Nutrition


Introduction
Nutrition covers dietary macronutrients and micronutrients, their biochemical roles, deficiency and excess states, and metabolic handling. Important topics include essential fatty acids, fat- and water-soluble vitamins, mineral micronutrients, protein-energy malnutrition, and metabolic effects of ethanol.
Essential Fatty Acids

Definition: Polyunsaturated fatty acids that cannot be synthesised by the human body and therefore must be obtained from the diet (sources: nuts, seeds, plant oils, oily fish).
- Linoleic acid (omega-6) is metabolised to arachidonic acid, a precursor for prostaglandins, thromboxanes and leukotrienes (eicosanoids).
- Alpha-linolenic acid (omega-3) and its long-chain metabolites (EPA, DHA) have cardioprotective and antihyperlipidaemic effects.
- Trans-unsaturated fatty acids (industrial trans fats, found in some processed and fast foods) promote cardiovascular disease by increasing low-density lipoprotein (LDL) and decreasing high-density lipoprotein (HDL).
Fat-Soluble Vitamins (A, D, E, K)
The fat-soluble vitamins are A, D, E and K. Their absorption requires bile emulsification, pancreatic secretions and an intact ileum. These vitamins are stored in body fat and the liver, so toxicity from chronic excess is more likely than with water-soluble vitamins. Conditions causing fat malabsorption (for example, cystic fibrosis, coeliac disease) or mineral oil use can lead to deficiency.
Vitamin A (retinol, retinal, retinoic acid)
- Functions: antioxidant; constituent of visual pigments (retinal); essential for normal differentiation of epithelial tissues (prevents squamous metaplasia); supports immune function.
- Clinical uses: topical tretinoin (retinoic acid) and oral isotretinoin for acne; all-trans retinoic acid (ATRA) for acute promyelocytic leukaemia.
- Deficiency: night blindness (nyctalopia), xerosis (dry scaly skin), xerophthalmia, Bitot spots (foamy keratin debris on conjunctiva), keratomalacia and increased susceptibility to infections.
- Excess (hypervitaminosis A): acute-nausea, vomiting, raised intracranial pressure (headache, blurred vision); chronic-alopecia, dry skin, hepatotoxicity, arthralgia, pseudotumour cerebri. Vitamin A derivatives (for example isotretinoin) are teratogenic and require strict pregnancy prevention measures.
Vitamin D (ergocalciferol D2, cholecalciferol D3)
- Synthesis and activation: D3 produced in skin from 7-dehydrocholesterol on UV exposure; D2 from plants. Both are 25-hydroxylated in the liver to 25-OH D (storage form) and then 1α-hydroxylated in the kidney to 1,25-(OH)2D (calcitriol, active form).
- Functions: increases intestinal absorption of Ca2+ and PO43-; promotes bone mineralisation at normal levels and bone resorption at high levels.
- Regulation: parathyroid hormone (PTH), serum Ca2+ and PO43- regulate 1α-hydroxylase activity; 1,25-(OH)2D provides negative feedback on its own production.
- Deficiency: rickets in children (bone deformities such as genu varum), osteomalacia in adults (bone pain, muscle weakness), hypocalcaemic tetany. Causes include inadequate sun exposure, poor dietary intake, malabsorption, chronic kidney or liver disease. Breastfed infants may require vitamin D supplementation.
- Excess: hypercalcaemia, hypercalciuria, anorexia, confusion; granulomatous diseases can cause hypervitaminosis D by extra-renal activation of vitamin D.
Vitamin E (tocopherols, tocotrienols)
- Function: antioxidant that protects cell membranes (including red blood cells and neuronal membranes) from oxidative damage.
- Deficiency: haemolytic anaemia, acanthocytosis, peripheral neuropathy, posterior column and spinocerebellar tract degeneration leading to impaired proprioception and vibration sense and ataxia. Presentation may resemble vitamin B12 deficiency neurologically, but without megaloblastic anaemia or elevated methylmalonic acid.
- Excess: high-dose supplementation can increase the risk of bleeding (interferes with vitamin K metabolism) and may cause enterocolitis in infants.
Vitamin K (phylloquinone, menaquinone)
- Function: reduced vitamin K is a cofactor for the γ-carboxylation of glutamic acid residues on clotting factors II, VII, IX and X and proteins C and S. It is synthesised by intestinal microbiota and dietary sources include leafy green vegetables.
- Deficiency: bleeding diathesis with prolonged prothrombin time (PT) and prolonged activated partial thromboplastin time (aPTT); normal platelet function and bleeding time. Neonates are at risk because the gut is sterile; prophylactic vitamin K is routinely given at birth to prevent haemorrhagic disease of the newborn. Prolonged broad-spectrum antibiotics or hepatocellular disease can also produce deficiency.
- Warfarin inhibits the vitamin K epoxide reductase cycle and thus the activation of vitamin K-dependent clotting factors.
Water-Soluble Vitamins (B Complex and Vitamin C)
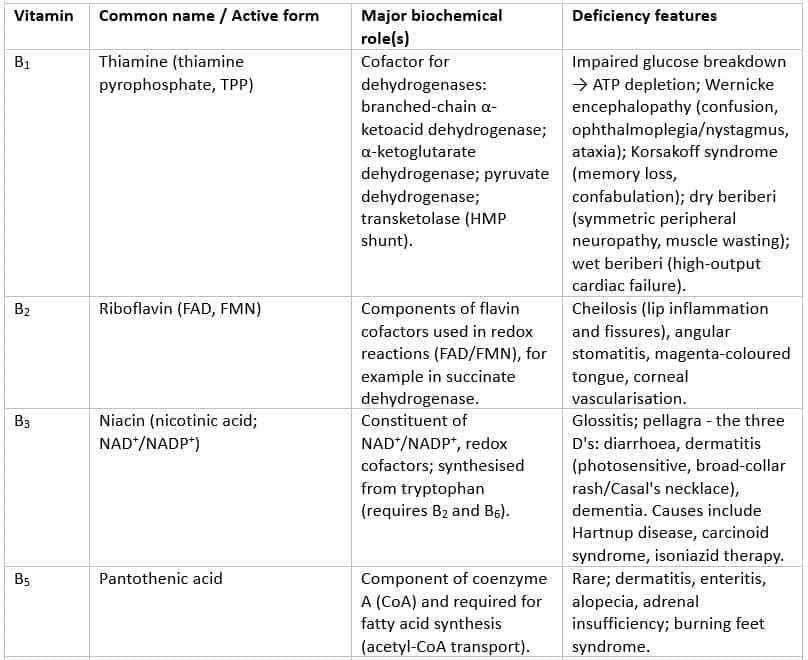
Water-soluble vitamins are readily excreted in urine (except for vitamin B12 and, to a lesser extent, folate). Deficiency of B-complex vitamins commonly causes dermatitis, glossitis and diarrhoea. Many B vitamins act as coenzymes or coenzyme precursors.

Selected Water-Soluble Vitamins and Key Features
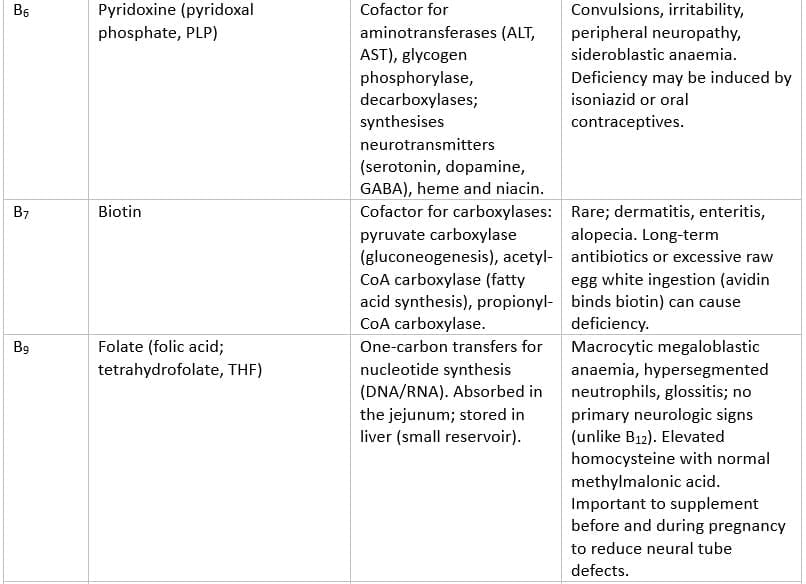
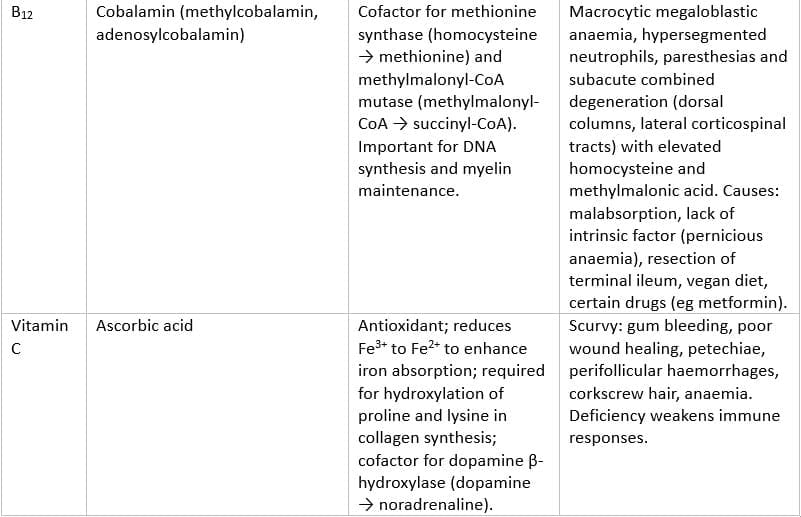
Additional Notes on Water-Soluble Vitamins
- Most water-soluble vitamins are not stored in large amounts and are readily lost; exceptions: vitamin B12 (large hepatic stores, several years) and folate (several months).
- Folate supplementation is recommended before conception and during pregnancy to reduce neural tube defects.
- Folate replacement can correct the haematologic abnormalities of vitamin B12 deficiency but will not prevent or reverse the neurological damage caused by B12 deficiency; therefore, assessing B12 before folate replacement is important in ambiguous cases.
Selected Minerals
Zinc
- Function: essential for >100 enzymes; structural role in zinc-finger transcription factors; important for growth, wound healing and immune function.
- Deficiency: delayed wound healing, impaired immunity, male hypogonadism, loss of axillary and pubic hair, dysgeusia, anosmia. Acrodermatitis enteropathica is a congenital defect of intestinal zinc absorption presenting with periorificial and acral dermatitis, alopecia and diarrhoea. Zinc deficiency may be seen in malnutrition and can be associated with alcoholic liver disease.
Protein-Energy Malnutrition
Protein-energy malnutrition (PEM) describes a spectrum from calorie deficiency to protein deficiency. Two classic forms are:
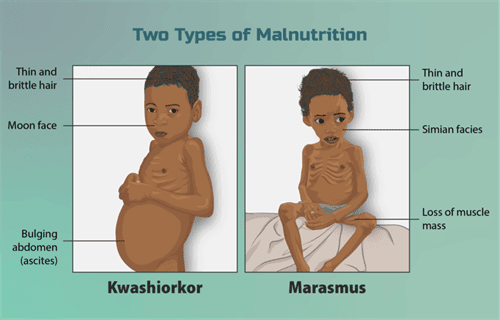
Kwashiorkor
- Cause: primarily protein deficiency with relatively preserved caloric intake.
- Features: oedema due to low plasma oncotic pressure (hypoalbuminaemia), fatty liver with hepatic steatosis (impaired apolipoprotein synthesis), skin changes (hyperkeratosis, dyspigmentation), irritability, anorexia. Typical clinical appearance is a small child with a distended abdomen.
Marasmus
- Cause: overall calorie deficiency (energy and protein deficiency).
- Features: severe muscle wasting and loss of subcutaneous fat, emaciation, but usually no oedema. Linear growth may be preserved in acute PEM versus chronic malnutrition.
Ethanol Metabolism and Metabolic Consequences
Ethanol is metabolised by several systems; the main hepatic pathway is via alcohol dehydrogenase (ADH) in the cytosol, which converts ethanol to acetaldehyde, producing NADH from NAD+. Acetaldehyde is then converted to acetate by aldehyde dehydrogenase (ALDH) in mitochondria, again generating NADH. A microsomal ethanol oxidising system (MEOS; CYP2E1) in the smooth endoplasmic reticulum also oxidises ethanol (important in chronic alcohol exposure and in generation of reactive oxygen species). Catalase in peroxisomes contributes minimally.
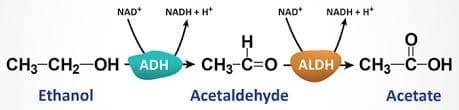
Reactions:
- ethanol → (ADH, cytosol) → acetaldehyde + NADH
- acetaldehyde → (ALDH, mitochondria) → acetate + NADH
- MEOS (CYP2E1) provides an alternative pathway and produces reactive oxygen species (ROS).
Physiological and biochemical consequences of an increased NADH/NAD+ ratio in the liver:
- Lactic acidosis - excess NADH shifts pyruvate → lactate.
- Fasting hypoglycaemia - gluconeogenesis is inhibited because oxaloacetate is diverted to malate.
- Ketoacidosis - acetyl-CoA is shunted to ketone formation rather than the tricarboxylic acid (TCA) cycle.
- Hepatic steatosis (fatty liver) - increased NADH promotes fatty acid synthesis and glycerol-3-phosphate formation, facilitating triglyceride synthesis and accumulation in hepatocytes.
Clinical and Pharmacological Points:
- Zero-order kinetics: alcohol dehydrogenase follows zero-order kinetics at usual drinking concentrations - a constant amount of ethanol is metabolised per unit time.
- Fomepizole is a competitive inhibitor of alcohol dehydrogenase and is used as an antidote for methanol or ethylene glycol poisoning (ethanol may also be used as a competitive substrate because ADH has higher affinity for ethanol than for methanol or ethylene glycol).
- Disulfiram inhibits aldehyde dehydrogenase, causing accumulation of acetaldehyde after ethanol ingestion and producing unpleasant effects (flushing, nausea, vomiting, tachycardia) to discourage drinking.
- Females are more susceptible to alcohol-related organ damage at lower doses due to lower gastric ADH activity, lower total body water (higher blood alcohol concentrations for a given dose) and other physiological differences.
Dietary Supplementation Considerations

Certain diets and conditions require attention to supplementation:
- Vegetarians and vegans: may require supplementation with vitamin B12 (animal products are the main dietary source) and sometimes iron and vitamin D.
- Vitamin B12: stored in the liver for several years; deficiency can occur with malabsorption (eg, resection of terminal ileum, pernicious anaemia) or strictly plant-based diets without supplementation.
- High raw egg white consumption: avidin in raw egg white binds biotin (vitamin B7) and can cause deficiency.
- Pellagra risk: diets based mainly on untreated maize (corn) low in bioavailable niacin and tryptophan can precipitate vitamin B3 deficiency.
- Fat-soluble vitamin status: malabsorption syndromes with steatorrhoea (eg, cystic fibrosis, coeliac disease) may cause deficiencies of vitamins A, D, E and K.
Summary
Nutrition integrates macronutrients and micronutrients with their biochemical roles and clinical consequences of deficiency or excess. Key points include the essential nature of omega-3 and omega-6 fatty acids, the fat- and water-soluble vitamin families with their cofactor roles and deficiency syndromes, the clinical importance of minerals such as zinc, the major forms of protein-energy malnutrition, and the metabolic and clinical effects of ethanol metabolism. Recognition of at-risk populations (eg, infants, pregnant women, people with malabsorption, strict vegans, chronic alcohol users) guides prevention and supplementation strategies.
FAQs on Nutrition
| 1. What are essential fatty acids and why are they important? |  |
| 2. What roles do fat-soluble vitamins play in human health? | |
| 3. How do water-soluble vitamins differ from fat-soluble vitamins? | |
| 4. What is protein-energy malnutrition and what are its consequences? | |
| 5. What considerations should be taken into account regarding dietary supplementation? | |


