Practice Questions :Mental and Physical Health

SECTION I: MULTIPLE CHOICE
Directions
Each of the questions or incomplete statements below is followed by four suggested answers or completions. Select the one that is best in each case and write your answer on a separate sheet of paper.
Question 1
Research Scenario: Dr. Martinez conducted a study examining the relationship between exercise frequency and symptoms of depression. Participants were 200 adults diagnosed with major depressive disorder who were randomly assigned to either a control group (no exercise intervention) or an experimental group (30 minutes of aerobic exercise, 5 days per week for 8 weeks). Depression symptoms were measured using the Beck Depression Inventory (BDI) at the beginning and end of the study. Results showed that the experimental group had significantly lower BDI scores at the end of the 8 weeks compared to the control group (p < 0.001).
Which of the following best describes the research method used in this study?
- Correlational study, because the researcher examined the relationship between two variables
- Experiment, because participants were randomly assigned to conditions and the independent variable was manipulated
- Naturalistic observation, because the researcher observed exercise behavior in real-world settings
- Case study, because the researcher examined individuals with depression in depth
Question 2
Research Data: A psychologist studying stress and immune function collected the following data from 150 college students during final exam week:
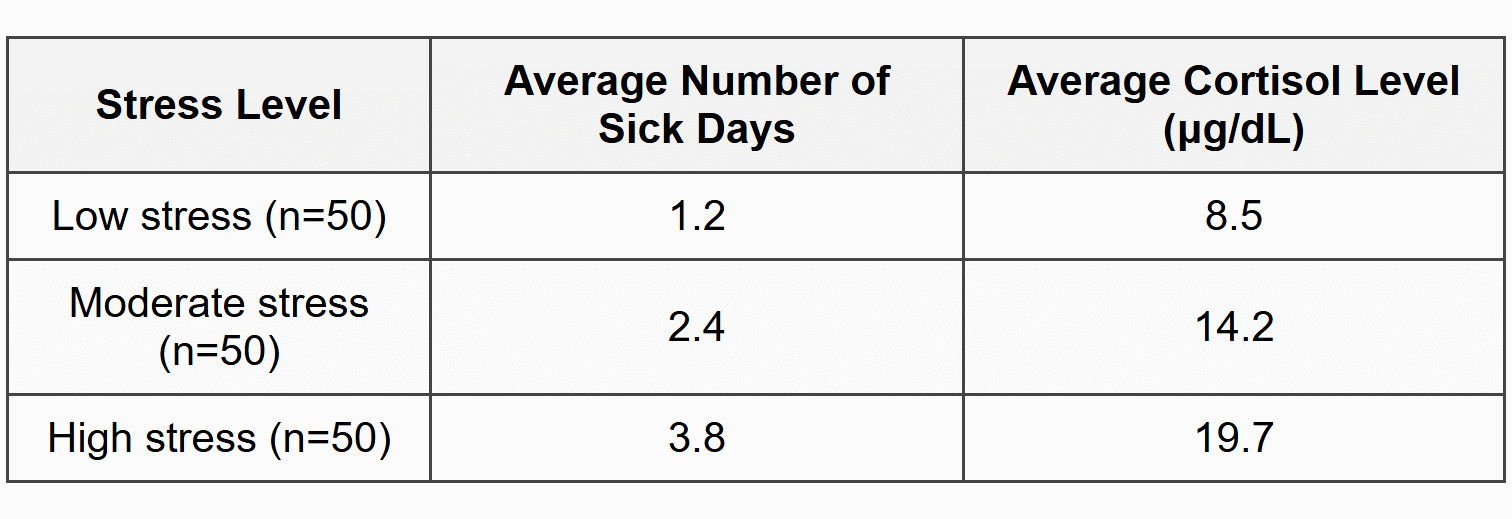
The data in the table best support which of the following conclusions?
- High stress causes elevated cortisol levels, which directly suppress immune function and increase illness
- There is a positive correlation between stress level and both cortisol levels and number of sick days
- Cortisol levels decrease as stress increases, demonstrating an inverse relationship
- The number of sick days is independent of stress level because correlation does not prove causation
Question 3
A patient with generalized anxiety disorder is prescribed a selective serotonin reuptake inhibitor (SSRI). The medication works by blocking the reuptake of serotonin in the synaptic gap, which increases the availability of serotonin to bind with receptor sites on the postsynaptic neuron. This mechanism most directly supports which explanation of anxiety disorders?
- Anxiety results from unresolved unconscious conflicts from childhood experiences
- Anxiety is maintained through negative reinforcement when avoidance reduces distress
- Anxiety disorders involve dysregulation of neurotransmitter systems in the brain
- Anxiety develops from maladaptive cognitive schemas and irrational thought patterns
Question 4
Clinical Vignette: Marcus experienced a traumatic car accident six months ago. Since then, he has persistent intrusive memories of the accident, avoids driving or riding in cars, experiences hypervigilance when near traffic, and has difficulty sleeping. His therapist uses a treatment approach that involves having Marcus gradually and repeatedly describe the accident in detail while in a safe, controlled environment until his anxiety response diminishes.
The therapeutic technique being used is based on which psychological principle?
- Systematic desensitization, which pairs relaxation with anxiety-provoking stimuli
- Exposure therapy based on extinction, which reduces the conditioned fear response through repeated presentation without the unconditioned stimulus
- Cognitive restructuring, which challenges and modifies irrational beliefs about the traumatic event
- Free association, which allows unconscious conflicts related to the trauma to emerge into consciousness
Question 5
Research Study: Researchers investigating the relationship between sleep deprivation and mental health recruited 300 adults and tracked their sleep patterns using wrist actigraphy for 30 consecutive days. Participants also completed daily mood assessments. The study found that participants who averaged fewer than 6 hours of sleep per night reported significantly higher levels of depression and anxiety symptoms compared to those who averaged 7-9 hours (r = -0.58, p < 0.001).
Which of the following is the most significant limitation of this study's ability to establish causation?
- The sample size was too small to detect meaningful relationships between variables
- The correlational design does not allow researchers to determine whether sleep deprivation causes mental health symptoms or whether mental health symptoms cause sleep deprivation
- Self-report measures of mood are inherently unreliable and invalid
- The study violated ethical guidelines by not providing treatment to participants with mental health symptoms
Question 6
According to the diathesis-stress model of mental disorders, which of the following best explains why two individuals exposed to the same traumatic event may have different outcomes, with one developing post-traumatic stress disorder (PTSD) and the other not developing the disorder?
- Mental disorders are entirely determined by genetic factors, so only individuals with specific genes will develop PTSD
- Individuals differ in their biological and psychological vulnerabilities, and those with greater predispositions are more likely to develop disorders when exposed to environmental stressors
- The severity of trauma alone determines whether PTSD develops, regardless of individual characteristics
- Social support has no influence on mental health outcomes following trauma
Question 7
Case Study: Jamal is a college student who has been experiencing persistent sadness, loss of interest in activities he once enjoyed, difficulty concentrating, significant weight loss, and thoughts that life is not worth living. These symptoms have been present for the past three months and are interfering with his academic performance and social relationships. His roommate encouraged him to seek help at the university counseling center.
Based on the DSM-5 criteria, Jamal's symptoms are most consistent with which diagnosis?
- Bipolar disorder, because he is experiencing mood changes
- Major depressive disorder, because he displays multiple depressive symptoms that have persisted for more than two weeks and cause significant impairment
- Generalized anxiety disorder, because he has difficulty concentrating
- Schizophrenia, because his symptoms interfere with his daily functioning
Question 8
Research Findings: A meta-analysis of 47 studies examining the effectiveness of cognitive-behavioral therapy (CBT) for anxiety disorders included a total of 3,490 participants. The analysis found that CBT produced a mean effect size of d = 0.85 for reduction in anxiety symptoms, with 68% of participants showing clinically significant improvement compared to 32% in wait-list control conditions.
Which of the following best describes what the effect size (d = 0.85) indicates about the effectiveness of CBT?
- The effect size indicates a small practical significance, suggesting CBT produces minimal symptom reduction
- The effect size indicates a large practical significance, suggesting CBT produces substantial symptom reduction compared to control conditions
- The effect size measures statistical significance, indicating that 85% of the results were due to chance
- The effect size indicates that CBT is effective for only 85% of anxiety disorders
Question 9
The general adaptation syndrome (GAS), proposed by Hans Selye, describes the body's response to stress in three stages: alarm, resistance, and exhaustion. During the exhaustion stage, prolonged exposure to stress can lead to which of the following outcomes?
- Enhanced immune function and increased resistance to disease
- Depletion of physiological resources, increased vulnerability to illness, and potential development of stress-related disorders
- Complete adaptation to the stressor with no negative health consequences
- Immediate activation of the parasympathetic nervous system and rapid recovery
Question 10
Experimental Design: Researchers studying the impact of mindfulness meditation on stress recruited 120 participants and randomly assigned them to one of two conditions: a mindfulness meditation group that practiced 20 minutes of guided meditation daily for 8 weeks, or a control group that listened to educational podcasts for the same duration. Stress levels were operationally defined as scores on the Perceived Stress Scale (PSS), measured before and after the intervention. Results showed that the meditation group had significantly lower PSS scores at post-test (M = 14.2, SD = 3.1) compared to the control group (M = 22.8, SD = 4.3).
Which of the following best explains why random assignment was used in this study?
- To ensure that participants in both groups were similar on characteristics that might affect stress levels before the intervention began, minimizing the influence of confounding variables
- To guarantee that all participants would experience reduced stress regardless of which group they were assigned to
- To allow researchers to generalize findings to all populations without limitation
- To eliminate the need for a control group in the experimental design
Question 11
The hypothalamic-pituitary-adrenal (HPA) axis plays a central role in the body's stress response. When an individual perceives a stressor, the hypothalamus releases corticotropin-releasing hormone (CRH), which triggers the pituitary gland to release adrenocorticotropic hormone (ACTH), which in turn stimulates the adrenal glands to release cortisol. Chronic activation of the HPA axis is associated with which of the following health outcomes?
- Improved cardiovascular health and enhanced cognitive function
- Weakened immune response, increased inflammation, and elevated risk for depression and anxiety disorders
- Decreased blood glucose levels and reduced energy availability
- Enhanced memory consolidation and increased neuroplasticity
Question 12
Treatment Scenario: Sophie has been diagnosed with major depressive disorder and is receiving a combination of antidepressant medication (an SSRI) and weekly sessions of cognitive-behavioral therapy. Her psychiatrist monitors medication effects and side effects, while her therapist helps her identify and challenge negative thought patterns and develop behavioral activation strategies.
This treatment approach is best described as which of the following?
- Psychoanalytic therapy, which focuses on unconscious conflicts
- Biomedical treatment exclusively, which relies only on medication intervention
- An eclectic or integrative approach, which combines biological and psychological interventions
- Humanistic therapy, which emphasizes self-actualization and personal growth
Question 13
Research Study: Psychologists examined the relationship between social support and recovery from surgery. They recruited 200 patients undergoing knee replacement surgery and assessed their level of social support (measured by number of close relationships and frequency of social contact) one week before surgery. Recovery was measured by time to independent mobility and self-reported pain levels at 2, 4, and 6 weeks post-surgery. Results indicated that patients with higher social support scores recovered independent mobility 5 days faster on average and reported 30% lower pain levels compared to those with lower social support scores.
These findings best illustrate which concept related to health psychology?
- The placebo effect, in which patient expectations influence health outcomes
- The buffering hypothesis of social support, which suggests that social relationships can protect against the negative effects of stress and promote better health outcomes
- Operant conditioning, in which recovery behaviors are reinforced by social attention
- The medical model, which views health as purely biological without psychological factors
Question 14
Aaron Beck's cognitive theory of depression proposes that negative thoughts and cognitive distortions contribute to the development and maintenance of depressive symptoms. Which of the following is an example of the cognitive distortion known as "overgeneralization"?
- A student who fails one exam concludes, "I fail at everything I attempt and will never be successful"
- A person believes they can read others' minds and know what people think about them
- An individual attributes all positive events to external factors and all negative events to internal factors
- Someone insists they must be perfect in all tasks or else they are a complete failure
Question 15
Longitudinal Study: Researchers conducted a 10-year longitudinal study of 500 adolescents to examine predictors of substance use disorders in young adulthood. Data collected at age 15 included family history of substance use, peer substance use, academic performance, and mental health symptoms. At age 25, participants were assessed for substance use disorders. The study found that adolescents with both a family history of substance use disorders and elevated symptoms of depression were 4.2 times more likely to develop substance use disorders by age 25 compared to those without these risk factors.
This study design is best described as which type of research method?
- Cross-sectional study, because it compares different age groups at one point in time
- Experimental study, because researchers manipulated the independent variables
- Longitudinal study, because researchers followed the same participants over an extended period to examine developmental changes and predictors of outcomes
- Case study, because researchers examined individuals in depth with detailed qualitative analysis
Question 16
Which of the following statements best describes the relationship between physical exercise and mental health based on current psychological research?
- Regular aerobic exercise has been shown to reduce symptoms of depression and anxiety, possibly through increased endorphin release, improved neuroplasticity, and enhanced self-efficacy
- Exercise has no measurable effect on mental health outcomes and should not be recommended as part of treatment plans
- Only high-intensity exercise produces mental health benefits; moderate exercise has no psychological effects
- Exercise is effective only for physical health conditions and has no impact on psychological disorders
Question 17
Treatment Comparison Study: A research team compared three treatment approaches for social anxiety disorder across 180 participants randomly assigned to one of three conditions: (1) cognitive-behavioral therapy (CBT) focused on cognitive restructuring and exposure, (2) medication with an SSRI, or (3) a combination of CBT and medication. Treatment outcomes were assessed using the Liebowitz Social Anxiety Scale at baseline, post-treatment (12 weeks), and 6-month follow-up. Results showed the following mean anxiety scores at 6-month follow-up:
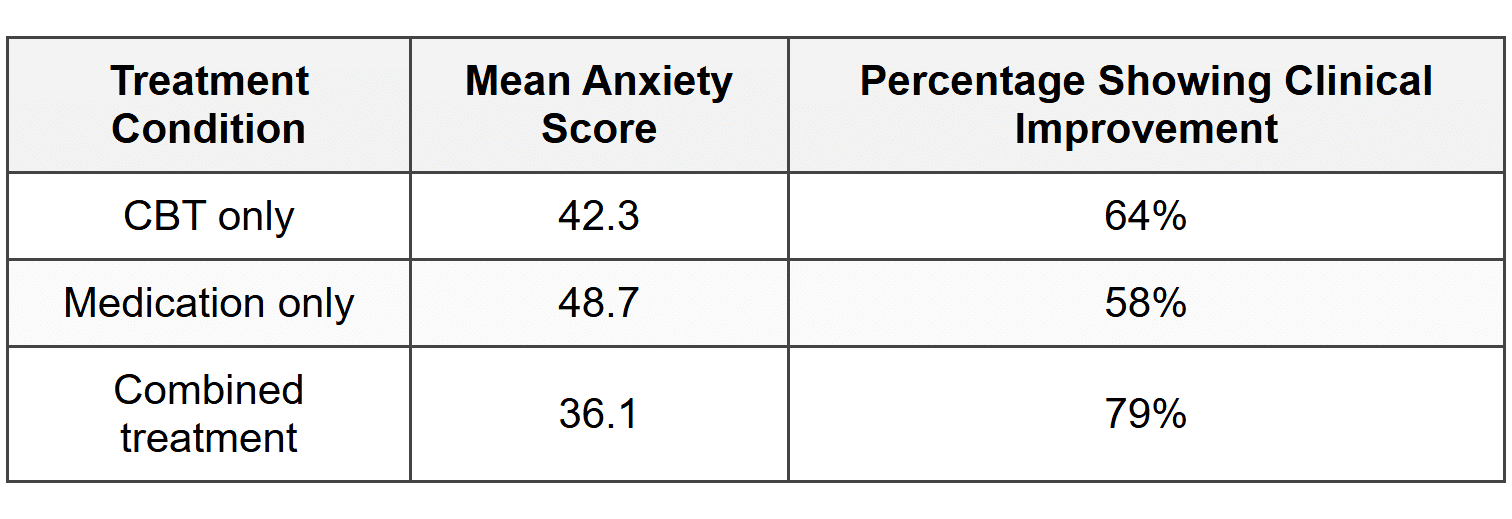
Based on these data, which of the following conclusions is most strongly supported?
- Medication alone is the most effective treatment for social anxiety disorder
- The combination of CBT and medication produced the lowest anxiety scores and highest rate of clinical improvement at follow-up
- CBT is ineffective for treating social anxiety disorder because some participants did not improve
- All three treatments produced identical outcomes, so treatment choice is irrelevant
Question 18
Type A behavior pattern, characterized by competitiveness, time urgency, and hostility, has been associated with increased risk for cardiovascular disease. According to research by Friedman and Rosenman, which specific component of the Type A pattern is most strongly linked to negative health outcomes?
- Time urgency and constant rushing, which elevate heart rate
- Hostility and chronic anger, which promote inflammation and cardiovascular strain
- Competitiveness in achievement settings, which increases motivation
- Perfectionism and attention to detail, which cause cognitive overload
Question 19
Neuroimaging Study: Researchers used functional magnetic resonance imaging (fMRI) to compare brain activity in individuals diagnosed with major depressive disorder to healthy controls while participants viewed emotionally negative images. The study found that participants with depression showed significantly greater activation in the amygdala and reduced activation in the prefrontal cortex compared to controls when processing negative emotional stimuli.
These findings support which explanation of depression?
- Depression results from learned helplessness caused by uncontrollable negative events
- Depression involves dysregulation of neural circuits involved in emotion processing, with heightened limbic reactivity and diminished prefrontal regulatory control
- Depression is caused solely by neurotransmitter deficiencies without structural or functional brain differences
- Depression is entirely psychological with no biological or neural correlates
Question 20
Prevention Program Evaluation: A school district implemented a mental health prevention program for high school students that included psychoeducation about stress management, training in coping skills, and peer support groups. To evaluate program effectiveness, researchers measured anxiety and depression symptoms in 400 students who participated in the program and compared them to 400 students at a similar school that did not implement the program. After one academic year, students who participated in the prevention program showed 23% lower rates of clinically significant anxiety symptoms and 18% lower rates of depressive symptoms compared to the comparison school.
This type of intervention is best classified as which level of prevention?
- Primary prevention, aimed at reducing the incidence of mental health problems before they occur by building protective factors in the general population
- Secondary prevention, focused on early detection and treatment of existing mental health symptoms
- Tertiary prevention, designed to reduce the severity and duration of chronic mental illness
- Crisis intervention, providing immediate support during acute psychological emergencies
SECTION II: FREE RESPONSE
Directions
Answer both questions. Your responses should demonstrate your ability to apply psychological concepts, interpret research findings, and evaluate evidence. Be sure to address all parts of each question. Use complete sentences and appropriate psychological terminology.
FRQ 1: Article Analysis Question (AAQ)
Study Summary:
Dr. Elena Rodriguez and colleagues (2023) investigated the effectiveness of sleep hygiene interventions on mental health outcomes in college students. The researchers recruited 240 undergraduate students (ages 18-22, 60% female, 40% male) from a large public university who reported poor sleep quality and elevated stress levels. Students were recruited through campus flyers and received course credit for participation.
Participants were randomly assigned to one of three conditions: (1) a sleep hygiene education group that received a 90-minute workshop on evidence-based sleep practices including maintaining consistent sleep schedules, limiting screen time before bed, and creating optimal sleep environments (n = 80); (2) a sleep hygiene education plus implementation support group that received the same workshop plus weekly text message reminders and access to a sleep tracking app with personalized feedback for 6 weeks (n = 80); or (3) a wait-list control group that received no intervention during the study period (n = 80).
The dependent variables were operationally defined as follows: Sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI), with scores ranging from 0-21 (higher scores indicate worse sleep quality). Mental health outcomes were assessed using the Depression Anxiety Stress Scales (DASS-21), which produces separate scores for depression, anxiety, and stress symptoms. All measures were administered at baseline and again at 6 weeks.
The study was approved by the university's Institutional Review Board (IRB). All participants provided informed consent after being told about study procedures, potential risks and benefits, and their right to withdraw at any time without penalty. Participants' data were kept confidential using coded identification numbers.
Results:
Statistical analyses revealed significant differences between groups at 6 weeks (p < 0.001). Both intervention groups showed significant improvements in sleep quality and stress levels compared to the control group, with the education plus support condition showing the greatest improvements.
Based on the study summary above, answer the following questions:
- Identify the research method used in this study.
- State the operational definition of sleep quality used in this study.
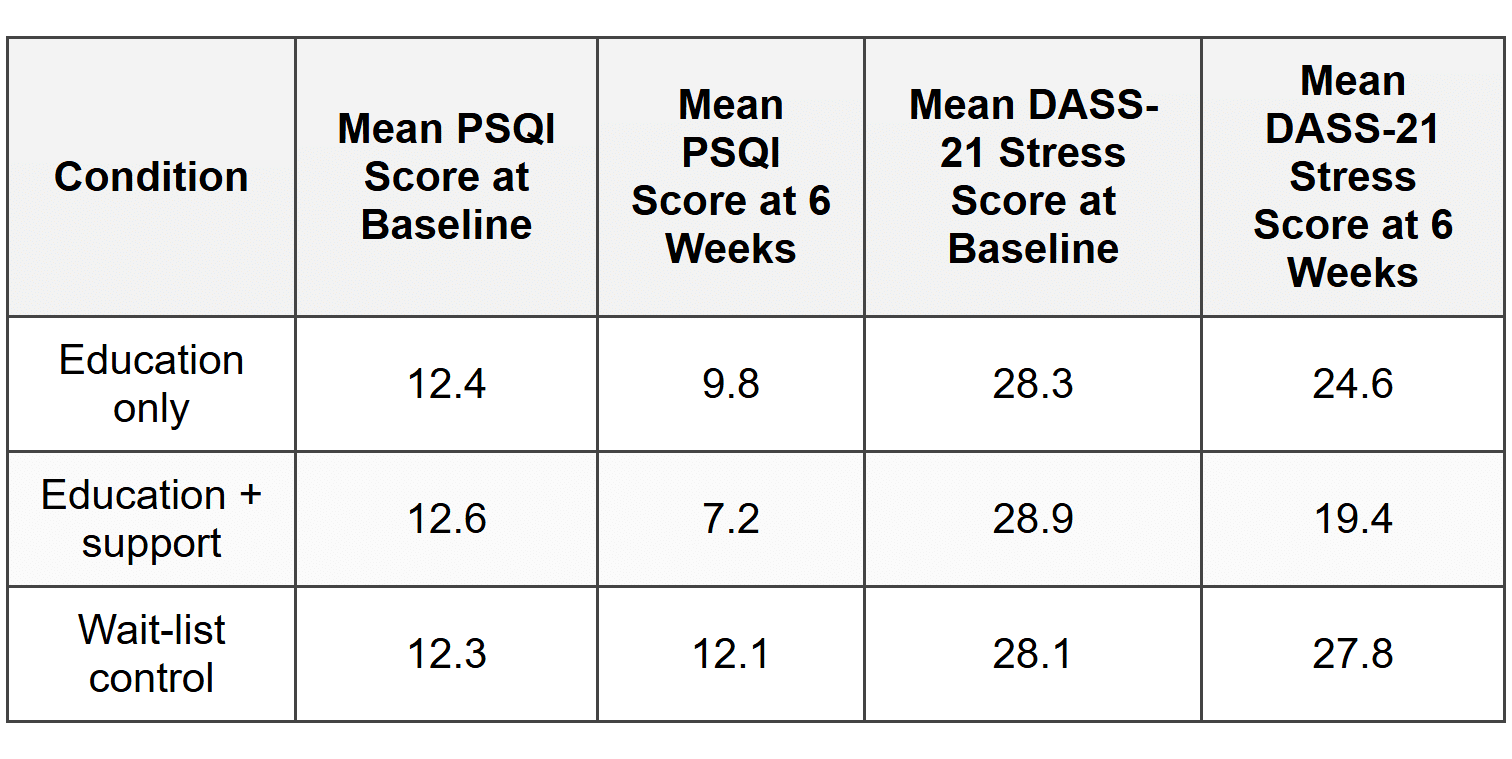
- Describe what the data in the table indicate about the relationship between sleep hygiene interventions and stress levels.
- Identify one ethical guideline that the researchers followed in conducting this study.
- Explain one limitation to the generalizability of the study findings, using specific information from the study description to support your answer.
- Explain how the finding that improved sleep quality was associated with reduced stress supports OR refutes the concept of the biopsychosocial model of health.
FRQ 2: Evidence-Based Question (EBQ)
Read the three study summaries below, then answer the questions that follow.
Study A: Social Support and Recovery from Depression
Thompson et al. (2022) conducted a 6-month longitudinal study of 180 adults receiving treatment for major depressive disorder. Participants completed measures of perceived social support (including emotional support, instrumental support, and social integration) and depressive symptoms at baseline, 3 months, and 6 months. Results showed that individuals with higher levels of social support at baseline demonstrated significantly greater reduction in depressive symptoms over the 6-month period (r = -0.64, p < 0.001). Additionally, participants who reported increases in social support during treatment showed faster recovery trajectories. The researchers concluded that social support may be an important protective factor that enhances treatment response and promotes recovery from depression.
Study B: Cardiovascular Disease and Social Relationships
Chen and Kumar (2021) analyzed data from 4,628 adults (ages 45-85) participating in a national health survey that tracked health outcomes over 10 years. The researchers examined the relationship between social isolation (defined as having fewer than 2 close relationships and limited social contact) and incidence of cardiovascular disease. Results indicated that socially isolated individuals were 1.8 times more likely to develop cardiovascular disease during the follow-up period compared to those with strong social connections, even after controlling for traditional risk factors such as diet, exercise, smoking, and family history. The researchers proposed that chronic social isolation may contribute to cardiovascular disease through sustained activation of stress response systems and inflammation.
Study C: Social Integration and Immune Function
Park et al. (2023) recruited 120 healthy adults and assessed their level of social integration using a standardized measure that evaluated the number and diversity of social roles (e.g., spouse, parent, friend, volunteer, employee) and frequency of social interactions. Participants were then intentionally exposed to a common cold virus in a controlled laboratory setting and monitored for symptom development over 5 days. Results showed that participants with higher social integration scores were significantly less likely to develop cold symptoms despite viral exposure (28% developed symptoms vs. 62% in the low social integration group). Blood samples revealed that socially integrated individuals showed stronger immune responses, including higher natural killer cell activity and lower inflammatory markers.
Based on the three studies above, answer the following questions:
- Identify one commonality shared across all three studies regarding the relationship between social relationships and health.
- Evaluate the consistency of the findings across the three studies. Describe whether the studies support or contradict each other, citing specific evidence from at least two studies.
- Explain how the pattern of findings across these three studies could be understood using the concept of stress and the general adaptation syndrome (GAS). Be sure to identify the specific psychological concept and apply it to the research findings.
ANSWER KEY
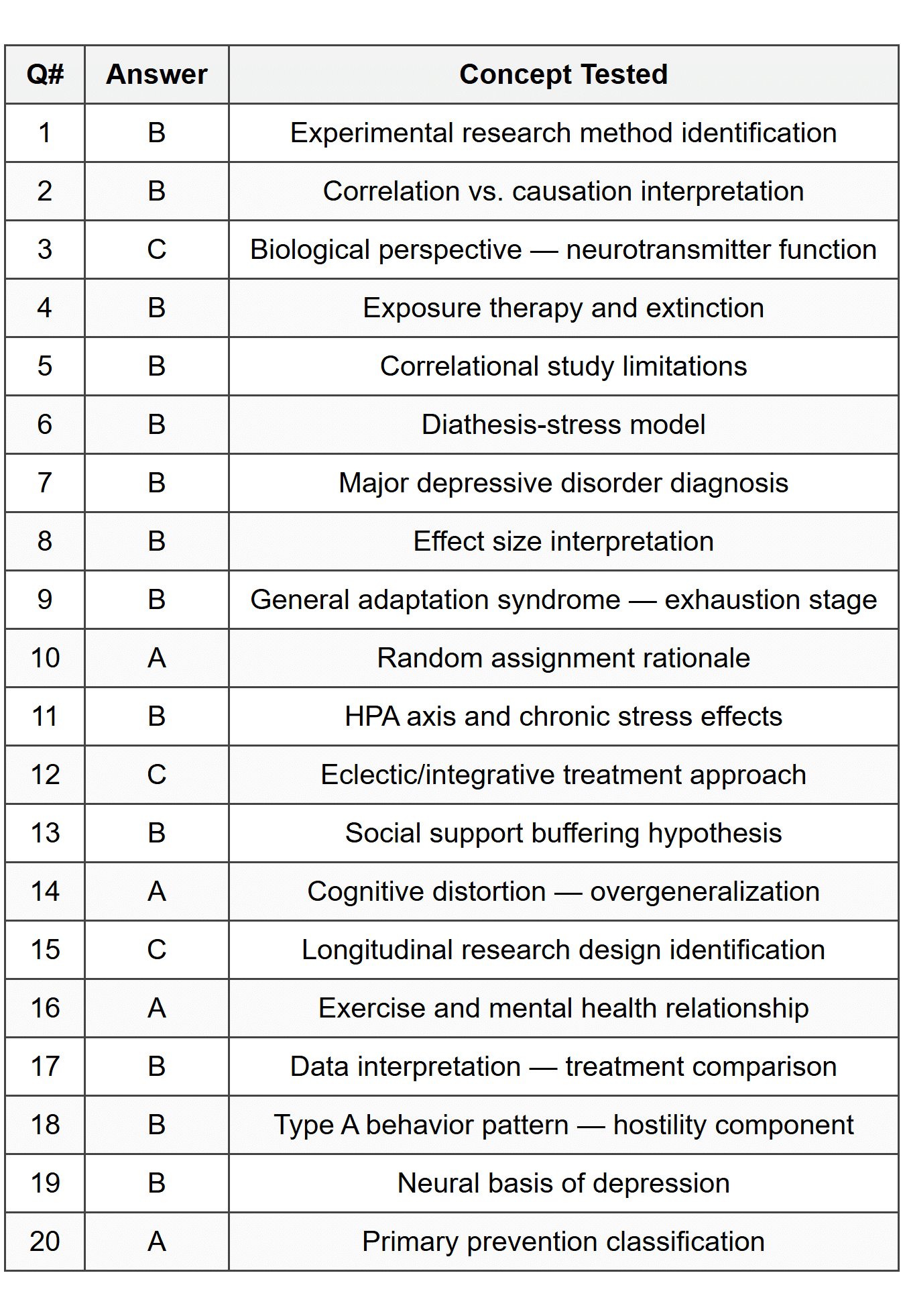
Part A - Multiple Choice Answer Table
Part B - Free Response Detailed Answers
FRQ 1 - Answer Key (Article Analysis Question)
Part A: Identify the research method used in this study.
The research method used in this study was an experiment (or experimental research design). The study qualifies as an experiment because participants were randomly assigned to different conditions (education only, education plus support, or wait-list control), and the researchers manipulated the independent variable (type of sleep hygiene intervention) to observe its effect on the dependent variables (sleep quality and stress levels).
Part B: State the operational definition of sleep quality used in this study.
Sleep quality was operationally defined as scores on the Pittsburgh Sleep Quality Index (PSQI), with scores ranging from 0-21, where higher scores indicate worse sleep quality. This operational definition specifies exactly how the abstract concept of "sleep quality" was measured in concrete, observable terms using a standardized instrument.
Part C: Describe what the data in the table indicate about the relationship between sleep hygiene interventions and stress levels.
The data indicate that sleep hygiene interventions were associated with reduced stress levels. Specifically, the education-only group showed a decrease in mean DASS-21 stress scores from 28.3 at baseline to 24.6 at 6 weeks (a reduction of 3.7 points). The education plus support group showed an even larger decrease from 28.9 to 19.4 (a reduction of 9.5 points). In contrast, the wait-list control group showed almost no change, with scores remaining essentially the same (28.1 to 27.8). The education plus support condition produced the greatest reduction in stress levels, suggesting that providing ongoing implementation support enhances the effectiveness of sleep hygiene education beyond education alone.
Part D: Identify one ethical guideline that the researchers followed in conducting this study.
The researchers followed the ethical guideline of informed consent. According to the study description, all participants were informed about study procedures, potential risks and benefits, and their right to withdraw at any time without penalty before agreeing to participate. Alternatively, acceptable answers include: confidentiality (participants' data were kept confidential using coded identification numbers) or institutional review (the study was approved by the university's Institutional Review Board).
Part E: Explain one limitation to the generalizability of the study findings, using specific information from the study description to support your answer.
One limitation to generalizability is the restricted sample characteristics. The study used only college students ages 18-22 from a single large public university who volunteered in response to campus flyers and received course credit. This convenience sample may not be representative of other populations, such as older adults, individuals not attending college, people from different cultural backgrounds, or those with more severe sleep disorders. Because college students may have different sleep patterns, stressors, and responsiveness to interventions compared to other age groups or populations, we cannot confidently generalize these findings to non-college populations. The fact that participants received course credit may also mean they were more motivated or compliant than individuals who would seek sleep interventions in other contexts.
Part F: Explain how the finding that improved sleep quality was associated with reduced stress supports OR refutes the concept of the biopsychosocial model of health.
The finding that improved sleep quality was associated with reduced stress supports the biopsychosocial model of health. The biopsychosocial model proposes that health and illness result from the complex interaction of biological, psychological, and social factors rather than from biological factors alone. This study demonstrates this integration: sleep is a biological process involving physiological mechanisms, yet it was improved through psychological interventions (education about sleep practices, cognitive changes about sleep hygiene) and behavioral modifications (implementing new bedtime routines, limiting screen time). The resulting improvements in both sleep quality (biological) and stress levels (psychological) illustrate how addressing one domain can produce beneficial effects across multiple systems. Furthermore, the finding that implementation support enhanced outcomes suggests that social and environmental factors (text reminders, app-based feedback) also play important roles in health behavior change, consistent with the biopsychosocial model's emphasis on multiple interacting levels of influence on health.
FRQ 2 - Answer Key (Evidence-Based Question)
Part A: Identify one commonality shared across all three studies regarding the relationship between social relationships and health.
One commonality shared across all three studies is that stronger social connections or social support are associated with better health outcomes. Study A found that higher social support was associated with greater reduction in depressive symptoms; Study B found that social isolation increased risk for cardiovascular disease (or conversely, that strong social connections were protective); and Study C found that higher social integration was associated with stronger immune function and lower rates of illness following viral exposure. All three studies demonstrate that the quality and quantity of social relationships have measurable impacts on physical and mental health.
Part B: Evaluate the consistency of the findings across the three studies. Describe whether the studies support or contradict each other, citing specific evidence from at least two studies.
The findings across the three studies are highly consistent and mutually supportive. Studies B and C both demonstrate that social relationships influence physical health outcomes through similar mechanisms. Specifically, Study B found that socially isolated individuals were 1.8 times more likely to develop cardiovascular disease and proposed that chronic social isolation contributes to sustained activation of stress response systems and inflammation. Study C directly tested immune function and found that socially integrated individuals showed stronger immune responses with lower inflammatory markers. Both studies converge on the conclusion that social isolation or lack of social connection leads to dysregulated physiological stress responses and inflammation, which in turn increase vulnerability to physical disease. Study A extends this pattern to mental health, showing that social support enhances recovery from depression. Together, these studies provide converging evidence that social relationships serve as a protective factor across multiple health domains-mental health (depression), cardiovascular health, and immune function-likely through shared biological pathways involving stress response systems.
Part C: Explain how the pattern of findings across these three studies could be understood using the concept of stress and the general adaptation syndrome (GAS). Be sure to identify the specific psychological concept and apply it to the research findings.
The pattern of findings can be understood through the general adaptation syndrome (GAS), proposed by Hans Selye, which describes the body's physiological response to stress in three stages: alarm, resistance, and exhaustion. According to GAS, prolonged exposure to stressors without adequate recovery leads to the exhaustion stage, in which the body's resources become depleted and vulnerability to illness increases. Social isolation or lack of social support can be understood as a chronic stressor that keeps the body's stress response systems activated over extended periods. Study B explicitly proposed that chronic social isolation leads to sustained activation of stress response systems and inflammation-this represents the resistance stage extending into exhaustion, where continuous physiological arousal eventually depletes adaptive resources and damages cardiovascular health. Study C's finding that socially isolated individuals had weaker immune responses and higher inflammatory markers provides direct evidence of the exhaustion stage: prolonged stress from social isolation has compromised the immune system's ability to respond effectively to pathogens. Study A's findings regarding depression recovery fit this model as well, since depression itself can be understood partly as a consequence of chronic stress exhaustion, and social support may help buffer against stress, preventing or reversing the progression through GAS stages. Conversely, strong social connections provide a buffer that prevents chronic activation of stress systems, allowing individuals to remain in a state of adaptive resistance or to recover effectively from acute stressors, thereby protecting against the health consequences predicted by the exhaustion stage of GAS. Overall, these studies illustrate how social relationships moderate the stress response and influence progression through the stages of GAS, with social isolation promoting chronic stress and exhaustion, and social connection providing protection against stress-related health deterioration.