Chapter Notes: Grief and Loss


Introduction
Every person at some point in their life experiences loss - whether it is a job, a cherished relationship, a pet, or ultimately the loss of life itself. As nurses, we stand at the frontline of supporting patients and their families through these deeply emotional and challenging moments. This chapter covers everything a nurse needs to know about grief, loss, palliative care, and end-of-life nursing - all based on the internationally recognized curriculum of the End-of-Life Nursing Care Consortium (ELNEC), which trains healthcare professionals to provide compassionate, skilled care to patients and families facing serious illness and death.- Nurses are typically the first line of support when patients and families face serious illness, loss, or end of life.
- The ELNEC (End-of-Life Nursing Care Consortium) is an international educational project sponsored by the American Association of Colleges of Nursing that equips nurses and healthcare professionals with skills to handle end-of-life care.
- The goal is to positively impact patients and families facing serious illness and death through specialized, evidence-based care.
Basic Concepts: Loss, Grief, and Mourning
Before diving into types and stages of grief, it is important to understand three foundational concepts that form the core of this topic.- Loss: This refers to the absence of something important, whether it is already gone or will be gone in the future. Loss can be the loss of health, a relationship, a role, or ultimately life itself. Example: A patient diagnosed with Parkinson's disease may feel loss of independence as the disease progresses.
- Grief: This is the emotional response to loss. It is deeply personal and individualized. Two people experiencing the same loss may grieve very differently. Grief can include feelings of anger, sadness, guilt, loneliness, regret, or even relief. It affects a person physically, psychologically, socially, and spiritually. Importantly, grief is not a straight line - a person may feel okay one day and devastated the next, which is completely normal.
- Mourning: This is the outward expression of grief, shaped by cultural norms, traditions, and personal background. For example, some cultures express grief through loud wailing and communal rituals, while others are very quiet and private in their mourning. Cultural background also determines how long someone is expected to mourn and what behaviors are appropriate.
Types of Grief
There are five recognized types of grief, each with its own characteristics and triggers.Anticipatory Grief
- Anticipatory grief happens before an actual loss occurs - usually triggered by a terminal or chronic illness diagnosis.
- Both patients and their family members can experience this. Example: A woman whose husband is diagnosed with terminal cancer may begin grieving the loss of her partner long before he dies.
- The patient may fear losing independence, body image, ability to drive, or the ability to attend important family milestones like a grandchild's birth or a child's wedding.
- Research suggests that anticipatory grief can actually help soften the impact of bereavement after the actual death occurs.
Acute Grief
- Acute grief begins immediately after the death of a loved one.
- The bereaved person may feel disbelief, shock, confusion about their identity, and withdrawal from daily activities.
- Example: A person who just lost a sibling in an accident may be unable to return to work for weeks because the reality of the loss has not fully set in.
Normal Grief
- Normal grief includes a wide range of emotional, physical, cognitive, and behavioral responses that are considered typical after a loss.
- Physical symptoms: Hollowness in the stomach, fatigue, tightness in the chest, heart palpitations, breathlessness, dry mouth, weakness.
- Emotional symptoms: Sadness, anger, guilt, fear, numbness, loneliness, relief, yearning, anxiety, helplessness.
- Cognitive symptoms: Confusion, inability to concentrate, dreaming of the deceased, a sense that the deceased is still present, idealization of the deceased.
- Behavioral signs: Crying, withdrawal from social activities, impaired work performance, avoidance of reminders of the deceased.
- Acute grieving may last months or even years. A person never truly "gets over" a loss, but they do eventually reconnect with life as their relationship with the deceased naturally evolves in memory.
Disenfranchised Grief
- Disenfranchised grief is grief that is not acknowledged or validated by society or others. The grieving person does not feel free to mourn openly.
- Examples:
- A person who loses a partner to AIDS may face social stigma that prevents open mourning.
- A mother grieving a miscarriage or stillbirth may find others dismissing her loss.
- A person grieving the end of a complicated relationship or an estranged friendship may not feel their loss is "valid" in the eyes of others.
Complicated Grief
- Complicated grief affects 10-20% of individuals who lose a romantic partner, and estimates are higher for parents who lose a child.
- Risk factors include sudden/traumatic death, suicide, homicide, dependent relationships, death of a child, multiple losses, lack of a support system or faith system, prior unresolved grief, and witnessing a painful dying process.
- There are four sub-types:
- Chronic Grief: Normal grief reactions that simply never subside over time. Example: A parent who lost a child 10 years ago still cannot function normally.
- Delayed Grief: Grief that is consciously or unconsciously suppressed to avoid pain and surfaces much later. Example: A soldier who loses comrades in war does not grieve until years later.
- Exaggerated Grief: An intense reaction that may include nightmares, phobias, delinquent behavior, or thoughts of suicide.
- Masked Grief: The person is not aware that certain behaviors are grief-related. Example: Someone who cancels all social plans to visit the cemetery every day without realizing this is disrupting their life.
- Complicated grief may require professional help such as counseling or therapy.
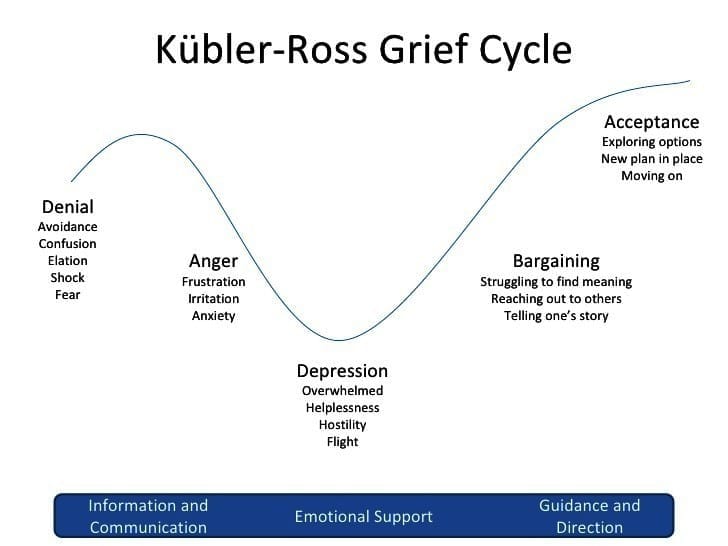
Stages of Grief (Kübler-Ross Model)
The famous Swiss psychiatrist Elisabeth Kübler-Ross described five stages of grief in her book On Death and Dying. These stages are commonly remembered using the mnemonic "DABDA". It is important to remember that these stages are not a strict sequence - a person may skip stages, repeat stages, or experience multiple stages at the same time. These stages apply not only to death but also to major life changes like divorce, job loss, or a serious diagnosis.- D - Denial: The person refuses to accept the reality of the loss. This acts as a protective mechanism. Example: A patient told they have terminal cancer says, "This can't be right, the tests must be wrong."
- A - Anger: Anger emerges as the loss becomes real. It may be directed at oneself, at others, at the healthcare team, or even at the person who died. Nurses must understand that anger directed at them is not personal - it is a manifestation of pain. Providing a safe space for expression while maintaining respectful boundaries is key.
- B - Bargaining: The person attempts to regain control by making deals, often with a higher power. Example: "I promise I'll be a better person if you just let my wife recover from this illness."
- D - Depression: Deep sadness sets in. The person may lose interest in activities, feel fatigue, experience insomnia, withdraw from others, and struggle to find meaning. Nurses should watch for unhealthy coping such as alcohol or drug use.
- A - Acceptance: The person acknowledges the new reality without denying the pain. They begin to re-engage with life, form new routines, and find moments of happiness. Acceptance does not mean the absence of sadness - it means learning to live with the loss.
Kubler-Ross Grief Cycle
Grief Tasks
In addition to the Kübler-Ross stages, grief can also be understood as a series of tasks that the bereaved person must work through:- Notification and Shock: The first task is simply accepting the reality of the loss. When someone first learns of a death, they may feel numb or go into shock and isolate themselves while processing the information.
- Experiencing the Loss: The second task involves actively working through the emotional and cognitive pain - allowing oneself to feel the sadness of separation rather than avoiding it.
- Reintegration: The third task involves adjusting to life without the deceased - adopting new roles, restructuring family relationships, and forming a new sense of normal while retaining precious memories of the person who died.
Palliative Care and Hospice
- Palliative Care is a broad philosophy of care aimed at improving quality of life for patients with life-limiting illnesses and their families. It addresses physical, psychosocial, and spiritual suffering. Crucially, palliative care is provided alongside curative treatments - a patient can receive chemotherapy and palliative care simultaneously. It can begin at any point during a serious illness.
- Hospice Care is a specific type of palliative care for patients who are expected to live six months or less. In hospice, the focus shifts entirely from curing the disease to providing comfort. Curative treatments (like chemotherapy) stop, but other medical treatments that support quality of life (like blood pressure medications or antibiotics for infection) may continue.
- Hospice services are available at home, in hospitals, nursing facilities, assisted living facilities, and even prisons.
- In the United States, older adults enrolled in Medicare can access hospice care including home medical equipment and medications related to the terminal diagnosis at no cost.
- A major barrier to hospice is the misconception that choosing hospice means "giving up." Many families resist it. Nurses must gently educate families that hospice is about living comfortably, not hastening death.
- Comfort Care is a term used in acute care settings when the goals shift from curative intervention to symptom control and quality of life, without a formal hospice admission. It is similar in philosophy but different in structure from hospice.
Ethical and Legal Considerations
- Nurses must always advocate for the patient's wishes, even when there is conflict among family members or the healthcare team.
- The American Nurses Association's Code of Ethics provides guidance for ethical dilemmas in end-of-life care.
- Many hospitals have ethics committees to provide support, resources, and guidance in complex ethical situations.
Do-Not-Resuscitate (DNR) Orders
- A DNR order is a medical order instructing healthcare professionals not to perform CPR if a patient's heart or breathing stops.
- It is written only with the consent of the patient or their health care power of attorney.
- CPR (Cardiopulmonary Resuscitation) may involve chest compressions, mouth-to-mouth breathing, electric shocks, breathing tubes, and cardiac medications.
- Important statistic: The overall survival rate for a person who experiences cardiac arrest and receives CPR is only about 10.6%. This helps families make informed, realistic decisions.
- Nurses play an important role in educating patients and families about CPR effectiveness based on the patient's condition.
Advance Directives
- Health Care Power of Attorney - A legal document that names a trusted person (over 18, of sound mind) to make healthcare decisions when the patient can no longer do so. This person must understand and carry out the patient's wishes.
- Living Will - A legal document describing what treatments the patient does or does not want if they cannot speak for themselves. It covers ventilator support, feeding tubes, CPR, and intubation. However, since it cannot cover every possible scenario, having a health care power of attorney is equally important.
Care of the Family - Fading Away
Fading away is the transition families experience when they suddenly realize their loved one is truly dying - even if they were told earlier. It is that gut-wrenching moment when they recognize that their loved one is "not going to get better." Both the patient and family go through several dimensions during this process:- Redefining: A shift from how life "used to be" to "how it is now." Example: A family stops planning a vacation and instead focuses on making the patient comfortable at home.
- Burdening: Patients may feel like a burden to their family, but family members typically view care as an act of love, not a burden.
- Searching for Meaning: Both the patient and family look inward, spiritually, and seek connections with loved ones to find meaning in the experience.
- Living Day to Day: Patients who find meaning try to live each day positively; families focus on making the most of remaining time together.
- Preparing for Death: Patients may want to leave a legacy - writing letters, recording memories. Families make funeral arrangements and handle financial matters.
- Contending with Change: Roles shift significantly - a spouse may become a caregiver, children may take on adult responsibilities, and normal social patterns change.
Caregiver Support
- Family caregivers provide 70-80% of care at home and work around the clock.
- Nurses must assess caregivers regularly for physical exhaustion, depression, and unhealthy coping behaviors (such as alcohol use).
- What caregivers want most:
- Practical support and help with daily tasks
- Honest communication from the healthcare team
- Confirmation that their loved one is being treated with dignity
- To be included in decision-making
- To be heard and listened to
- To be remembered as compassionate and dedicated
- Reassurance that they did everything they could
Caregiver Support
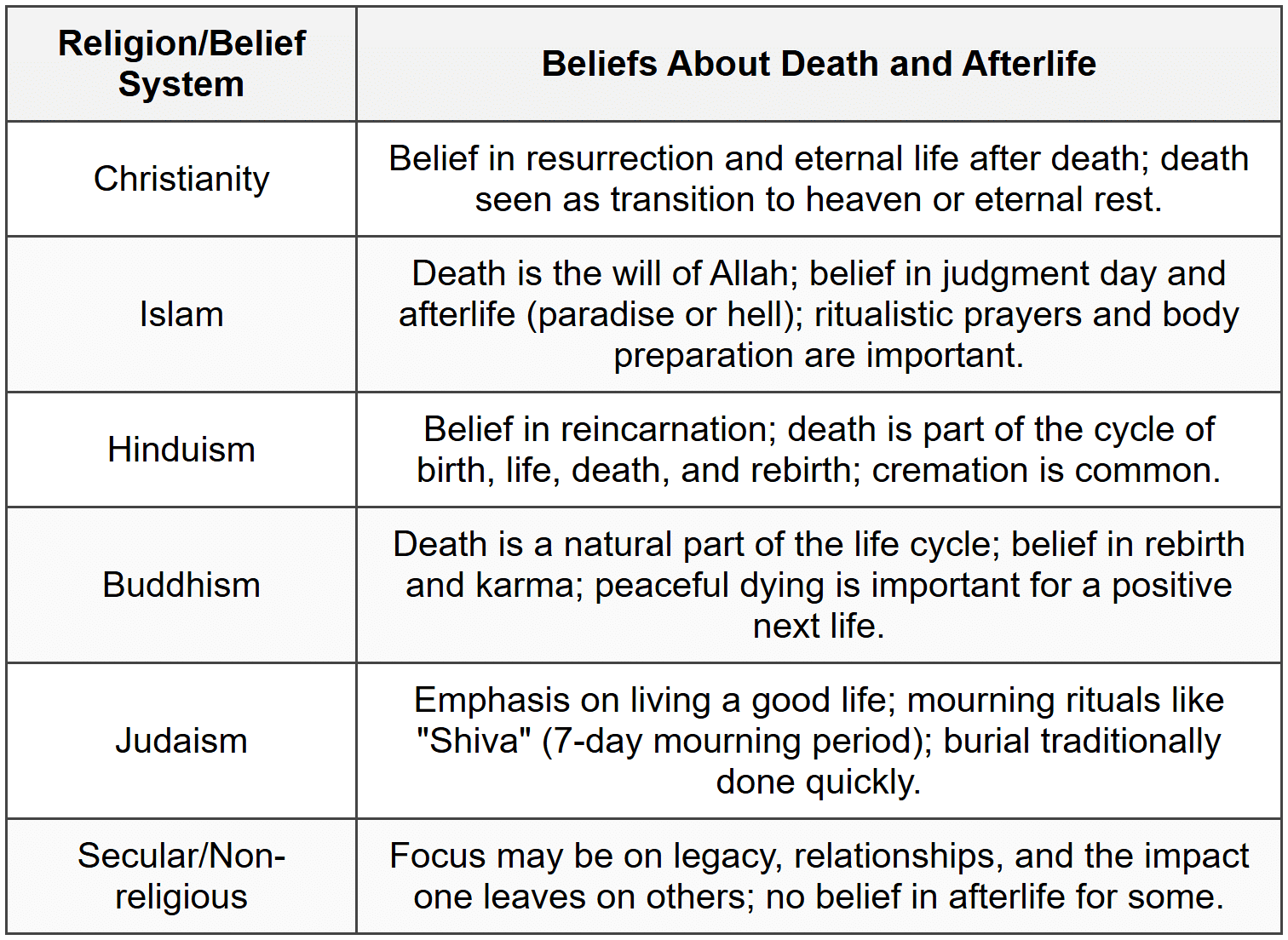
Cultural Considerations Regarding Death
- Cultural background deeply influences how a patient and family approach illness, pain, decision-making, spirituality, grief, dying, and bereavement.
- Nurses must assess cultural values and incorporate them into care planning in a sensitive and respectful manner.
- Different cultures have unique funeral traditions, mourning periods, and beliefs about what happens after death.
A Good Death
Research has identified several key elements that define what is considered a "good death" - a death that is meaningful, comfortable, and dignified for both the patient and family:- The patient's preferences for where and with whom they die are honored
- The patient is free from pain with emotional well-being maintained
- Family is prepared and supportive of the patient's wishes
- Dignity and respect are shown to the patient at all times
- The patient has a sense that their life was complete and well-lived
- Spiritual and religious comfort is provided
- Quality of life is maintained - including hope, gratitude, and moments of pleasure
- The patient feels trust, comfort, and support from the nursing and interdisciplinary team
Bereavement
- Bereavement encompasses both grief (internal feelings) and mourning (outward expression) after the death of a loved one.
- Bereavement can have serious physical consequences - it is associated with an increased risk of heart attack and cardiomyopathy. Widows and widowers have an elevated risk of dying after their spouse's death.
- Bereaved individuals should be encouraged to:
- Talk about the death and express their feelings openly
- Give themselves adequate time for grief - not rush through it
- Postpone major life decisions (like moving or changing jobs) during acute grief
- Draw on spiritual practices to cope
- The nurse's role during bereavement includes enhancing coping, facilitating spirituality, supporting the expression of grief, and communicating with the interdisciplinary team.
Grief in Children
- Children grieve differently depending on their developmental stage and may have difficulty verbalizing their feelings.
- Always use the word "death" with children - avoid euphemisms like "gone to sleep" or "passed away" as these create confusion.
- Younger children may show: nervousness, uncontrollable rages, hyperactivity, nightmares, denial, excessive anger, regression, or overdependence on the surviving parent.
- Older children may show: difficulty concentrating, decreased academic performance, social withdrawal, insomnia or sleeping too much, antisocial behavior, experimentation with alcohol or drugs, depression, or suicidal thoughts.
- Play is the universal language of children - therapeutic play can be a powerful tool to help children process grief.
- Refer children and families to grief specialists and local support groups as needed.
Grief in Parents, Grandparents, and Spouses
- For parents, losing a child is one of the most devastating losses possible.
- For grandparents, grief is twofold - they mourn the grandchild and also witness the pain of their own child (the parent), yet their grief is often overlooked.
- Loss of a spouse is ranked as the most stressful life event on life event scales. The deep emotional, social, and practical bonds of marriage make this loss uniquely painful and persistent.
Therapeutic Communication During Bereavement
What you say matters - but so does what you do not say. Being present and listening is often more valuable than trying to find the perfect words.- Avoid: "I know how you feel." - Instead say: "I'm sorry you're going through this."
- Avoid: "You should be over this by now." - Instead say: "Grief takes time. There's no rush."
- Avoid: "At least you had a good life together." - Instead say: "Tell me about your relationship with them."
- Encourage silence when appropriate - sometimes just being present without speaking is the most comforting thing a nurse can do.
Completion of the Grieving Process
- Grief work is never fully "done" - anniversaries, songs, objects, or memories may always bring up feelings of loss.
- However, healing is recognizableby these signs:
- The intensity of pain around the loss has decreased
- The person has adapted to life without the deceased
- The person has "let go" physically, psychologically, and socially - while still cherishing memories
- "Letting go" does not mean forgetting - it means adapting to the loss while maintaining the bond through memory and love.
Self-Care for Nurses
- Providing end-of-life care repeatedly, especially after traumatic losses, can deeply impact nurses emotionally.
- Compassion Fatigue - A state of chronic self-sacrifice and prolonged exposure to suffering that erodes a healthcare professional's physical, emotional, and spiritual well-being, eventually making it hard to empathize with patients.
- Burnout - Loss of motivation and cynicism triggered by workplace demands, inadequate resources, interpersonal stress, or policies that conflict with professional values.
- Signs to watch for in yourself:
- Has my behavior changed?
- Am I communicating differently with colleagues and patients?
- Am I tempted by destructive habits?
- Am I projecting my pain onto others?
- Healthy coping strategies include: prayer, meditation, exercise, art, music, journaling, and using employee assistance programs (EAP) for counseling.
- The four "A's" of self-care resilience:
- Attention: Be aware of your own physical, emotional, social, and spiritual health. Practice gratitude.
- Acknowledgement: Honestly recognize what you have witnessed as a healthcare professional. Do not invalidate your own experiences.
- Affection: Treat yourself with kindness and warmth. Avoid being overly self-critical.
- Acceptance: Embrace both your strengths and imperfections with peace, avoiding blame and victim mentality.
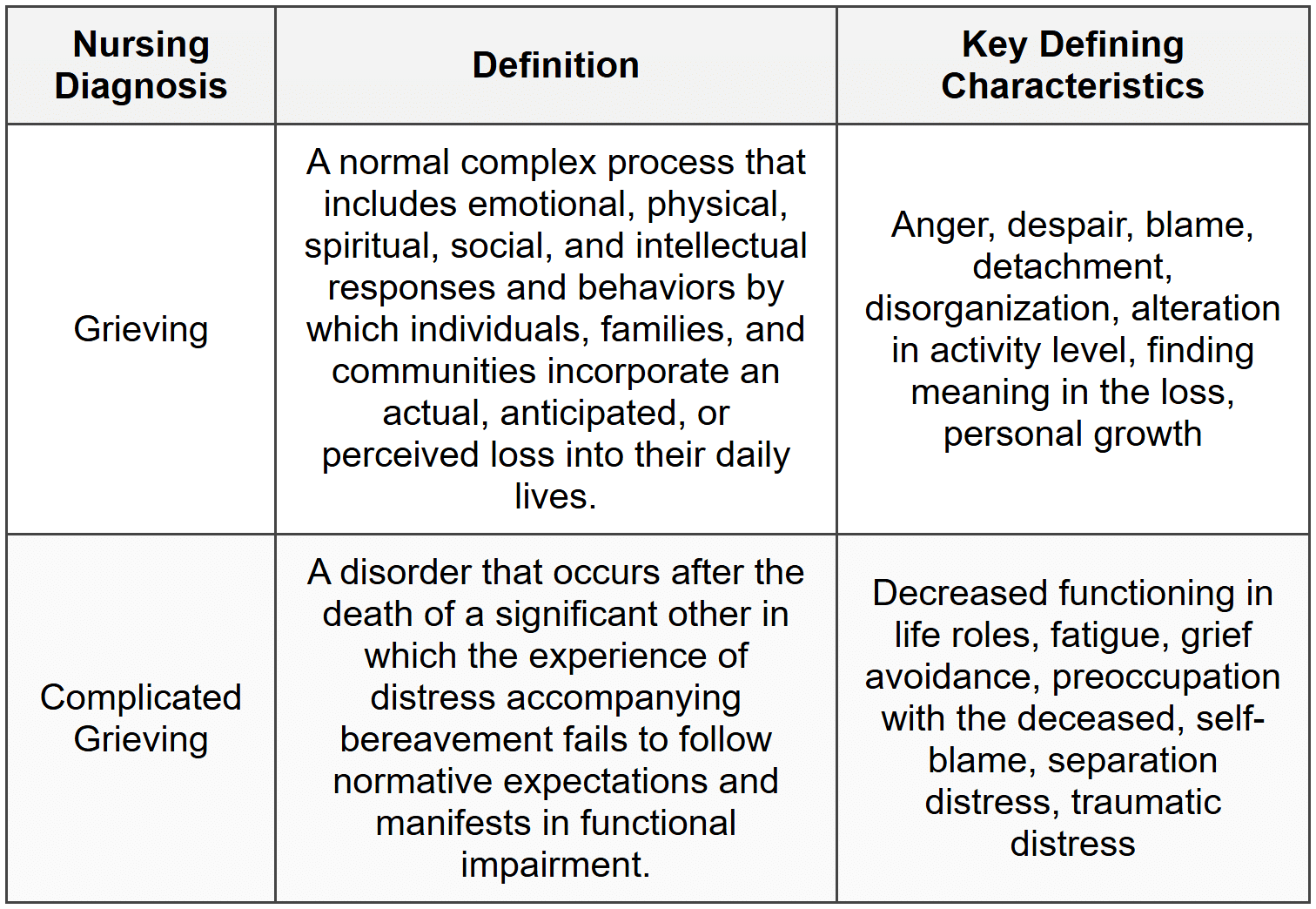
Applying the Nursing Process to Grief
Grief is a normal response to loss and has direct implications for patient and family well-being. NANDA-I formally recognizes two key nursing diagnoses related to grief: Grieving and Complicated Grieving. Communities can also grieve collectively - for example, after a devastating flood or community tragedy.Assessment
- Grief assessment includes the patient, family members, and significant others.
- It begins at the time of diagnosis and continues through the bereavement period after death.
- Grief can manifest as physical (headaches, insomnia, weight changes), cognitive (confusion, poor concentration), and emotional (anxiety, guilt, anger, sadness) symptoms.
- Any behavior that could endanger the patient - such as suicidal ideation or depression lasting more than 6 months - must be reported immediately.
NANDA-I Nursing Diagnoses
Outcome Identification
- Goals focus on grief resolution: resolving feelings about the loss, verbally accepting reality, maintaining daily living, and seeking social support.
- Sample SMART outcome: "The patient will discuss the meaning of the loss to their life within the next 2 weeks."
Nursing Interventions - Coping Enhancement
- Help the patient identify short- and long-term goals and available resources
- Break complex tasks into small, manageable steps
- Use a calm, reassuring, and accepting approach
- Encourage relationships with others who have shared experiences or interests
- Provide factual information about diagnosis, treatment, and prognosis
- Encourage realistic hope
- Teach relaxation techniques
- Acknowledge cultural and spiritual background and encourage use of spiritual resources
- Discourage major decisions during periods of severe stress
Coping Enhancement

Nursing Interventions - Anticipatory Grieving
- Build a trusting relationship using therapeutic communication and presence
- Keep patients and families informed about the patient's condition and healthcare options
- Actively listen and normalize the patient's expressions of grief about their own impending death
- Discuss and document the patient's preferred place of death
- Recognize caregiver role strain in family members providing long-term care
- Refer to chaplains, counselors, or clergy as appropriate
Nursing Interventions - Grief Work Facilitation
- Identify and acknowledge the loss clearly
- Listen to expressions of grief without judgment
- Make empathetic statements and encourage verbalization of memories
- Educate about the stages and tasks of the grieving process
- Support progression through personal grieving stages at the individual's own pace
- Encourage cultural and religious customs associated with mourning
- Identify community support sources and refer the patient to support groups
- Answer children's questions about loss clearly and honestly
Palliative Care Management
Palliative care is not just end-of-life care - it begins at diagnosis and continues throughout the course of any serious illness. It addresses multiple dimensions of a patient's well-being:
- Physical: Pain, fatigue, sleep disturbances, nausea, appetite, constipation
- Psychological: Anxiety, depression, fear, cognitive changes, distress
- Social: Caregiver burden, financial stress, role changes, relationships
- Spiritual: Hope, meaning, suffering, religiosity, transcendence
As a nurse in palliative care, key interventions include eliciting the patient's goals, listening carefully, communicating with the team, managing symptoms, facilitating spiritual practices, and making appropriate referrals.
Common Symptoms and Their Management
Pain
- Pain is "whatever the experiencing person says it is, existing whenever he says it does."
- For non-verbal patients, assess behavioral cues like grimacing, guarding, and moaning.
- Goal: Balance adequate pain relief with the patient's desire to remain alert.
- Many analgesic options exist - reassure patients that pain control is achievable.
Dyspnea (Breathlessness)
- Dyspnea is the most reported symptom in patients with life-limiting illness and can be extremely frightening.
- Assessment includes: rating scale (0-10), ability to speak in full sentences, respiratory rate, oxygen saturation, anxiety level, and lung sounds.
- Pharmacological: Small doses of opioids can significantly improve dyspnea without substantially shortening life.
- Non-pharmacological: Pursed-lip breathing, fans/open windows, elevation of the head of bed, tripod positioning, relaxation techniques, calm environment.
Cough
- Chronic cough causes pain, fatigue, vomiting, and insomnia and is common in COPD, heart failure, cancer, and AIDS.
- Treatment options include opioids, dextromethorphan, benzonatate, guaifenesin (to thin secretions), and anticholinergics (for high-volume secretions).
Anorexia and Cachexia
- Anorexia = loss of appetite; Cachexia = wasting of muscle and fat tissue.
- Weight loss is associated with decreased survival. However, aggressive nutritional intervention does not improve outcomes and may increase discomfort.
- Interventions focus on eating for pleasure: favorite foods, small frequent meals, high-calorie options, pleasing presentation.
- Educate family that forcing the patient to eat may cause more discomfort.
- Medications like mirtazapine, olanzapine, metoclopramide, or medical marijuana may be prescribed.
Constipation
- Defined as fewer than 3 bowel movements per week.
- Caused by reduced food/fluid intake, opioid use, chemotherapy, or immobility.
- Goal: Bowel movement at least every 72 hours.
- Treatment: Stool softeners (docusate) stimulant laxatives (sennosides); rectal suppositories or enemas if oral medications fail.
Diarrhea
- Defined as more than 3 unformed stools in 24 hours.
- Can cause dehydration, electrolyte imbalance, and skin breakdown.
- Treatment: Hydration (water, sports drinks), IV fluids if needed, loperamide, psyllium, or anticholinergic agents.
Nausea and Vomiting
- Common in advanced disease and often a feared side effect of cancer treatment.
- Non-pharmacological: Room-temperature meals, avoid strong odors, small portions, relaxation techniques, music therapy.
- Pharmacological: Antiemetics such as prochlorperazine and ondansetron.
Depression
- Sadness is normal in serious illness, but persistent hopelessness, helplessness, and suicidal ideation are not normal and must be treated.
- Undertreated depression reduces immune function, quality of life, and survival.
- Pharmacological: SSRIs (fluoxetine, sertraline, paroxetine, citalopram) are first-line treatment.
- Non-pharmacological: Reminiscing and life review, grief counseling, relaxation techniques, spiritual support, cognitive behavioral techniques, reducing isolation, promoting autonomy.
- Nurses must always conduct a suicide assessment. Ask directly: "Have you had thoughts of harming yourself?" Normalize the question: "It wouldn't be unusual for someone in your situation to have such thoughts. Have you?"
Anxiety
- A subjective feeling of apprehension and unease; assessed on a continuum from mild to severe.
- Physical symptoms: Sweating, tachycardia, trembling, chest pain, insomnia, restlessness.
- Cognitive symptoms: Persistent worried thoughts, difficulty concentrating.
- Pharmacological: Benzodiazepines (lorazepam) - with caution in the elderly due to fall risk.
- Non-pharmacological: Relaxation and guided imagery, spiritual support, active listening, identifying effective coping strategies, stress diary, providing clear concrete information.
Delirium (Cognitive Changes)
- An acute change in cognition - very common in palliative settings, and up to 90% of patients develop it in their final hours.
- Symptoms: Agitation, confusion, hallucinations, inappropriate behavior.
- Most common cause at end of life: Medications, followed by organ failure.
- Management: Neuroleptics (haloperidol, chlorpromazine), benzodiazepines, family presence for reorientation, massage, distraction, and relaxation.
Fatigue
- Defined as a distressing, persistent sense of tiredness not proportional to activity that interferes with normal function.
- Causes include metabolic alteration from chronic disease, anemia, poor sleep, pain, and medication side effects.
- Intervention: Energy conservation techniques - prioritizing important activities and resting between tasks.
Pressure Injuries
- Patients at end of life are highly susceptible to pressure injuries due to immobility, poor nutrition, and moisture.
- Prevention is key: promote mobility, manage moisture, encourage nutrition as tolerated.
- The Kennedy Terminal Ulcer is a special type of pressure injury that develops rapidly near death due to multiorgan failure, typically starting on the sacrum in a pear, butterfly, or horseshoe shape. It progresses so quickly that it may appear within a single nursing shift.
Seizures
- Caused by abnormal electrical brain activity; may result from infection, tumors, brain injury, metabolic imbalances, or drug toxicity.
- Focus is on prevention and limiting trauma during the seizure.
- Medications: Phenytoin, phenobarbital, benzodiazepines, levetiracetam.
Sleep Disturbances
- Poor sleep dramatically reduces quality of life and increases suffering.
- Often caused by uncontrolled pain or symptom management and environmental disturbances.
- Nurses can improve sleep by creating a quiet environment, promoting consistent sleep routines, and advocating for periods of uninterrupted rest.
Nursing Care During the Final Hours of Life
When death is approaching, the nurse has two critical responsibilities: symptom management and preparing the family for what to expect. Every person dies in their own way - there is no single "typical" death.
Pain and Dyspnea in Final Hours
- Pain assessment becomes challenging as consciousness decreases - rely on behavioral cues (grimacing, posturing).
- Roxanol (concentrated oral morphine sulfate, 20 mg/mL) can be given sublingually to relieve both pain and "air hunger" (severe breathlessness).
- Morphine not only relieves pain but also relaxes respiratory muscles and improves air exchange.
Terminal Secretions ("Death Rattle")
- Typically observed 3-23 hours before death.
- A gurgling sound caused by secretions in the throat as the patient loses the ability to swallow.
- Very distressing for families to hear.
- Treatment: Anticholinergics (atropine or scopolamine) to dry secretions; reposition on side if possible.
- Suctioning is not recommended - it is ineffective and causes additional distress to the patient.
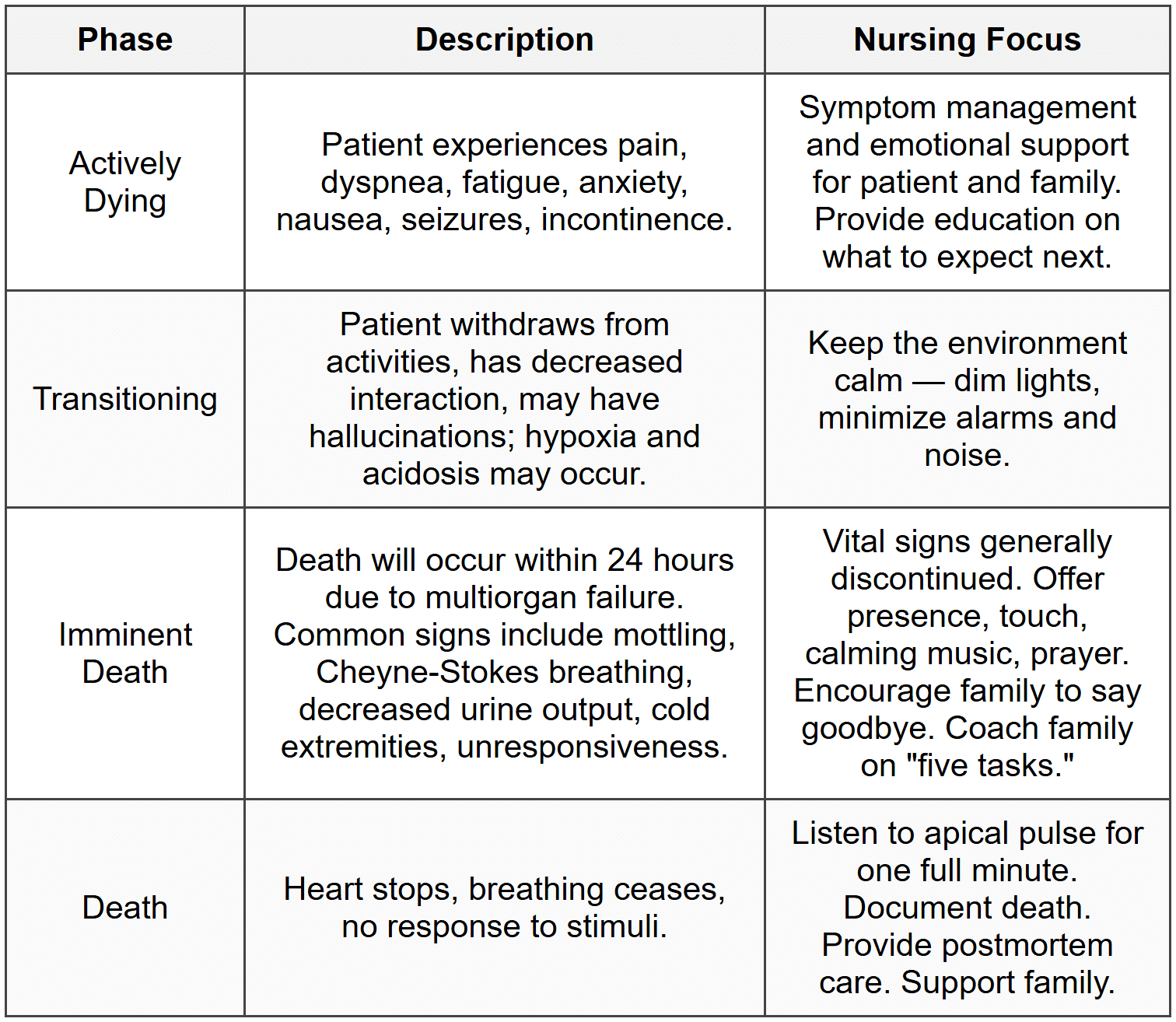
Phases of Dying
Five Tasks for Family Members as Parting Words
- Ask for forgiveness
- Offer forgiveness
- Say "Thank you"
- Say "I love you"
- Say "Goodbye"
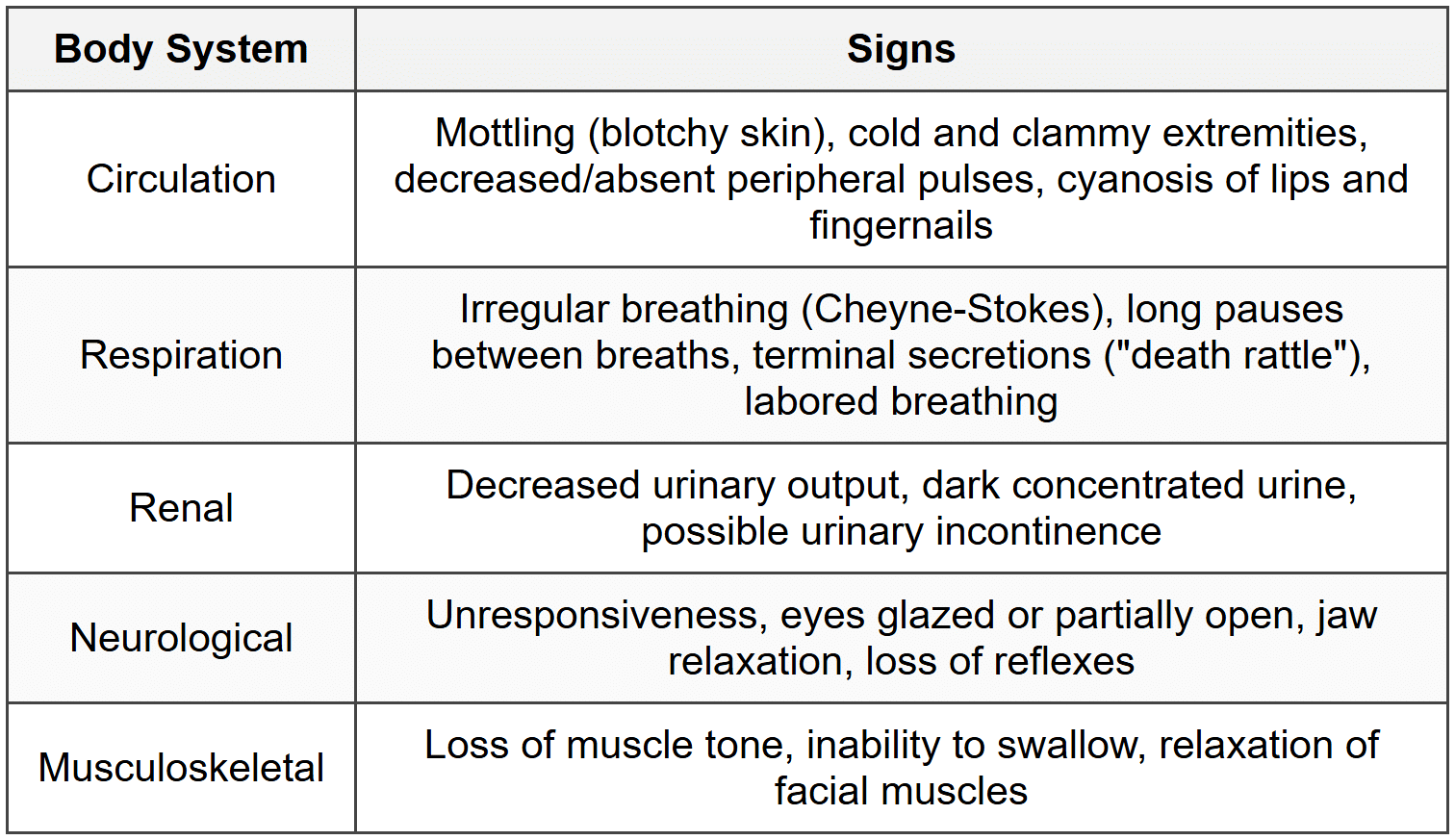
Typical Signs as Death Becomes Imminent
Death Vigil
Postmortem Care
- Clinical death = cessation of heartbeat and respiration. Biological death = brain and organ cell death from lack of oxygen (occurs within 4-6 minutes).
- Rigor mortis begins several hours after death, peaks at 12-18 hours, and disappears by 48 hours.
- The nurse's postmortem assessment documents: date/time, individuals present, absence of apical pulse, lack of response to stimuli, and arrangements for body transport.
- Postmortem care includes:
- Removing medical equipment/tubes (unless a coroner requires otherwise)
- Bathing, dressing, and positioning the body with respect and dignity
- Placing dentures, dressing wounds, applying incontinence products
- Honoring cultural practices around body care after death
- Allow the family adequate time to say goodbye - do not rush them. Support them in taking photos, holding hands, or simply being present with their loved one.
- Burial: The body is embalmed (blood replaced with formaldehyde-based solution) to be displayed at a funeral or memorial service.
- Cremation: Heat reduces the body to ashes placed in an urn - may be buried, placed in a mausoleum, or kept at home depending on cultural preferences.
Organ Donation
- Federal law and Medicare regulations require that hospitals offer families the opportunity for organ and tissue donation.
- Many families find comfort in knowing their loved one helped save another life.
- There is no cost for organ or tissue donation to the donor family.
Applying the Nursing Process at End of Life
Assessment at End of Life
- Routine assessments (vital signs, intake/output, blood draws) are generally discontinued as comfort becomes the priority.
- Subjective: Many patients are non-verbal; family members should be encouraged to speak to the patient as hearing may remain intact until the very end.
- Objective: Monitor for signs of pain (grimacing, moaning, guarding), labored breathing, terminal secretions, mottling, and skin breakdown.
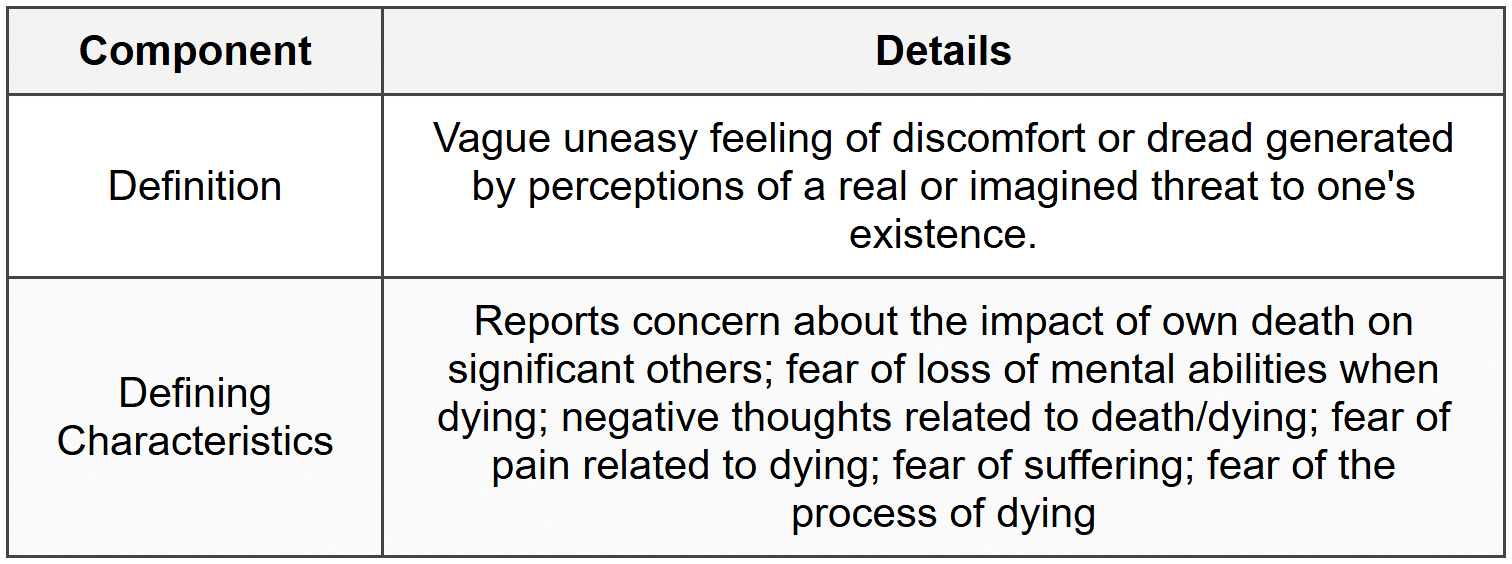
NANDA-I Diagnosis: Death Anxiety
Goals and Outcomes for Actively Dying Patients
- Overall goal: "The patient will experience dignified life closure."
- Evidence of this includes: expressing readiness for death, resolving important issues, sharing feelings about dying, discussing spiritual concerns.
- Sample SMART outcome: "The patient will express their fears associated with dying by the end of the shift."
Key Nursing Interventions in the Last Days and Hours
- Honor every patient preference for end-of-life care
- Provide physical care with utmost respect - shield from harsh light, loud voices, unnecessary procedures
- Reinforce the dying process steps repeatedly for the family - they may not retain information due to emotional distress
- Be present and practice active, empathetic listening
- Encourage a quiet, comfortable, and meaningful environment
- Assess and manage pain consistently based on patient goals
- Assist with life review and reminiscing
- Provide music of the patient's choosing
- Recognize and support spiritual needs - call chaplains or clergy as needed
- Encourage family to touch, hold, and speak to their loved one
- After death occurs, allow time for closure before moving the body
- Medicate for pain (morphine) and anxiety (lorazepam) using appropriate routes; anticipate need for subcutaneous pumps if oral route fails
- Administer anticholinergics (atropine/scopolamine) for terminal secretions
Patient Scenario: Putting It All Together
Patient: Mr. Yun, 34-year-old male, recently lost his wife in a motor vehicle accident. He presents with difficulty concentrating, insomnia, 15 lb weight loss in one month, and consuming 5-6 alcoholic drinks nightly to "numb himself."
- Nursing Diagnosis: Ineffective Coping related to inability to deal with a situation as manifested by unintended weight loss, difficulty concentrating, difficulty sleeping, and drinking 5-6 alcoholic beverages daily.
- Overall Goal: The patient will demonstrate improved coping.
- SMART Outcome: Mr. Yun will verbalize three positive coping behaviors by the end of the teaching session.
- Nursing Interventions:
- Identify the patient's personal resources and relationships
- Use empathetic communication to build rapport
- Encourage activities that bring personal satisfaction
- Educate about healthy coping strategies (exercise, meditation, prayer)
- Provide information about community support resources
- Evaluation: Mr. Yun identified three positive coping strategies - daily walks, limiting alcohol to two drinks, and using a meditation app nightly. He also planned to join a church-based widowers' support group. SMART outcome was met.
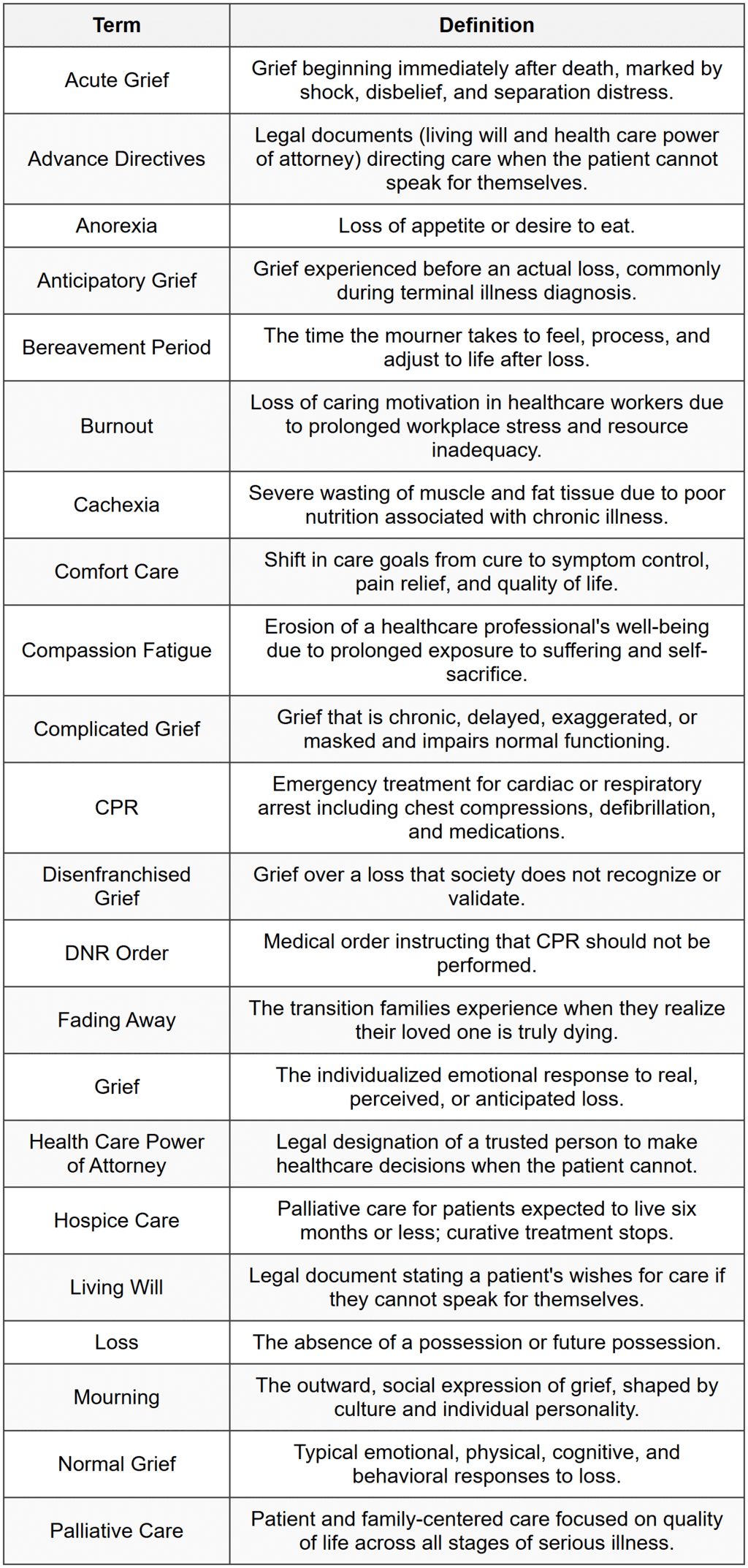
Glossary of Key Terms
FAQs on Chapter Notes: Grief and Loss
| 1. What are the basic concepts of loss, grief, and mourning? |  |
| 2. What are the different types of grief? | |
| 3. Can you explain the stages of grief according to the Kübler-Ross model? | |
| 4. What role do grief tasks play in coping with loss? | |
| 5. How do cultural considerations impact the care of the family during grief? | |
