Chapter Notes: Management of High-Risk Labor - 1

Malpositions
Position: Relationship between the denominator of the presenting part and six reference points on the maternal pelvic brim (right anterior, left anterior, right posterior, left posterior, right lateral, left lateral).Denominator: The part of the presenting part used to describe position. Examples:
- Vertex presentation - occiput is the denominator.
- Breech presentation - sacrum is the denominator.
- Face presentation - mentum is the denominator.
- Shoulder presentation - acromion process is the denominator (in practice the fetal dorsum is used).
- Brow presentation - no fixed denominator is used.
Malposition: The denominator of the presenting part points to a point on the maternal pelvis other than the iliopectineal eminence (that is, not the usual occiput anterior position). Factors that favour malposition include pendulous abdomen in multipara, certain pelvic shapes (anthropoid, android), a flat sacrum, uterine abnormalities and others.
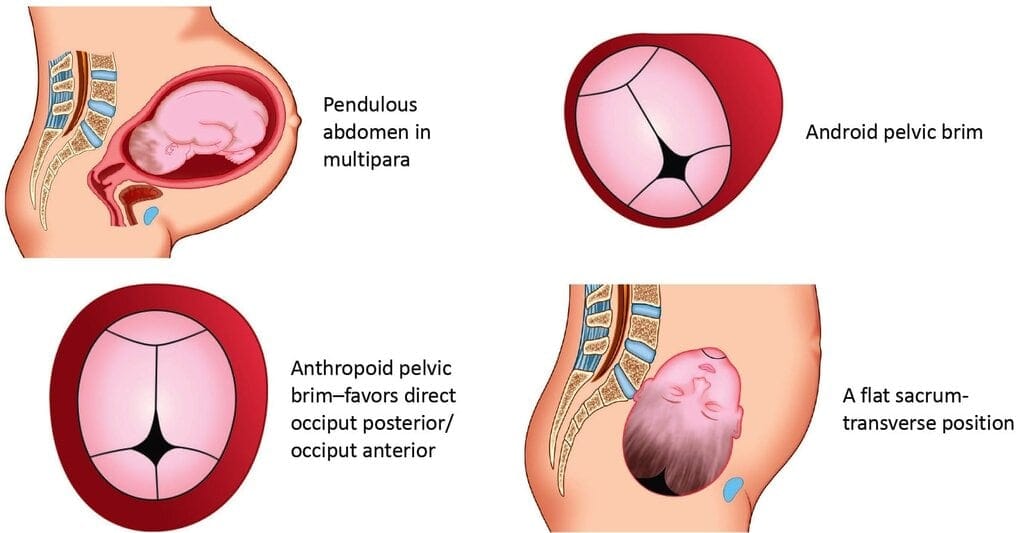 Factors favoring malposition
Factors favoring malposition
Diagnosis of Malposition/Malpresentation
Determine the presenting partThe commonest presenting part is the fetal vertex. If the vertex is not presenting, suspect malpresentation. If the vertex presents, use skull landmarks (fontanelles, sutures, occiput, sinciput, mentum) to determine position.
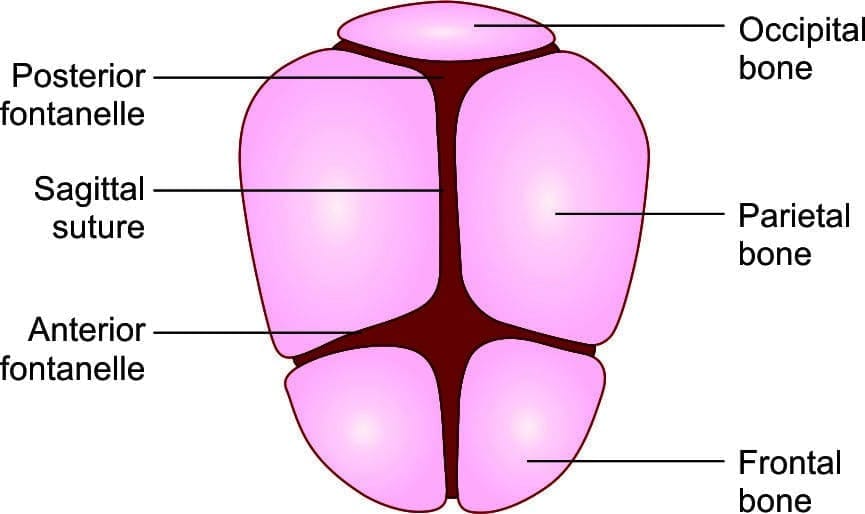 Landmarks of the fetal skull
Landmarks of the fetal skull
Determine the position of the fetal head
Normally the fetal head engages occiput transverse and rotates with descent so the occiput becomes anterior. Failure to rotate from an occiput transverse to occiput anterior should be considered and managed as an occiput posterior position.
Signs of occiput posterior:
- Abdomen: Flattening of lower abdomen, fetal limbs palpable anteriorly; fetal heart may be heard in a flank.
- Vaginal examination: Posterior fontanelle toward sacrum; anterior fontanelle may be easily felt if the head is deflexed.
- If occiput transverse persists late in first stage, manage as occiput posterior.
Malpositions According to Different Presentations
Malpositions in vertex presentation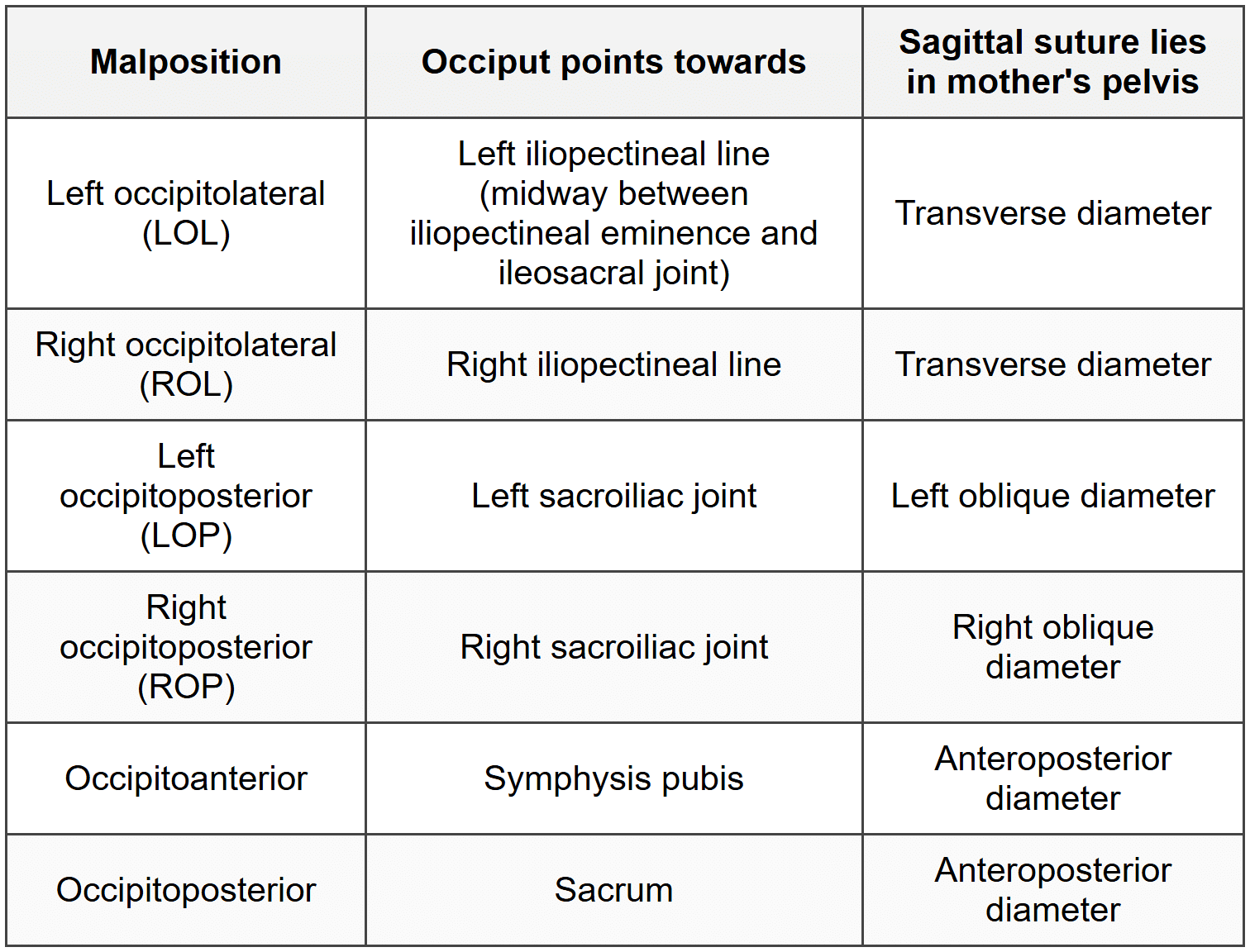
Malpositions in Breech Presentation
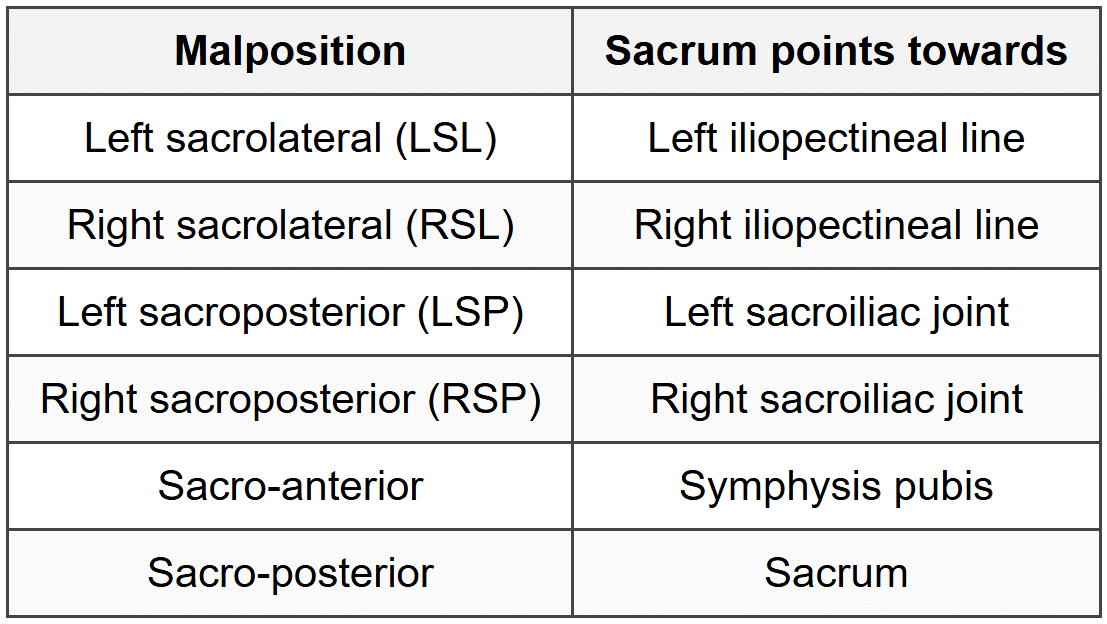
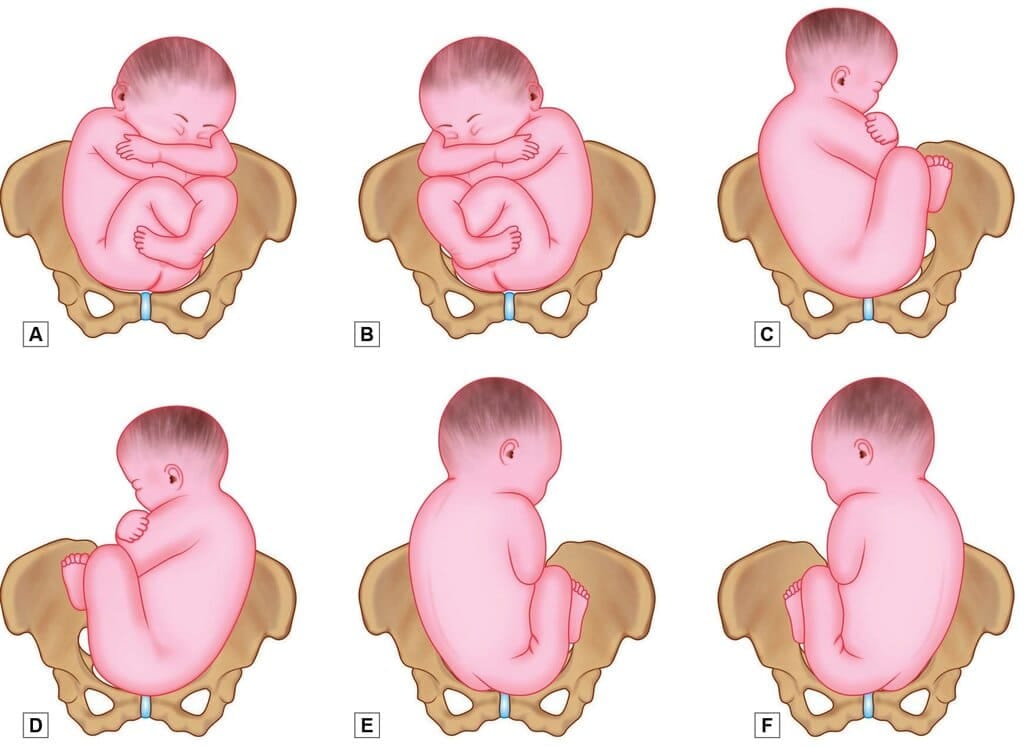 Positions in breech presentation. A. Right sacroposterior; B. Left sacroposterior; C. Right sacrolateral; D. Left sacrolateral; E. Right sacroposterior and F. Left sacroposterior
Positions in breech presentation. A. Right sacroposterior; B. Left sacroposterior; C. Right sacrolateral; D. Left sacrolateral; E. Right sacroposterior and F. Left sacroposterior
Malpositions in face presentation
In face presentation the mentum is the denominator. Positions include:
- Right mentoposterior (RMP)
- Left mentoposterior (LMP)
- Left mentoanterior (LMA)
- Right mentoanterior (RMA)
- Right and left mentotransverse
Malpositions in shoulder presentation
Shoulder presentation uses the fetal dorsum for description. Two common positions:
- Dorsoanterior: Dorsum lies anteriorly (towards iliopectineal eminence and symphysis pubis).
- Dorsoposterior: Dorsum lies posteriorly in the maternal pelvis.
- Malpositions in brow presentation: No fixed denominator is used.
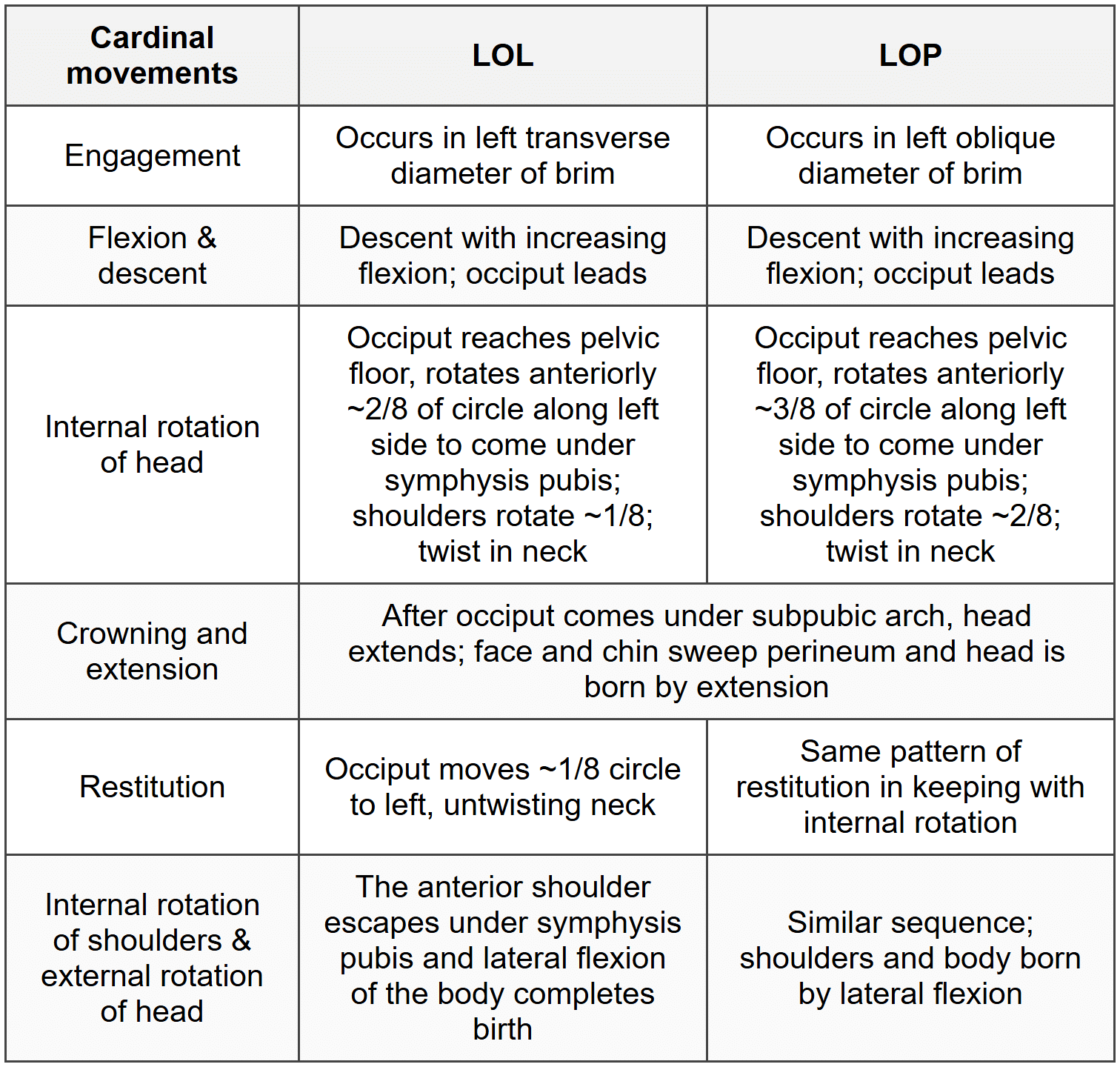
Mechanism of labour in left occipito-posterior and left occipito-lateral positions
Common features for LOL and LOP:- Lie: Longitudinal.
- Attitude: Complete flexion (when well flexed).
- Presentation Vertex; denominator: occiput.
Malpresentation
Malpresentation indicates the presenting part or attitude is other than a well-flexed vertex in longitudinal lie. Common malpresentations are: face, brow, shoulder (transverse lie), breech, compound presentation, and cord presentation.Face presentation
When the fetal head is fully extended so that the face is the presenting part.Incidence: ~0.2% of labours.
Causes:
- Contracted pelvis
- Polyhydramnios
- Fetal congenital abnormalities (e.g., anencephaly, fetal neck masses such as goitre)
- High parity (pendulous abdomen)
Diagnosis: Usually by vaginal examination in labour; may be confused with breech if not carefully examined. Ultrasonography can confirm.
Distribution by mentum position:
- ~60% mentoanterior
- ~15% mentotransverse
- ~25% mentoposterior
Mechanism in mentoanterior face presentation
- Lie: Longitudinal.
- Attitude: Body flexed, head fully deflexed.
- Denominator: Mentum; engaging diameter is submentobregmatic (~9.5 cm).
- Presentation: Face (mentum anterior).
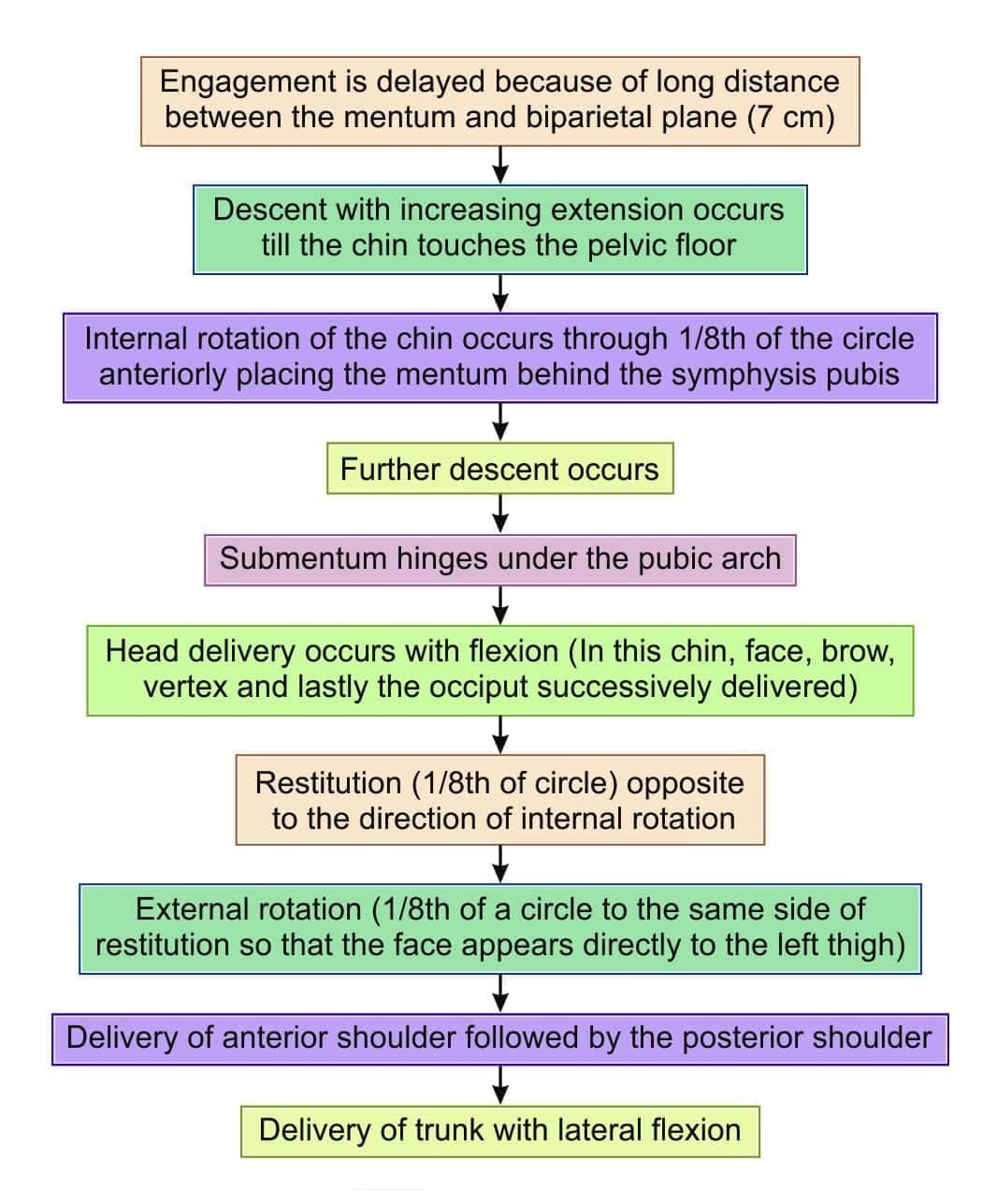 Mechanism of labor in face presentation (Mentoanterior presentation)Mechanism in mentoposterior presentation
Mechanism of labor in face presentation (Mentoanterior presentation)Mechanism in mentoposterior presentation
- Cardinal movements are similar to occiput posterior.
- In about 20-30% the mentum rotates anteriorly allowing vaginal birth; in the remaining 70-80% incomplete rotation, non-rotation or short posterior rotation occurs and there is higher risk of arrest of descent.
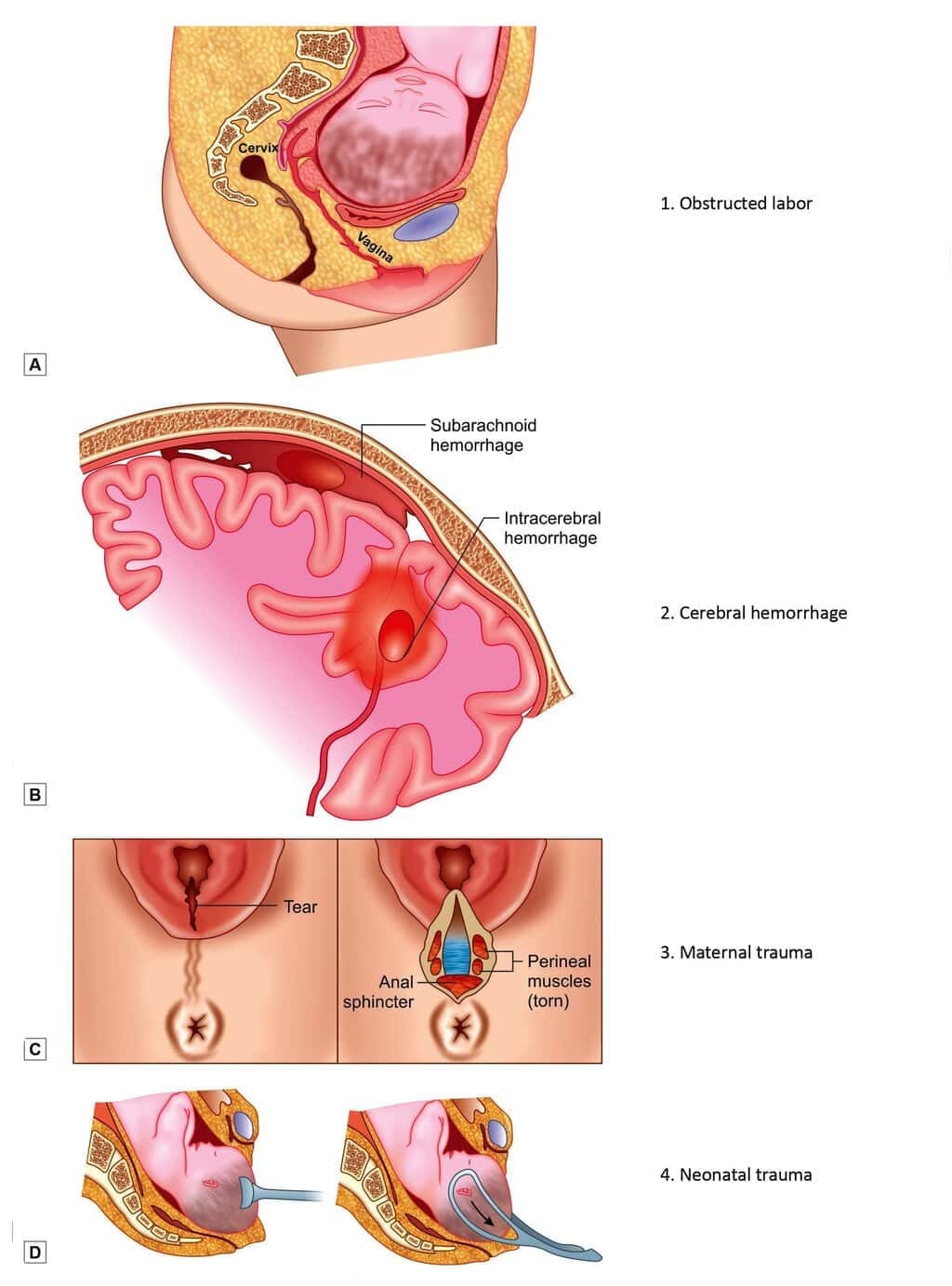
Complications of face presentation
- Obstructed labour (face moulds poorly; minor pelvimetric problems may obstruct)
- Cord prolapse (presenting part may be ill fitting)
- Facial bruising and swelling (oedema of eyelids and lips)
- Cerebral haemorrhage (reduced moulding can cause intracranial injury from compression)
- Increased maternal trauma (perineal laceration, increased operative delivery)
 Complications of face presentationManagement of Face Presentation
Complications of face presentationManagement of Face Presentation
- Confirm diagnosis with ultrasonography to exclude fetal bony or congenital anomalies and to estimate fetal size.
- If the maternal pelvis is adequate and the baby is not disproportionately large, allow labour to proceed with close monitoring and avoid maternal exhaustion.
- If pelvis is contracted or if there are high-risk maternal factors (e.g., elderly primigravida, bad obstetric history), plan caesarean section.
Brow Presentation
Occurs when the head is between full flexion and full extension. The engaging diameter is mentovertical (approximately 13.0-13.5 cm), the largest head diameter.- Causes: Contracted pelvis, uterine obliquity, tumours of the fetal neck, cord round neck, anencephaly, pendulous abdomen, tumours of lower uterine segment.
- Diagnosis: Abdominally more than half the head above symphysis pubis; occiput above the sinciput. Vaginal exam: anterior fontanelle and orbits may be felt.
- Outcome and mechanism: The position may spontaneously convert to vertex or face. If conversion does not occur, there may be no effective mechanism for an average-sized baby in a normal pelvis. Small babies with roomy pelvises and strong uterine contractions may be delivered: the brow may descend, internal rotation leads to flexion and extension with eventual delivery.
- Management
- If diagnosed antenatally and no contraindication, await spontaneous correction until near term (up to about one week before EDD) provided close follow up.
- Elective caesarean section if complicating factors exist (e.g., elderly primigravida, contracted pelvis).
- If diagnosed in labour with mother and fetus stable, caesarean section is preferred.
- If obstructed labour with fetal death, destructive procedures (e.g., craniotomy) may be considered by an experienced practitioner.
Shoulder (transverse lie) presentation
When the long axis of the fetus is perpendicular to maternal spine; the shoulder (or arm) may present. More common in multigravida.Causes: Contracted pelvis, uterine deformities, prematurity, lax abdomen (multipara), polyhydramnios, multiple pregnancy, hydrocephalus, anencephaly, placenta praevia.
Types: Dorsoanterior (dorsum anterior) and dorsoposterior (dorsum posterior).
Diagnosis
- Inspection: Uterus broad and asymmetric; fundal height less than period of amenorrhoea in late pregnancy; transverse abdominal bulge.
- Palpation: Hard, ballotable head in one iliac fossa; breech or small parts on one side; fetal back may be anterior (dorsoanterior) or small parts anterior (dorsoposterior).
- Auscultation: Fetal heart sounds heard well below the umbilicus in dorsoanterior.
- Vaginal exam in labour: An elongated bag of membranes may be felt when membranes intact; after rupture, shoulder landmarks (acromion, scapula, clavicle, axilla, ribs) can be palpated; an arm may prolapse.
- Ultrasonography is diagnostic and shows placental location.
Mechanism and outcome
There is no normal mechanism for spontaneous vaginal birth in transverse lie for an average-size fetus in an average pelvis. Vaginal birth is usually not possible unless conversion to a longitudinal lie occurs or specialised manoeuvres are used (e.g., internal podalic version for non-viable or very small fetuses).
Management
Antenatal
- External cephalic version may be attempted beyond 35 weeks if no contraindication.
- If version fails or is contraindicated, admit at 37 weeks because of risk of PROM and cord prolapse; plan elective caesarean section.
- Vaginal delivery may be considered only for a dead or severely malformed small fetus under controlled conditions (internal podalic version).
Intrapartum
- If transverse lie is detected with intact membranes, a controlled external cephalic version may be attempted followed by controlled amniotomy if successful.
- If membranes have ruptured, examine immediately to detect cord prolapse.
- Immediate caesarean section indicated for cord prolapse, unsuccessful version with labour in progress, or prolonged labour after rupture.
Complications: Cord prolapse, prolapsed arm when impacted, obstructed labour and uterine rupture, fetal death.
Breech Presentation
Definition: The fetal lie is longitudinal and the podalic pole (buttocks or feet) presents at the pelvic brim.Types of breech
- Complete breech (flexed): Thighs flexed on the abdomen, legs flexed at knees; presenting part includes buttocks and often feet alongside.
- Frank breech (extended legs): Thighs flexed, legs extended at knees so only buttocks present. Common in primigravida.
- Footling presentation: One or both feet present at the brim; legs partially extended.
- Knee presentation: Thighs extended but knees flexed so knee presents.
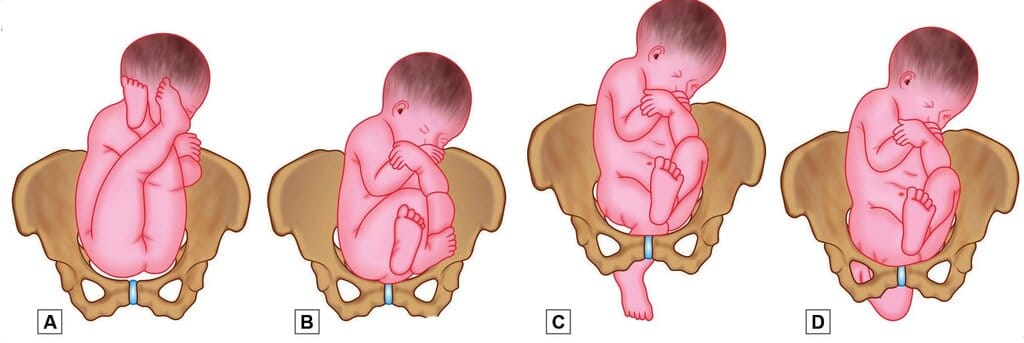 Types of breech presentations. A. Frank breech; B. Complete breech; C. Footling presentation and D. Knee presentationCauses of breech presentation
Types of breech presentations. A. Frank breech; B. Complete breech; C. Footling presentation and D. Knee presentationCauses of breech presentation
- Prematurity (higher incidence before 36 weeks)
- Factors preventing spontaneous version: Multiple pregnancy, oligohydramnios, congenital uterine malformation (septate or bicornuate), short cord, intrauterine fetal death
- Favourable adaptation for breech: Hydrocephalus, placenta praevia, contracted pelvis, cornual-fundal placental insertion
- Undue fetal mobility: Polyhydramnios, multiparity with lax abdominal wall
Diagnosis
- Abdominal palpation: cephalic pole at fundus, podalic pole low.
- Auscultation: fetal heart sound heard above the umbilicus.
- Ultrasonography: confirms presentation.
- Vaginal exam in early labour: presenting part high; slow cervical dilatation; sausage-shaped forewaters; foot may be felt in bag of waters; PROM may occur.
Mechanism of labour in breech (example: left sacro-anterior)
- Lie: Longitudinal; attitude: flexion.
- Denominator: Sacrum (left).
- Presenting part: Anterior (left) buttock; bitrochanteric diameter (~10 cm) engages in left oblique diameter of brim.
- Sequence: Compaction and descent with flexion → internal rotation of buttocks (anterior buttock reaches pelvic floor and rotates) → lateral flexion of body and birth of buttocks → restitution → internal rotation of shoulders → internal rotation and birth of head in flexed attitude.
Types of breech delivery
- Spontaneous breech delivery: Buttocks and trunk born with little assistance.
- Assisted breech delivery: Some assistance required for extended legs, arms or head.
- Breech extraction: Obstetric manipulative delivery performed in emergencies (fetal distress, maternal cardiac disease).
Management of vaginal breech delivery
Preliminaries
- Confirm full cervical dilatation.
- Ensure adequate maternal pelvis clinically or by imaging.
- Empty the bladder and have resuscitative equipment for mother and baby ready.
- Explain and instruct the mother about bearing down efforts; use lithotomy position.
- Delivery should be conducted with obstetrician, neonatologist and anaesthesiologist present to allow immediate intervention if needed.
Delivery of the trunk
- When the presenting part is engaged, shift to labour room and place mother in lithotomy position.
- Prepare sterile field, catheterise bladder and provide appropriate analgesia or anaesthesia (epidural, pudendal block or local infiltration as required).
- Encourage maternal expulsive efforts; buttocks are usually delivered spontaneously.
- Gently avoid undue traction on cord; handle the baby by supporting hips (thumbs over sacroiliac area and fingers on iliac crests).
- If arms are extended, avoid pulling; wait for the next contraction which often delivers arms spontaneously; if necessary, sweep the arm across the chest to bring it down.
Delivery of the shoulders
- Allow the baby to hang by its own weight; uterine contractions usually bring the shoulders down to the pelvic floor where they rotate to AP diameter and are delivered.
- Grasp hips and tilt the baby towards the maternal sacrum to free the anterior shoulder; then lift towards maternal abdomen to deliver posterior shoulder.
- If arms are extended, deliver each arm by inserting a hand into the vagina and sweeping the forearm across the chest.
Delivery of the head
- Allow the baby to hang for 1-2 minutes so the head descends and flexes on the pelvic floor.
- Sagittal suture should be in the anteroposterior diameter; controlled delivery of the head is essential to avoid sudden intracranial pressure changes and cerebral haemorrhage.
Methods to deliver the after-coming head
- Forceps delivery: applied by an obstetrician to achieve controlled delivery of the head.
- Burns-Marshall manoeuvre: allow baby to hang until nape of neck slips under pubic arch, assistant gives suprapubic pressure to flex the head; baby swung up and forward to deliver face and head; suction cleared from mouth and pharynx as required.
- Modified Mauriceau-Smellie-Veit (molar flexion and shoulder traction): baby supported on forearm with fingers over maxillary (molar) bones to maintain flexion; traction directed downwards and backwards while assistant provides suprapubic pressure until nape is under pubic arch, then lift up and forward to complete delivery.
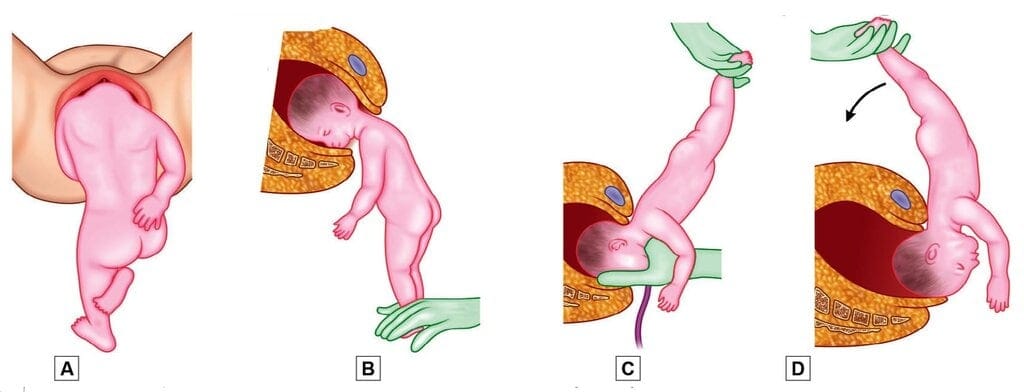 Burns Marshall maneuver. A. Let the baby to hang by its own weight until nape of neck comes under pubic arch; B. Hold his feet; C. With delivery of face and mouth, suction mucus should be performed; D. Swing his head clear
Burns Marshall maneuver. A. Let the baby to hang by its own weight until nape of neck comes under pubic arch; B. Hold his feet; C. With delivery of face and mouth, suction mucus should be performed; D. Swing his head clear
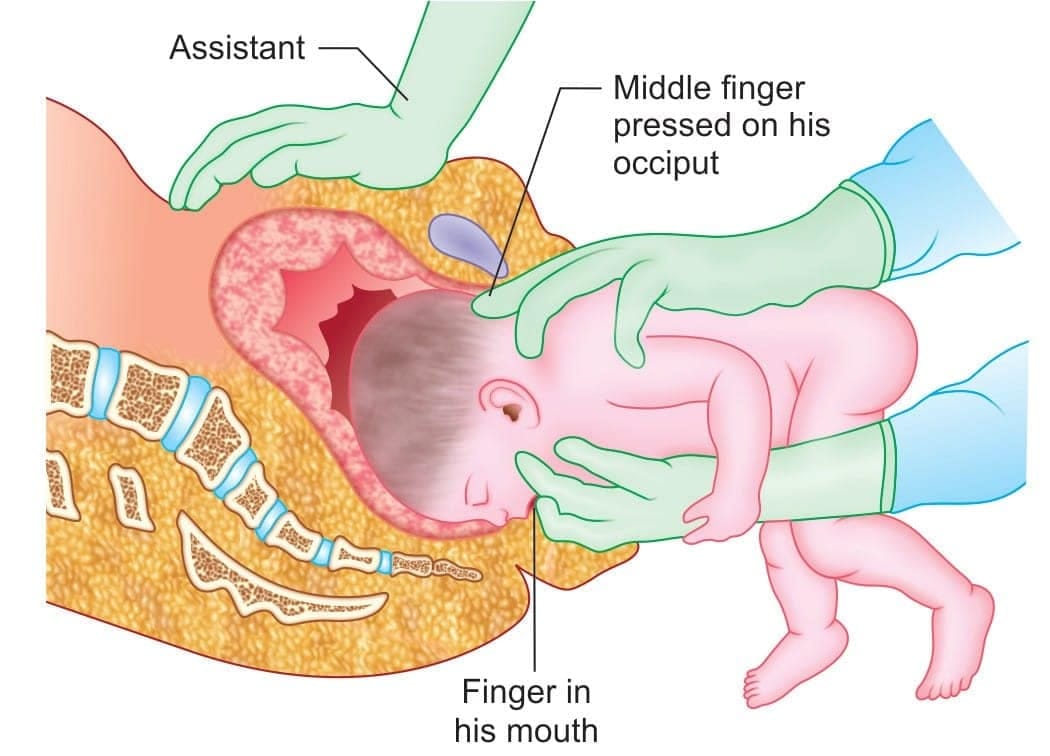 Mauriceau-Smellie-Veit maneuver
Mauriceau-Smellie-Veit maneuver
Delivery of the placenta
The placenta is usually expelled soon after delivery of the head; manage as per active management of third stage.
Care of the newborn
Newborn after breech delivery may be asphyxiated and require resuscitation; otherwise routine newborn care is the same as for vertex presentation.
Compound Presentation
Presence of a hand or foot alongside the head, or both hands by the side of a breech, is called compound presentation. Most common is head with a hand.- Causes: prematurity, pelvic tumours, contracted pelvis, multiple pregnancy, macerated fetus, high head with early rupture of membranes, polyhydramnios.
- Diagnosis: palpation of a limb alongside the presenting part when cervix is dilated.
- Management: Depends on stage of labour, fetal maturity, number of fetuses, pelvic adequacy and cord status. For a live singleton with contracted pelvis or cord prolapse, caesarean section is often indicated. In uncomplicated cases, replacement of a prolapsed limb under general anaesthesia and assisted vaginal delivery may be performed.
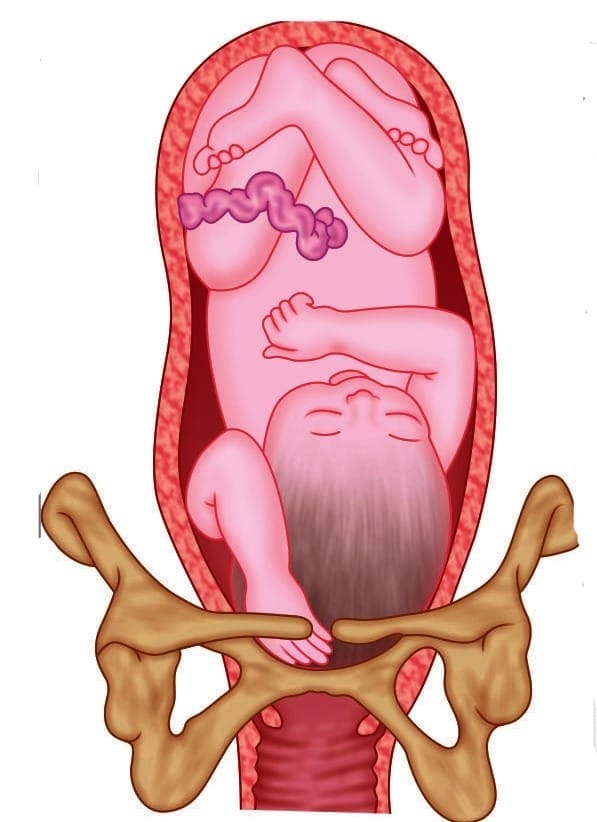 Compound presentation
Compound presentation
Contracted Pelvis
Definition: Alteration in size and/or shape of the pelvis sufficient to alter the normal mechanism of labour for an average-sized baby.Classification of pelvic types
Four classical female pelvic types (many women have mixed features):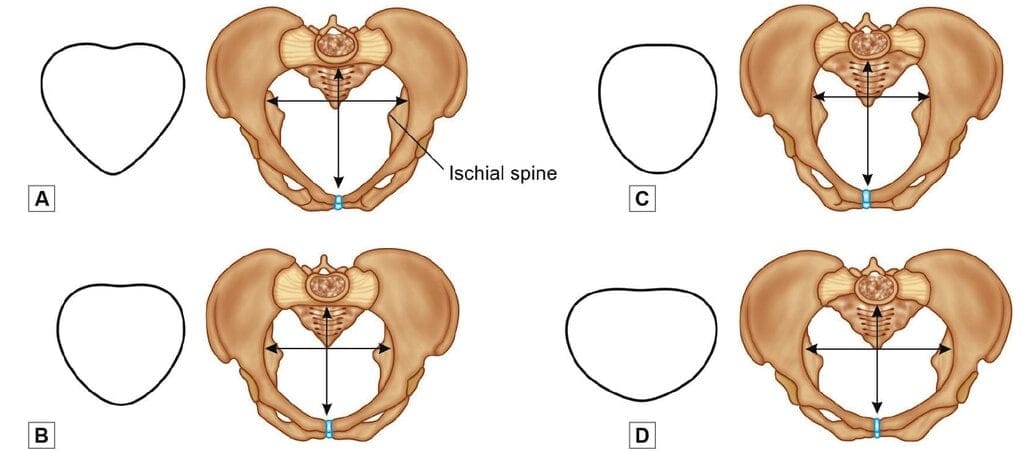 Types of female pelvises. A. Android; B. Gynecoid; C. Anthropoid; D. Platypelloid
Types of female pelvises. A. Android; B. Gynecoid; C. Anthropoid; D. Platypelloid
- Gynecoid (≈50%): Normal female pelvis; inlet slightly transverse oval; sacrum wide; subpubic angle 90°-100°.
- Anthropoid (≈25%): Long anteroposterior diameters, short transverse diameters; sacrum long and narrow; subpubic angle narrow.
- Android (≈20%): Heart-shaped inlet with narrow anterior apex; converging side walls and prominent ischial spines; subpubic angle <90°.
- Platypelloid (≈5%): Flat pelvis with short anteroposterior diameters and wide transverse diameters; sacrosciatic notch narrow; wide subpubic angle.
Asymmetrical pelvises (osteomalacic, Robert's pelvis, scoliotic pelvis, coxalgic pelvis, split pelvis, Naegele's pelvis) are other causes of obstruction.
Causes of Contracted Pelvis
- Nutritional and environmental
- Rickets (vitamin D deficiency in childhood) leading to poor ossification and pelvic deformity.
- Osteomalacia in adults (vitamin D/calcium deficiency) producing an osteomalacic pelvis.
- Diseases or injuries
- Infections or tumours of bones, tubercular arthritis, poliomyelitis, scoliosis, spondylosis, kyphosis.
- Fractures or other pelvic injuries causing deformity.
- Developmental defects
- Naegele's pelvis: Arrested development of one ala of sacrum leading to asymmetry.
- Robert's pelvis: Absence of both alae with sacral fusion to innominate bone.
Signs and Symptoms
- Arrest of the presenting part at the pelvic inlet.
- Abnormal uterine contractions or poor progress of labour.
- Positive Vasten sign (prominent disproportion between fetal head and symphysis pubis).
- Urinary bladder compression signs if severe.
- Edema of cervix and vaginal walls; risk of fistula formation with prolonged obstruction.
- Danger of uterine rupture if lower uterine segment over-distends.
Diagnosis
Diagnosis is clinical supported by imaging. The elements below are important.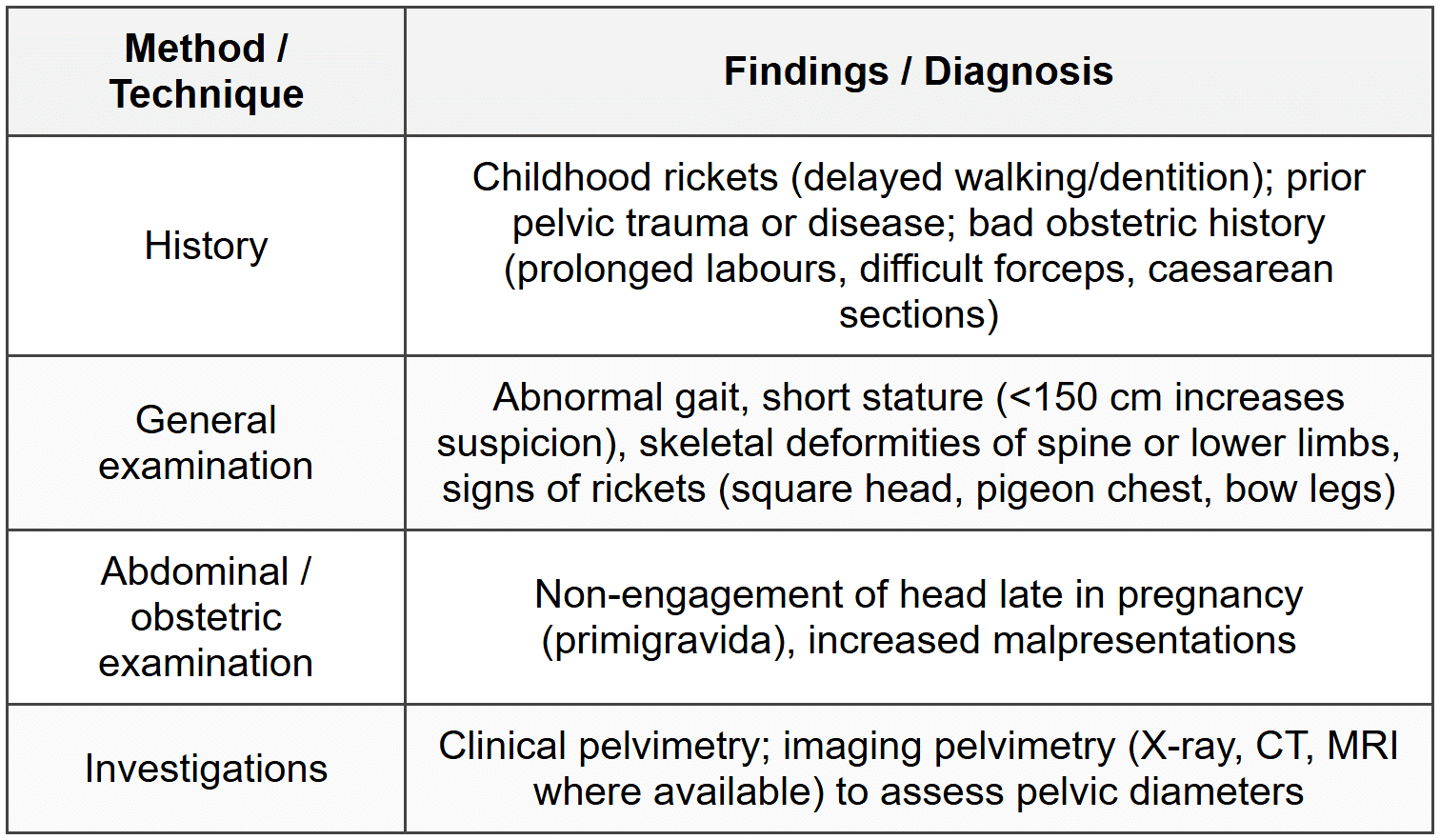
Effects of Contracted Pelvis on Pregnancy/Labor
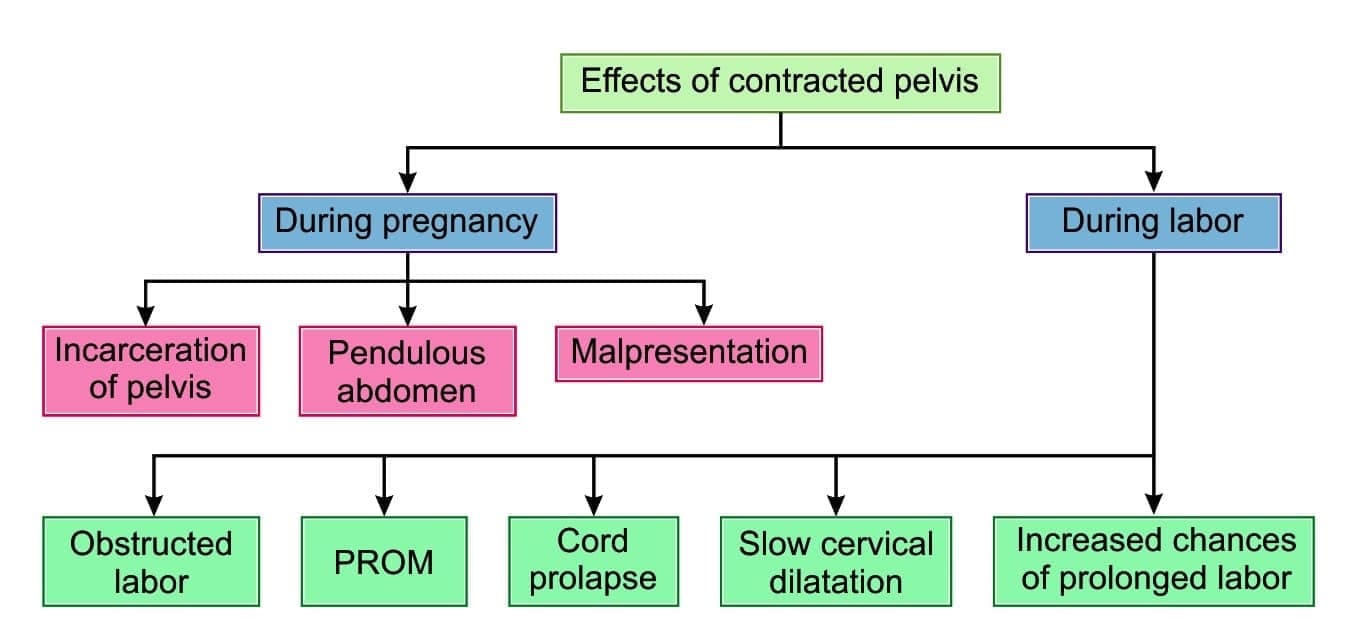 Effects of contracted pelvis on pregnancy or labor
Effects of contracted pelvis on pregnancy or labor
Effects of Contracted Pelvis on Mother and Fetus
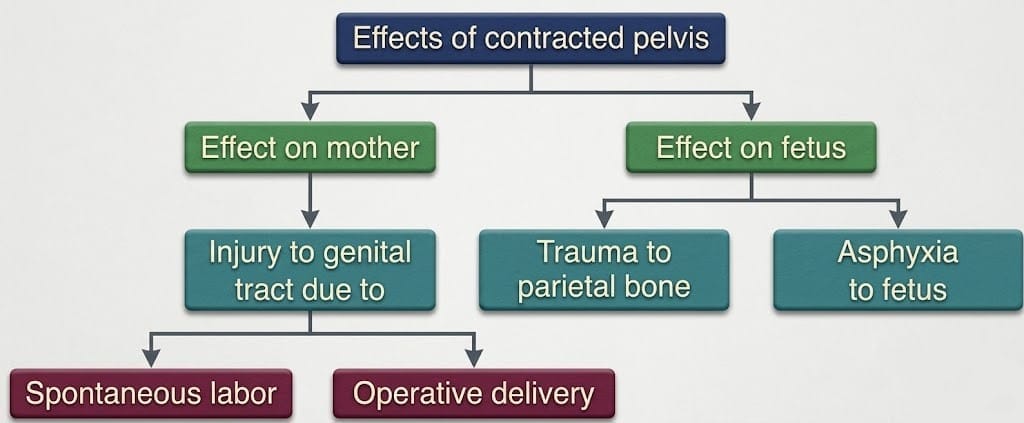 Effects of contracted pelvis on mother and fetus
Effects of contracted pelvis on mother and fetus
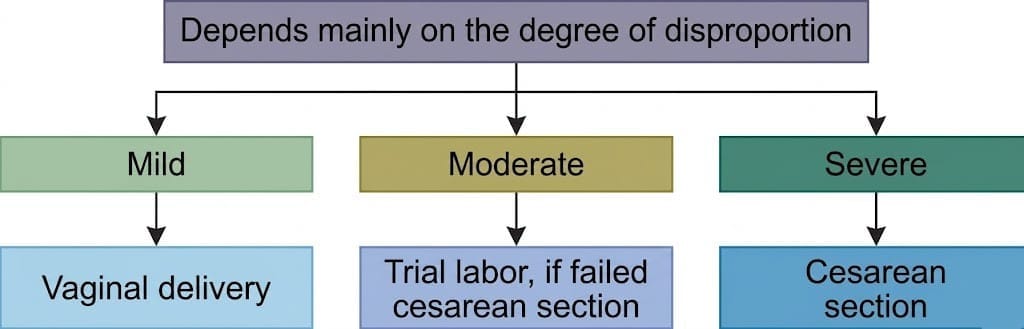
Management of contracted pelvis
- Assess degree of fetopelvic disproportion clinically and with imaging pelvimetry when necessary.
- Minor inlet contraction may allow spontaneous vaginal delivery at term in many cases.
- Moderate or severe inlet contraction requires active management: induction before term, trial of labour or planned caesarean section depending on degree.
- Induction of labour: May be considered earlier than EDD (for example 1-3 weeks earlier) in select moderate contraction to allow delivery of a smaller fetus, provided pelvis and other factors are suitable and close monitoring is available.
- Caesarean section:
- Elective caesarean section is recommended for major disproportion (markedly reduced conjugata vera). A conjugata vera (CV) markedly less than normal (for example CV < 8 cm) is commonly considered major disproportion and a strong indication for elective caesarean.
- Emergency caesarean section when trial of labour fails or when obstruction, fetal distress or uterine rupture is suspected.
- Trial labour: In moderate contraction (example CV ≈ 9 cm) with an average-sized baby (first-degree inlet disproportion), a supervised trial of labour may be offered in an appropriate setting with readiness for immediate operative delivery if the trial fails.
 Trial labor
Trial labor
FAQs on Chapter Notes: Management of High-Risk Labor - 1
| 1. What are malpositions in the context of high-risk labour? |  |
| 2. How does malpresentation differ from malposition? | |
| 3. What is a contracted pelvis and how does it affect labour? | |
| 4. What should be included in the nursing management of high-risk labour? | |
| 5. Why is it important to recognise signs of malpresentation and malposition during labour? | |


