preference should be a valid reason for choosing a C-section.
- This situation creates an ethical dilemma, as there are differing opinions on what should be a valid reason for having a C-section.
Case 15
- CJ is 32 years old and currently pregnant with her second child.
- Her first child, a boy, is now 3 years old and was born healthy after a normal pregnancy and delivery.
- The boy's birth weight was on the 60th percentile.
- CJ was referred to the hospital at 37 weeks of pregnancy because she had not felt any fetal movements for two days.
- There is no history of abdominal pain or vaginal bleeding.
- CJ is not in labor, her blood pressure is normal, and there are no signs of conditions like pre-eclampsia.
- Intrauterine fetal death has been confirmed.
- CJ requests a delivery by Caesarean section with general anesthesia because she does not want to deliver a dead baby or ruin the good memory of her last delivery.
- The question is whether to agree to her request or not, balancing her personal wishes with what is considered best for her health based on clinical experience.
- If labor were induced, it is likely that CJ would have a normal labor and could go home sooner than after a Caesarean section.
- A Caesarean delivery under general anesthesia or regional block carries more risks for CJ without any benefits for the fetus.
- A uterine scar from the Caesarean could also pose risks in future pregnancies.
- There is no clear right or wrong answer in this situation.
- Assuming that the decision is made against the Caesarean section and CJ later agrees to this, labor is induced.
- After 5 hours, she delivers a stillborn male infant.
- The cause of death is not clear, though the baby is small for his gestational age.
- CJ is able to go home within a few hours after the delivery.
- She returns two weeks later to discuss the pregnancy and expresses gratitude for not following her initial request.
- She feels that performing the Caesarean would have been treating her dead baby as if it were a tumor.
- Her feelings about the appropriateness of the situation do not determine whether the original decision was right or wrong.
- In articles discussing the ethics and facts surrounding requested Caesarean sections, it is stated that taking women's views seriously is good practice but not the only consideration in decision-making.
- They conclude that elective Caesarean sections have not been proven to be safer than labor based on current clinical evidence.
Gynecological Oncology
Case16
- Mrs. LW is a 58-year-old woman who underwent surgery and chemotherapy four years ago for ovarian cancer.
- The tumor has come back and is now widespread.
- She is admitted to the hospital, and you discuss treatment options, including a new session of aggressive chemotherapy.
- You inform her that the treatment is likely to make her feel quite unwell and that the chances of success are limited.
- You choose not to mention that the chemotherapy is very expensive.
- LW expresses her wish to avoid another round of chemotherapy and prefers to go home for palliative care as needed.
- Assuming you believe this is the right decision, a few days later, she returns with a change of heart.
- After discussing with her husband, older sister, and three children, she now wants to proceed with chemotherapy.
- You must decide between two options:
- The first option is that LW's initial choice accurately reflected her true feelings, but her family influenced her to change her mind.
- The second option is that during the first meeting, LW sensed that you thought she should avoid treatment, leading her to believe you knew what was best. It was only after talking with her family that she understood what she really wanted.
- In a busy hospital ward or clinic, it may be hard to recognize the importance of this second option.
- Her General Practitioner might offer some assistance, but they may not know LW and her family any better than you do.
- This situation highlights the importance of listening to the patient's story and the danger of making quick ethical judgments.
The document Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 is a part of the NEET PG Course Gynaecology and Obstetrics.
All you need of NEET PG at this link: NEET PG
FAQs on Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2
| $1. What are some common ethical dilemmas faced in obstetrics and gynaecology ? |  |
Ans. Common ethical dilemmas in obstetrics and gynaecology include issues related to informed consent, the right to refuse treatment, the management of maternal and fetal health risks, confidentiality in reproductive health, and the implications of prenatal testing and its potential outcomes. These dilemmas often arise when balancing the rights and health of the mother against those of the fetus, or when considering the moral implications of reproductive technologies.
| $2. How does informed consent play a role in obstetrics and gynaecology ? | |
Ans. Informed consent is crucial in obstetrics and gynaecology as it ensures that patients are fully aware of the risks, benefits, and alternatives to procedures or treatments. Ethical practice requires that patients understand the information provided to them and can make voluntary decisions regarding their care. This is especially important in scenarios involving complex procedures, prenatal testing, and decisions regarding pregnancy termination.
| $3. What are the ethical considerations surrounding prenatal testing ? | |
Ans. Ethical considerations surrounding prenatal testing include the potential for discrimination based on genetic information, the psychological impact of test results on parents, and the implications of choosing to terminate a pregnancy based on these results. Additionally, healthcare providers must navigate issues related to the availability of testing, informed consent, and the equitable access to these technologies for all patients.
| $4. How should healthcare providers approach the issue of maternal-fetal conflicts ? | |
Ans. Healthcare providers should approach maternal-fetal conflicts by prioritizing open communication and shared decision-making with patients. It is essential to respect the autonomy of the mother while also considering the health and well-being of the fetus. Providers should facilitate discussions that explore the ethical, medical, and personal implications of potential decisions to ensure that patients feel supported in their choices.
| $5. What role does confidentiality play in reproductive health services ? | |
Ans. Confidentiality is a fundamental ethical principle in reproductive health services, as it fosters trust between patients and healthcare providers. It ensures that sensitive information regarding a patient's reproductive choices, sexual health, and medical history is protected. Maintaining confidentiality is vital for encouraging individuals to seek care without fear of judgment or repercussions, thereby promoting overall health and well-being.
About this Document

4.65/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 for NEET PG 2026 is part of Gynaecology and Obstetrics preparation. The notes and questions for Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 covers topics like and Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2.
Introduction of Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 in English is available as part of our Gynaecology and Obstetrics for NEET PG & Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 in Hindi for Gynaecology and Obstetrics course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2
Description
Chapter Notes: Ethical dilemmas in obstetrics & gynaecology of Gynaecology & Obstetrics with clear explanations of key concepts & important topics of the chapter, to help you underst& lessons better & revise quickly, & crack the NEET PG exam.
Information about Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2
In this doc you can find the meaning of Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 defined & explained in the simplest way possible. Besides explaining types of Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 theory, EduRev gives you an ample number of questions to practice Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2 tests, examples and also practice NEET PG tests


Related Searches
shortcuts and tricks, study material, practice quizzes, Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2, Exam, Previous Year Questions with Solutions, pdf , video lectures, Semester Notes, Summary, Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2, Extra Questions, mock tests for examination, Objective type Questions, Chapter Notes: Ethical dilemmas in obstetrics and gynaecology- 2, ppt, Important questions, Sample Paper, past year papers, Free, Viva Questions, MCQs;