NEET PG Exam > NEET PG Notes > Medicine > CheatSheet: Disorders of Kidney
CheatSheet: Disorders of Kidney


1. Glomerular Diseases
1.1 Classification
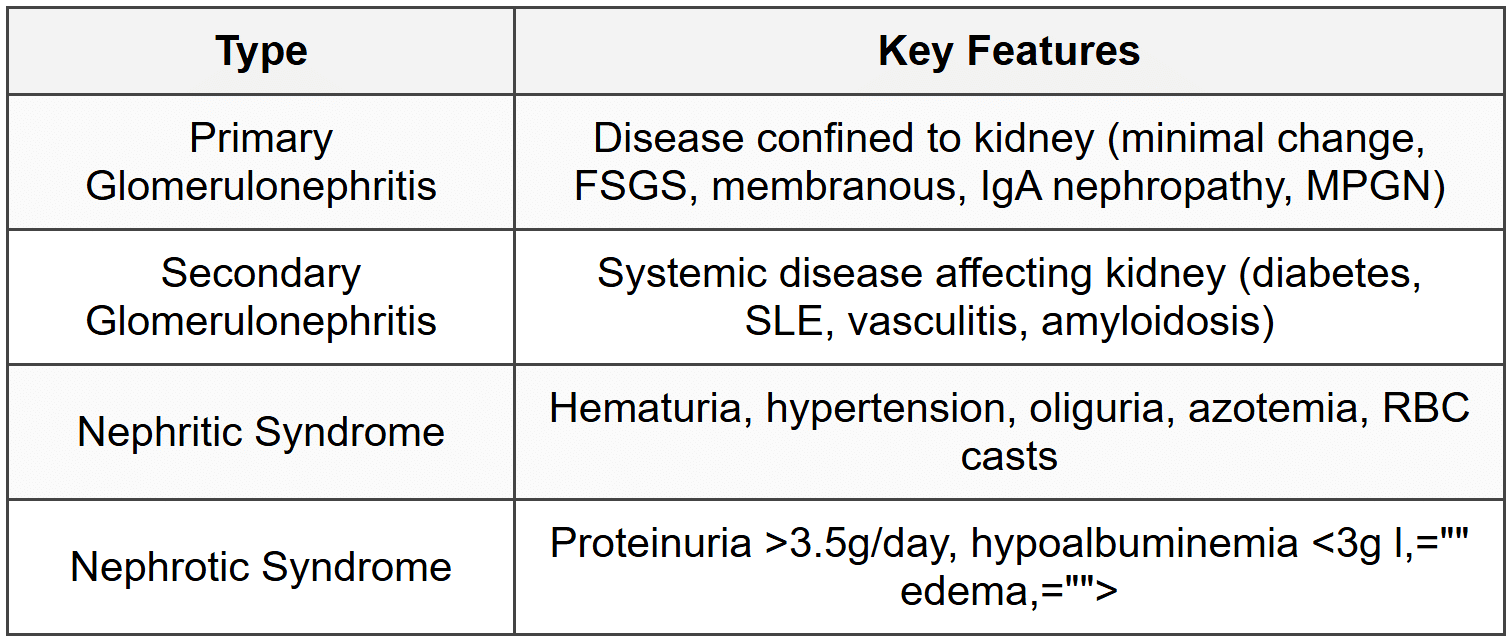
1.2 Minimal Change Disease
- Most common cause of nephrotic syndrome in children (90%)
- Selective proteinuria (albumin only), normal GFR, no hematuria
- Light microscopy: normal glomeruli; EM: podocyte foot process effacement
- Treatment: Corticosteroids - 90% response rate in children
- Associated with Hodgkin lymphoma, NSAIDs
1.3 Focal Segmental Glomerulosclerosis (FSGS)
- Most common primary glomerular disease in adults causing nephrotic syndrome
- Non-selective proteinuria, hematuria, hypertension, progressive renal failure
- Light microscopy: focal and segmental sclerosis; EM: foot process effacement
- Poor response to steroids (20-30%); 50% progress to ESRD in 10 years
- Secondary causes: HIV, heroin, obesity, reflux nephropathy, sickle cell disease
1.4 Membranous Nephropathy
- Most common primary cause of nephrotic syndrome in Caucasian adults
- Anti-PLA2R antibodies in 70% primary cases
- Light microscopy: thickened GBM; IF: granular IgG and C3; EM: subepithelial deposits with spike and dome
- Secondary causes: SLE, hepatitis B, malignancy, NSAIDs, penicillamine
- Rule of thirds: 1/3 remit, 1/3 persistent proteinuria, 1/3 progress to ESRD
- Treatment: ACEi/ARB; immunosuppression if high risk (Cyclophosphamide + steroids or Tacrolimus)
1.5 IgA Nephropathy (Berger Disease)
- Most common primary glomerulonephritis worldwide
- Recurrent gross hematuria within 1-2 days of URTI (synpharyngitic hematuria)
- Mesangial IgA deposition on immunofluorescence
- Henoch-Schonlein Purpura is systemic form with purpura, arthritis, abdominal pain
- Treatment: ACEi/ARB; steroids if proteinuria >1g/day; fish oil
- 25-30% progress to ESRD in 20 years
1.6 Membranoproliferative Glomerulonephritis (MPGN)
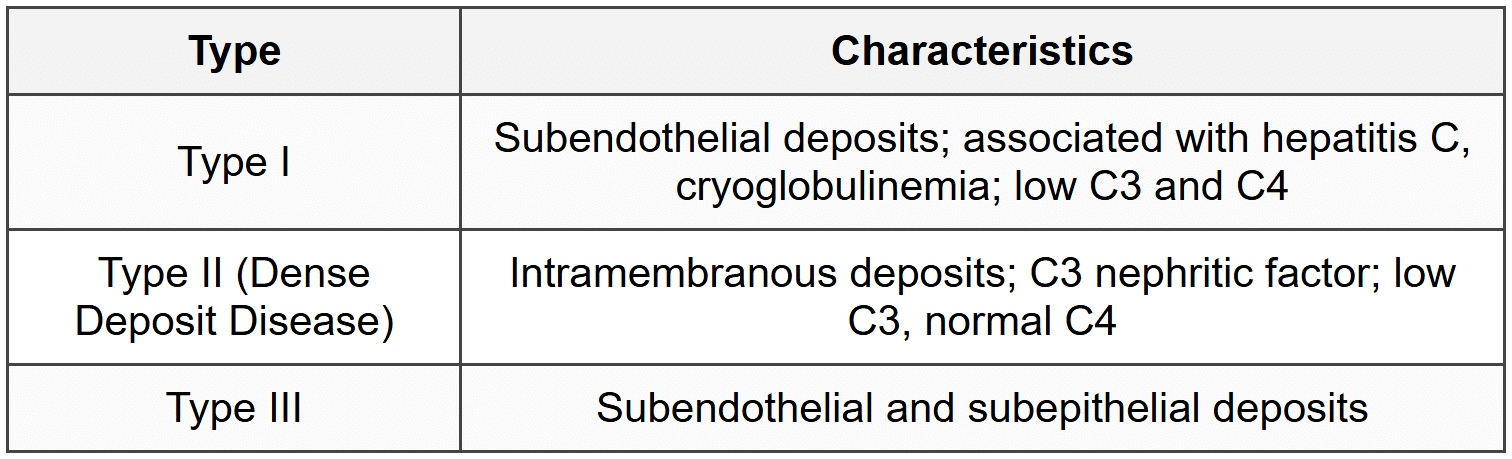
- Tram-track appearance on silver stain; mesangial proliferation
- Mixed nephritic-nephrotic presentation
1.7 Post-Infectious Glomerulonephritis
- Follows group A beta-hemolytic Streptococcus infection (pharyngitis/impetigo) by 1-3 weeks
- Acute nephritic syndrome: hematuria, cola-colored urine, hypertension, edema, oliguria
- Low C3, elevated ASO and anti-DNase B titers
- Light microscopy: diffuse proliferative GN; IF: granular IgG and C3 (starry sky); EM: subepithelial humps
- Self-limited in children (>95% recover); worse prognosis in adults
- Treatment: supportive (salt restriction, diuretics, antihypertensives)
1.8 Rapidly Progressive Glomerulonephritis (RPGN)
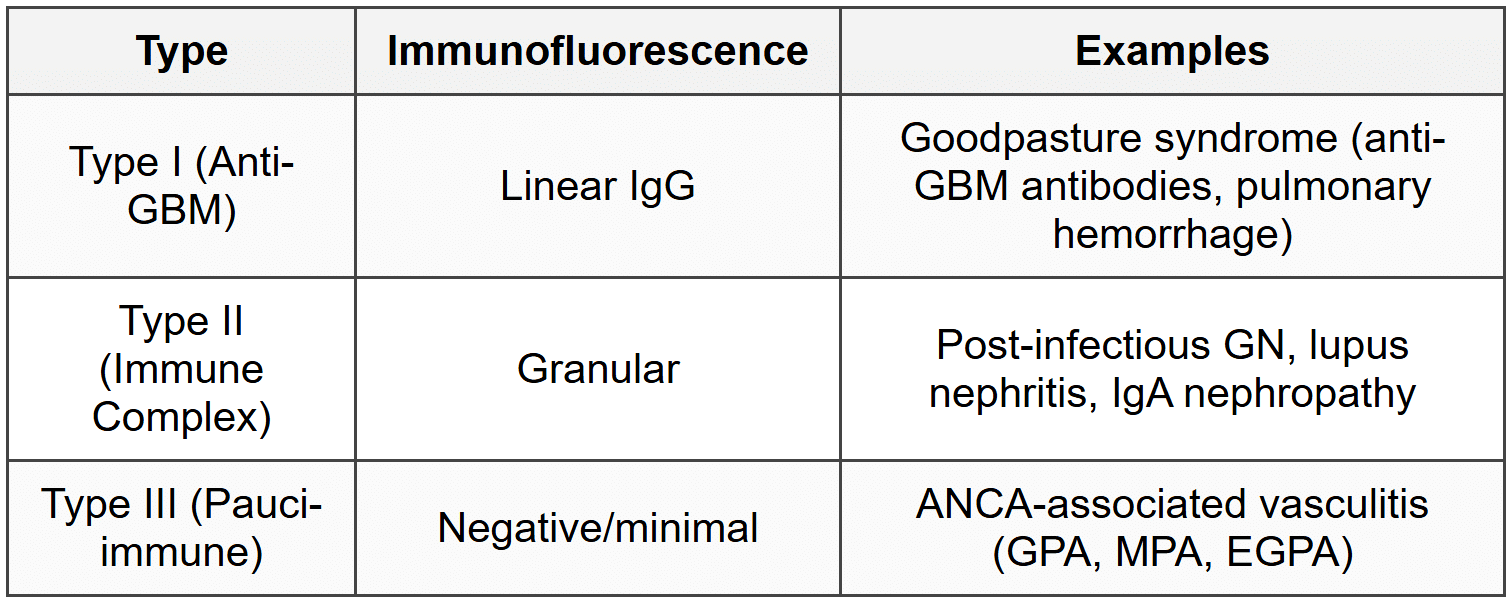
- Hallmark: crescentic GN on biopsy (>50% glomeruli with crescents)
- Rapid decline in GFR over days to weeks; oliguria, hematuria, RBC casts
- Treatment: pulse methylprednisolone + cyclophosphamide; plasmapheresis for anti-GBM disease
1.9 Alport Syndrome
- X-linked dominant mutation in COL4A5 gene (type IV collagen)
- Hematuria, progressive renal failure, sensorineural deafness, ocular abnormalities (lenticonus)
- EM: GBM splitting (basket-weave appearance)
- Males more severely affected; ESRD by 20-30 years
1.10 Thin Basement Membrane Disease
- Benign familial hematuria; autosomal dominant
- Persistent microscopic hematuria, no proteinuria, normal renal function
- EM: diffusely thin GBM (<250>
- Excellent prognosis; no treatment required
2. Tubular and Interstitial Diseases
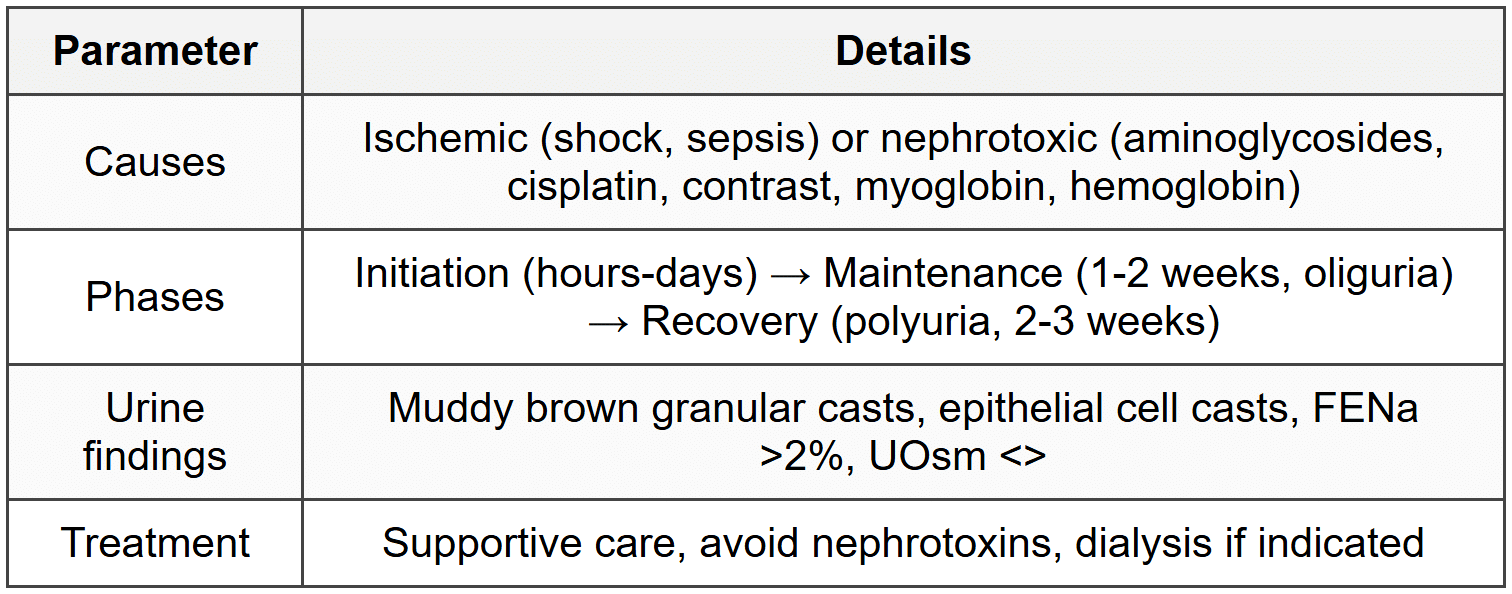
2.1 Acute Tubular Necrosis (ATN)
2.2 Acute Interstitial Nephritis (AIN)
- Causes: drugs (beta-lactams, NSAIDs, PPIs, 5-ASA, allopurinol), infections, autoimmune
- Classic triad: fever, rash, eosinophilia (in <10%>
- Urine: eosinophiluria, WBC casts, sterile pyuria, mild proteinuria
- NSAIDs cause AIN with nephrotic-range proteinuria (minimal change disease)
- Biopsy: interstitial inflammation with eosinophils and lymphocytes
- Treatment: stop offending drug, steroids if severe
2.3 Chronic Interstitial Nephritis
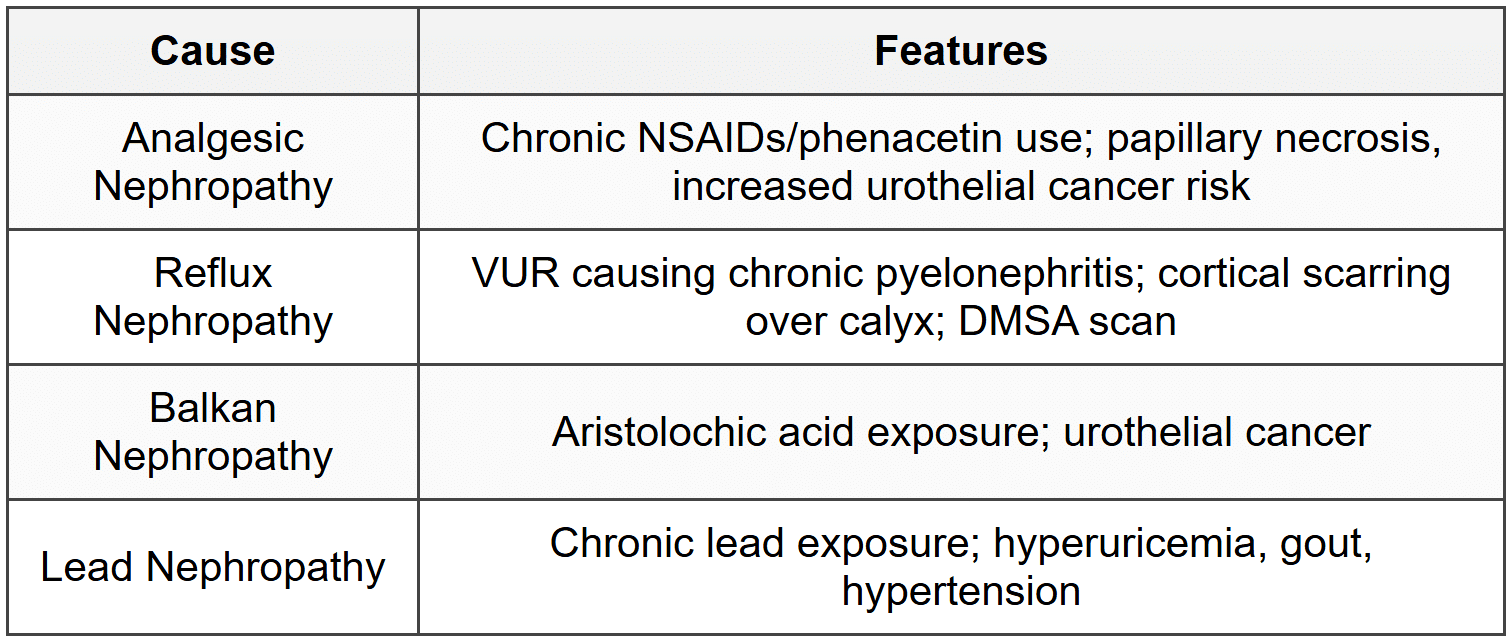
2.4 Renal Tubular Acidosis (RTA)
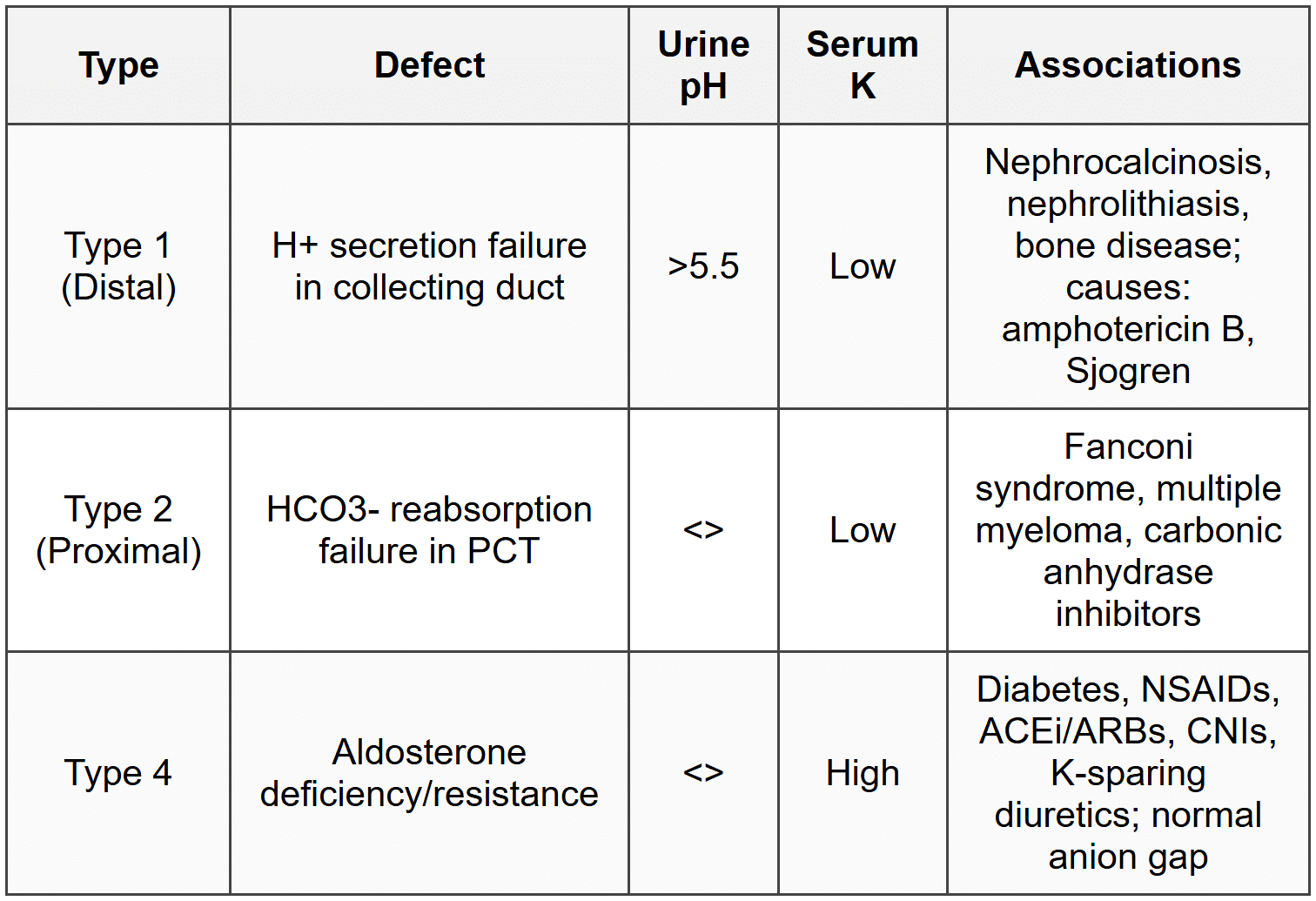
2.5 Fanconi Syndrome
- Generalized PCT dysfunction: aminoaciduria, glycosuria, phosphaturia, bicarbonaturia, uricosuria
- Causes: cystinosis (most common in children), multiple myeloma (adults), ifosfamide, tenofovir
- Rickets/osteomalacia due to phosphate wasting
- Type 2 RTA with hypokalemia
2.6 Bartter and Gitelman Syndromes
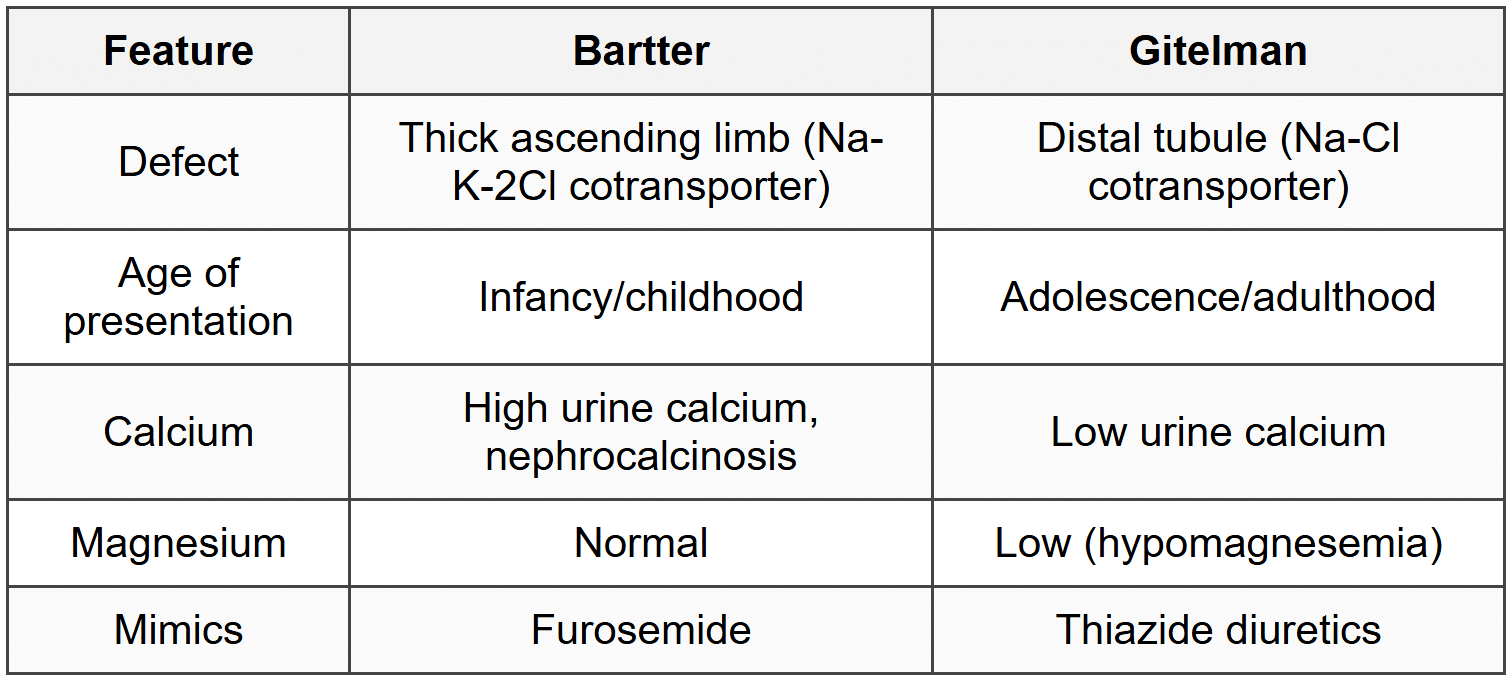
- Both: hypokalemic metabolic alkalosis, hyperreninemia, hyperaldosteronism, normal BP
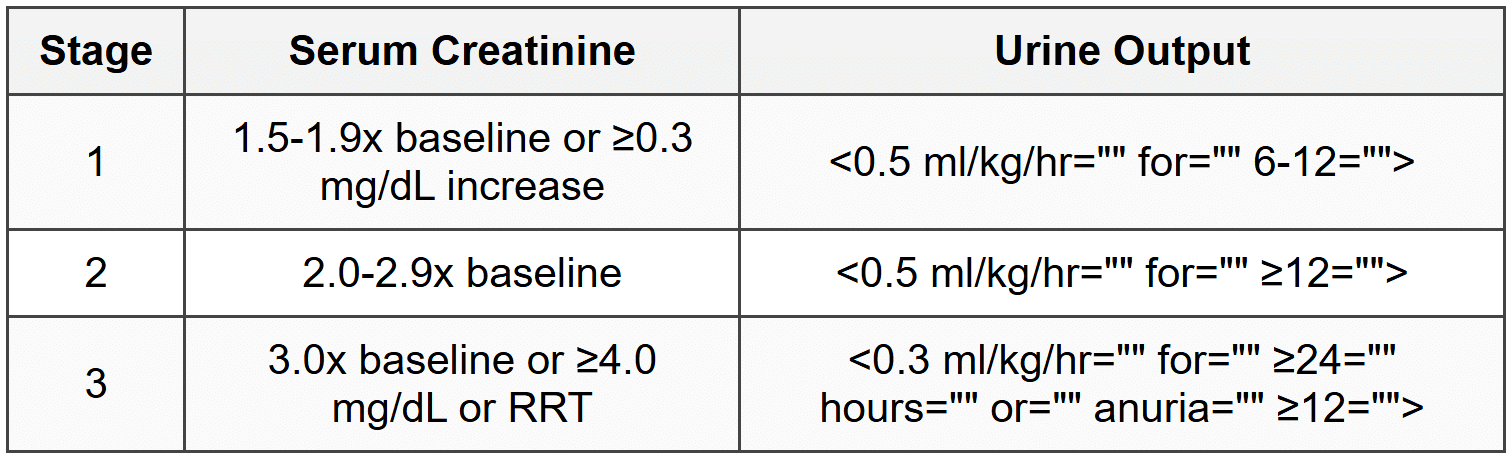
3. Acute Kidney Injury (AKI)
3.1 Definition and Staging (KDIGO)
3.2 Classification
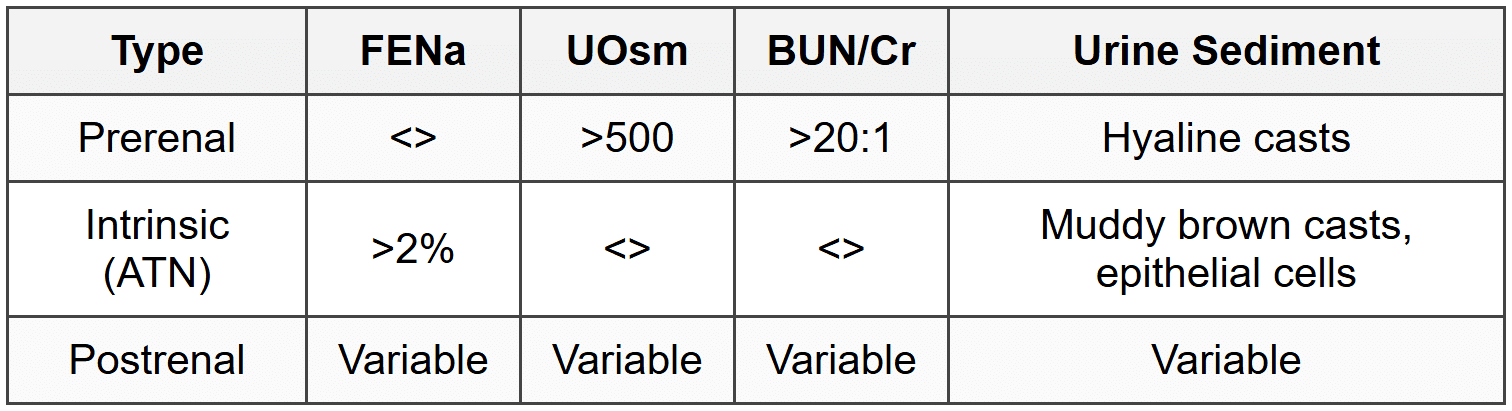
3.3 Prerenal AKI
- Causes: volume depletion (bleeding, GI losses, burns), decreased effective circulating volume (CHF, cirrhosis), renal vasoconstriction (NSAIDs, ACEi/ARBs, HRS)
- Rapidly reversible with volume resuscitation
- If prolonged, progresses to ATN (intrinsic renal failure)
3.4 Intrinsic AKI
- ATN: ischemic or nephrotoxic (see section 2.1)
- Acute interstitial nephritis (see section 2.2)
- Glomerulonephritis: RPGN (see section 1.8)
- Vascular: renal artery thrombosis/stenosis, renal vein thrombosis, atheroembolic disease, TTP/HUS, malignant hypertension
3.5 Postrenal AKI
- Bilateral ureteric obstruction or unilateral in single functioning kidney
- Causes: BPH, prostate cancer, cervical cancer, retroperitoneal fibrosis, bilateral stones, neurogenic bladder
- Diagnosis: ultrasound showing hydronephrosis (may be absent in early obstruction or retroperitoneal fibrosis)
- Treatment: relieve obstruction (catheterization, nephrostomy); watch for post-obstructive diuresis
3.6 Contrast-Induced Nephropathy (CIN)
- Rise in creatinine ≥0.5 mg/dL or ≥25% from baseline within 48-72 hours of contrast
- Risk factors: pre-existing CKD, diabetes, volume depletion, CHF, age >75, contrast volume
- Prevention: IV isotonic saline hydration, minimize contrast volume, hold NSAIDs/diuretics, NAC (controversial)
- Avoid metformin (lactic acidosis risk); restart after 48 hours if renal function stable
3.7 Rhabdomyolysis
- Causes: trauma, prolonged immobilization, seizures, drugs (statins, cocaine), heat stroke, malignant hyperthermia
- Myoglobin causes ATN; serum CK >5000 U/L, hyperkalemia, hyperphosphatemia, hypocalcemia (early), hyperuricemia
- Urine: dipstick positive for blood but no RBCs on microscopy (detects myoglobin)
- Treatment: aggressive IV fluids (200-300 mL/hr), urine alkalinization (sodium bicarbonate), monitor for compartment syndrome
3.8 Tumor Lysis Syndrome
- Massive cell lysis after chemotherapy: hyperkalemia, hyperphosphatemia, hypocalcemia, hyperuricemia
- AKI from uric acid and calcium phosphate precipitation in tubules
- Prevention: allopurinol or rasburicase (preferred if high risk), aggressive hydration, avoid loop diuretics
- Treatment: rasburicase, dialysis if refractory
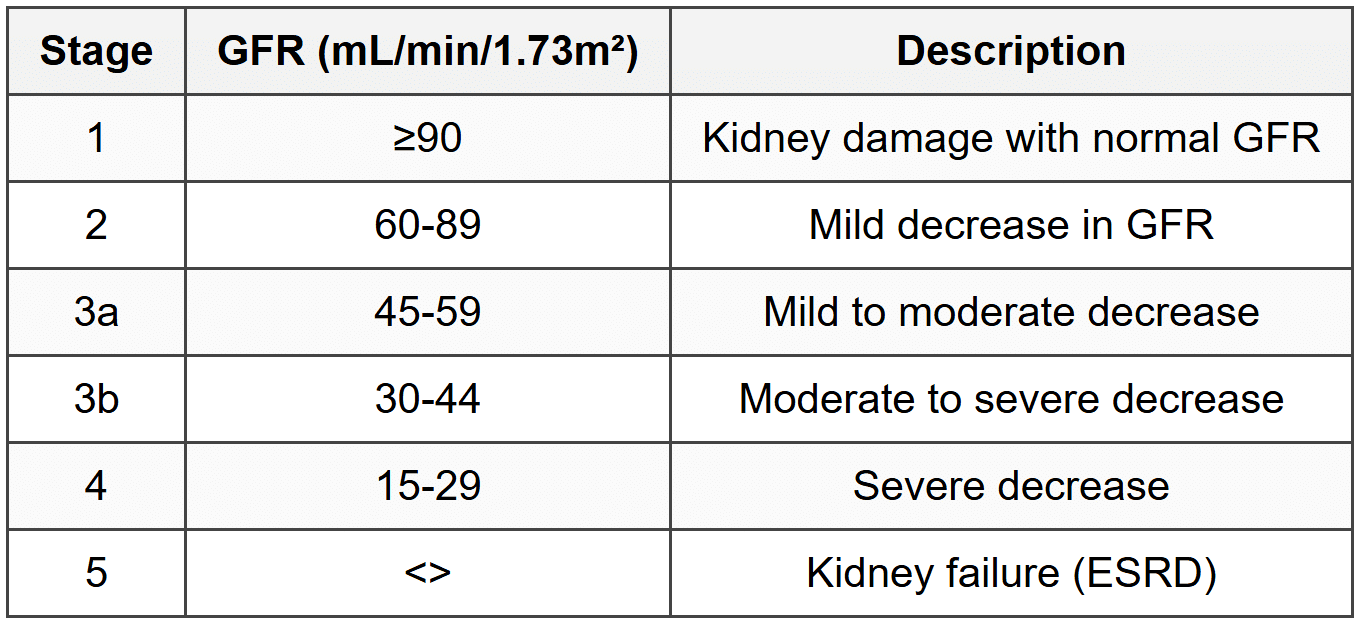
4. Chronic Kidney Disease (CKD)
4.1 Definition and Staging
- CKD: GFR <60 ml/min/1.73m²="" or="" kidney="" damage="" for="" ≥3="">
4.2 Common Causes
- Diabetes mellitus (40%): most common cause
- Hypertension (25-30%)
- Glomerulonephritis (10-15%)
- Polycystic kidney disease
- Chronic interstitial nephritis
4.3 Clinical Features

4.4 CKD-Mineral Bone Disease
- Decreased phosphate excretion → hyperphosphatemia
- Decreased calcitriol production → hypocalcemia
- Secondary hyperparathyroidism → renal osteodystrophy
- Target PTH: 2-9 times upper limit of normal in ESRD
- Treatment: phosphate binders (calcium carbonate, sevelamer), calcitriol, calcimimetics (cinacalcet)
- Adynamic bone disease: oversuppression of PTH
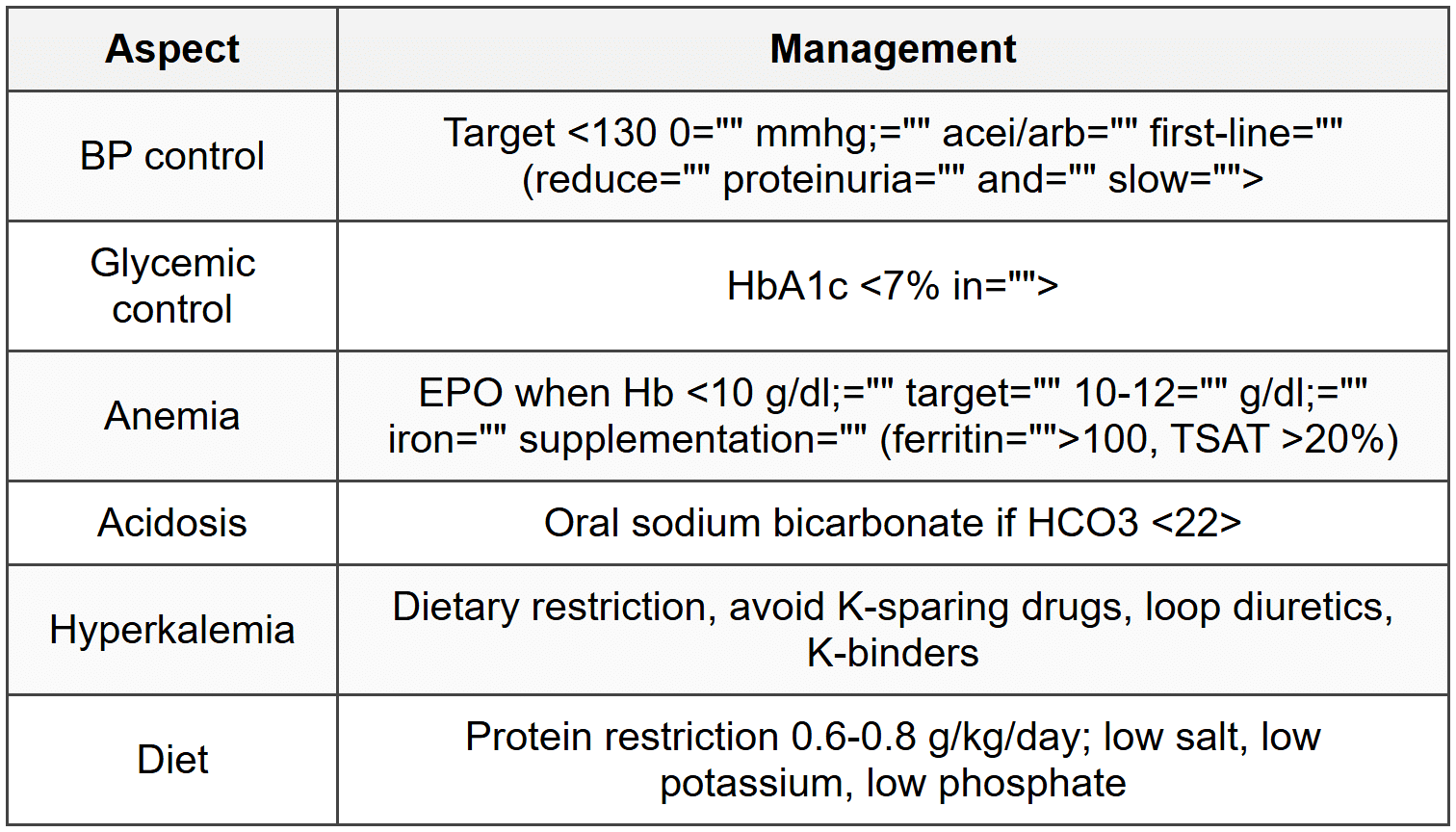
4.5 Management
4.6 Indications for Dialysis (AEIOU)
- A: Acidosis (refractory metabolic acidosis)
- E: Electrolyte abnormalities (hyperkalemia refractory to medical therapy)
- I: Intoxications (methanol, ethylene glycol, lithium, salicylates)
- O: Fluid overload (refractory to diuretics)
- U: Uremia (pericarditis, encephalopathy, bleeding)
- GFR <15 ml/min="" with="" symptoms="" or="" gfr=""><10>
4.7 Uremic Pericarditis
- Indication for urgent dialysis
- Pericardial friction rub, chest pain, ECG changes
- Risk of hemorrhagic pericardial effusion and tamponade
- Does not respond to NSAIDs (contraindicated in CKD)
5. Cystic Kidney Diseases
5.1 Autosomal Dominant Polycystic Kidney Disease (ADPKD)
- Most common inherited cause of ESRD (10% of ESRD cases)
- PKD1 (85%, chromosome 16, worse prognosis) and PKD2 (15%, chromosome 4)
- Bilateral renal cysts, enlarged kidneys, flank pain, hematuria, hypertension
- Extrarenal: hepatic cysts (most common), cerebral berry aneurysms (5-10%), mitral valve prolapse, colonic diverticula
- Screening: MRI brain for aneurysm if family history of SAH or high-risk occupation
- Treatment: BP control (ACEi/ARB), tolvaptan slows cyst growth and GFR decline
- ESRD by 50-60 years
5.2 Autosomal Recessive Polycystic Kidney Disease (ARPKD)
- PKHD1 gene mutation; presents in infancy/childhood
- Bilateral enlarged cystic kidneys, Potter sequence (oligohydramnios → pulmonary hypoplasia, limb deformities)
- Congenital hepatic fibrosis → portal hypertension, varices, splenomegaly
- Poor prognosis; many die in neonatal period
5.3 Medullary Cystic Kidney Disease
- Autosomal dominant; cysts at corticomedullary junction
- Polyuria, salt wasting, progressive renal failure
- Small kidneys (unlike ADPKD)
5.4 Medullary Sponge Kidney
- Benign condition; dilated collecting ducts in medulla
- Nephrolithiasis (calcium stones), hematuria, UTI, nephrocalcinosis
- Normal renal function; IVP shows contrast-filled cystic spaces (bouquet of flowers)
5.5 Simple Renal Cysts
- Very common; increase with age; no clinical significance
- Bosniak classification for characterizing cysts on CT
- Bosniak I-II: benign; Bosniak IIF: follow-up; Bosniak III-IV: surgical exploration (malignancy risk)
6. Vascular Disorders
6.1 Renal Artery Stenosis (RAS)
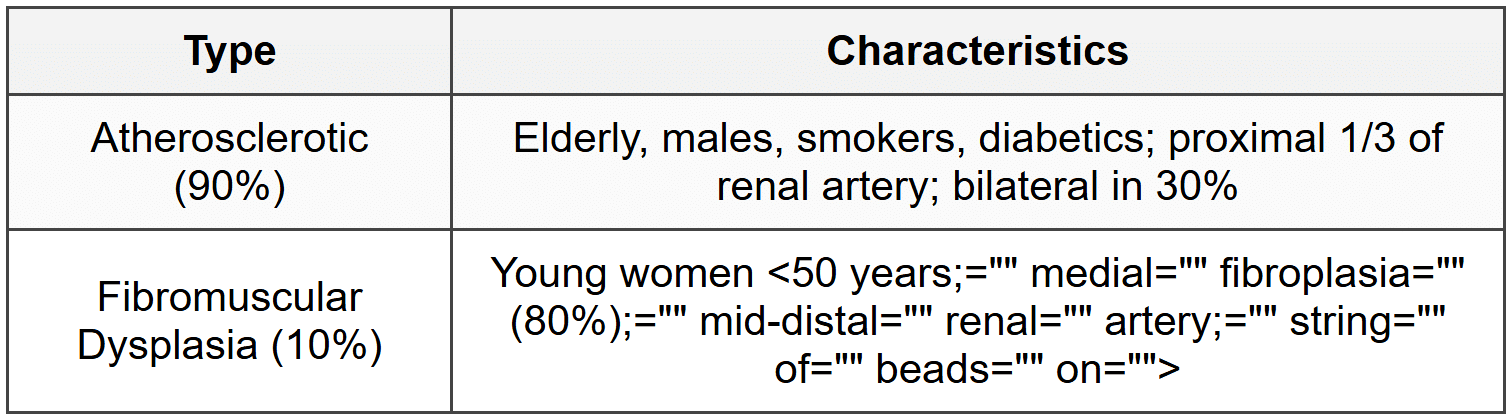
- Clinical clues: resistant hypertension, abdominal bruit, flash pulmonary edema, rise in creatinine >30% after ACEi/ARB
- Diagnosis: Doppler ultrasound (screening), CT/MR angiography, gold standard is renal arteriography
- Captopril renography (decreased use now)
- Treatment: ACEi/ARB for medical therapy; angioplasty for FMD (high cure rate); stenting for atherosclerotic (limited benefit)
6.2 Renal Vein Thrombosis
- Causes: nephrotic syndrome (membranous nephropathy, especially), hypercoagulable states, trauma, malignancy
- Acute: flank pain, hematuria, AKI, left testicular swelling (left-sided)
- Chronic: asymptomatic or worsening proteinuria
- Diagnosis: CT/MR venography, Doppler ultrasound
- Treatment: anticoagulation
6.3 Atheroembolic Disease
- Cholesterol emboli to kidneys after vascular procedure or spontaneous in severe atherosclerosis
- Subacute renal failure (days to weeks post-procedure), eosinophilia, eosinophiluria, hypocomplementemia
- Extrarenal: livedo reticularis, blue toe syndrome, GI ischemia, stroke
- Biopsy: cholesterol clefts in arterioles
- No specific treatment; supportive care; poor prognosis
6.4 Renal Infarction
- Causes: atrial fibrillation (embolic), endocarditis, atherosclerosis, trauma, vasculitis
- Sudden flank pain, nausea, fever, hematuria, elevated LDH
- CT with contrast: wedge-shaped perfusion defect
- Treatment: anticoagulation if embolic; thrombolysis if early presentation
6.5 Malignant Hypertension
- BP >180/120 mmHg with acute end-organ damage (retinopathy, AKI, encephalopathy, cardiac)
- Renal: AKI, hematuria, proteinuria, RBC casts
- Biopsy: acute tubular necrosis, fibrinoid necrosis of arterioles
- Treatment: gradual BP reduction over 24-48 hours; IV labetalol, nicardipine, nitroprusside (avoid in renal failure)
6.6 Scleroderma Renal Crisis
- Acute renal failure with malignant hypertension in systemic sclerosis (diffuse cutaneous)
- Microangiopathic hemolytic anemia, thrombocytopenia
- Risk: anti-RNA polymerase III antibodies, early diffuse skin involvement, corticosteroids
- Treatment: ACEi (captopril) started immediately; dialysis if needed (some recover renal function)
7. Thrombotic Microangiopathies
7.1 Hemolytic Uremic Syndrome (HUS)
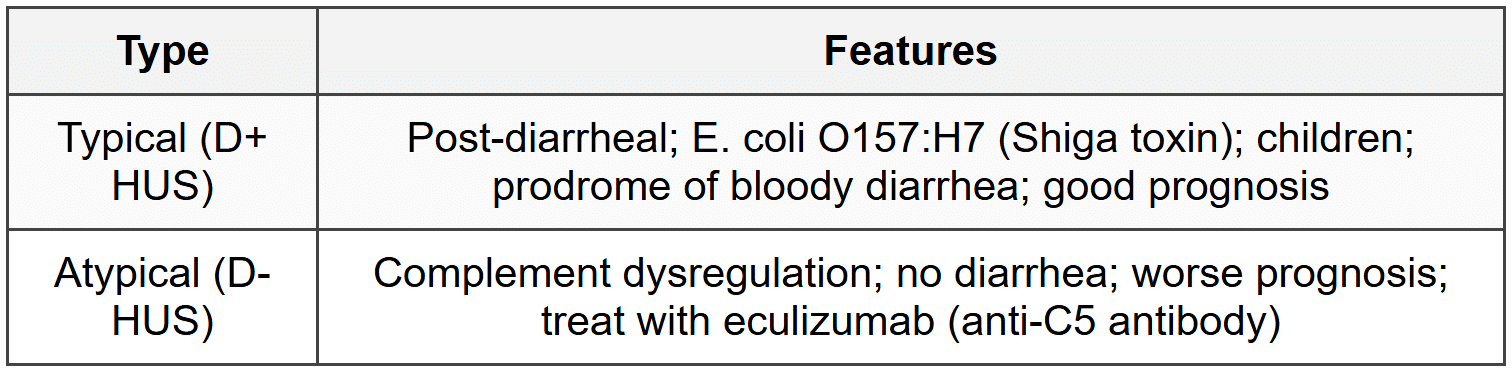
- Classic triad: microangiopathic hemolytic anemia (schistocytes), thrombocytopenia, AKI
- Normal coagulation profile (PT, aPTT), elevated LDH, low haptoglobin, negative Coombs
- Renal manifestations predominate (unlike TTP)
7.2 Thrombotic Thrombocytopenic Purpura (TTP)
- ADAMTS13 deficiency (cleaves vWF); congenital or acquired (autoantibodies)
- Pentad: microangiopathic hemolytic anemia, thrombocytopenia, AKI, neurologic symptoms, fever
- Neurologic manifestations predominate (headache, confusion, seizures, stroke)
- ADAMTS13 activity <>
- Treatment: plasma exchange (first-line), rituximab, caplacizumab (anti-vWF); avoid platelet transfusion
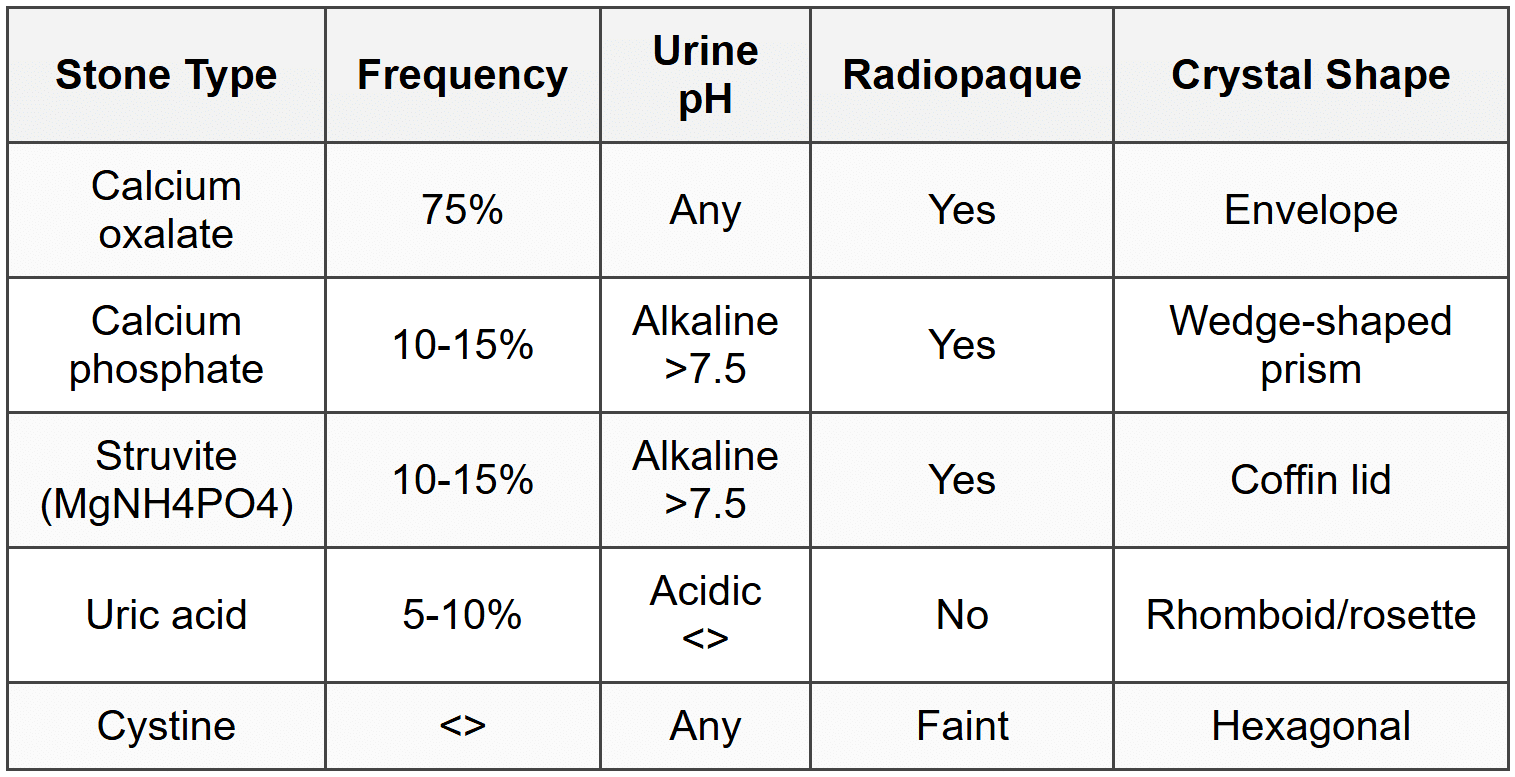
8. Nephrolithiasis
8.1 Stone Types
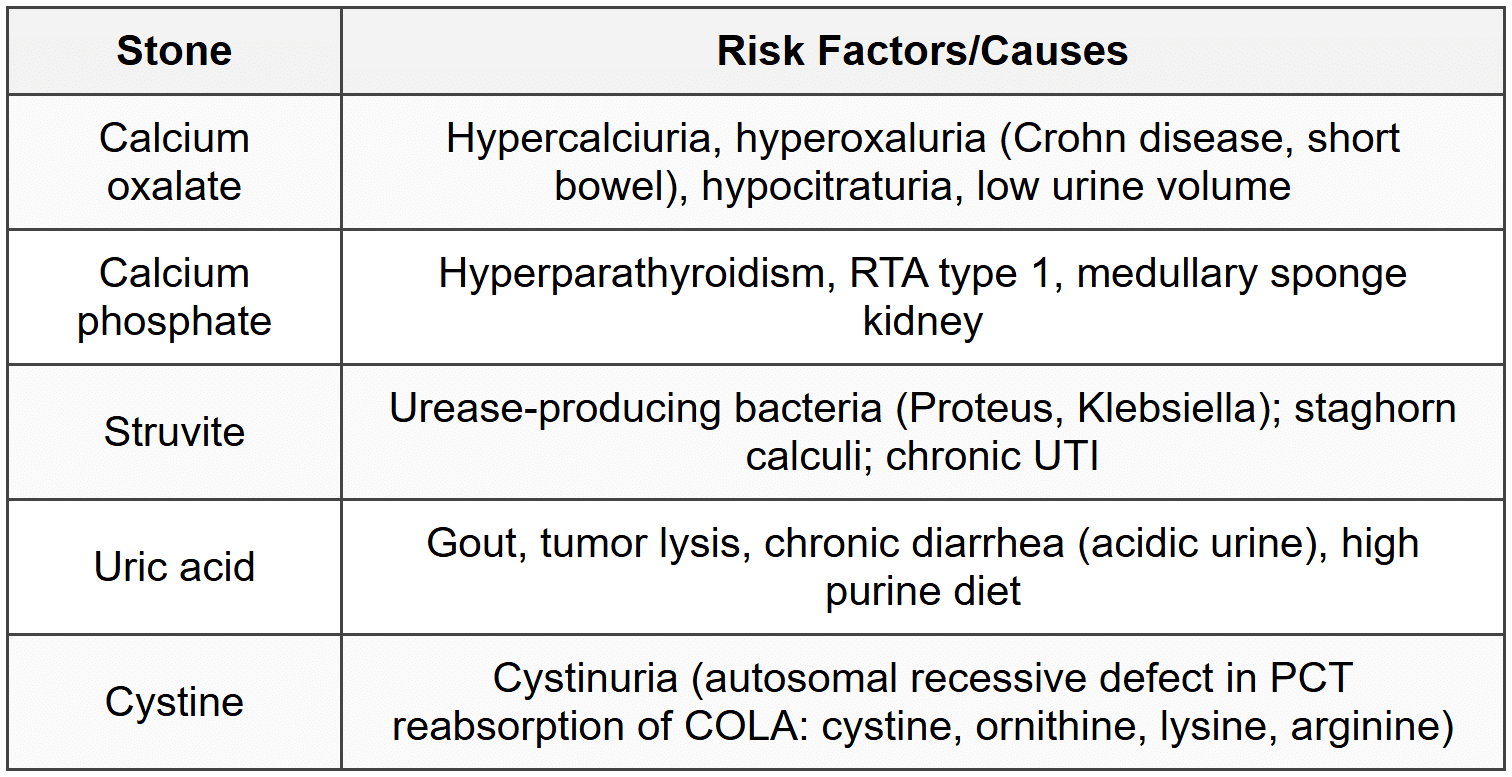
8.2 Risk Factors and Causes
8.3 Clinical Presentation
- Acute renal colic: sudden severe flank pain radiating to groin, nausea, vomiting, restlessness
- Hematuria (90% cases), UTI, hydronephrosis, AKI (if bilateral obstruction)
- Diagnosis: non-contrast CT KUB (gold standard); ultrasound in pregnancy
8.4 Management
- Acute: NSAIDs for pain, hydration, medical expulsive therapy (tamsulosin) for stones 5-10 mm
- Indications for intervention: stone >10 mm, obstruction with infection (emergency), intractable pain, AKI
- Procedures: ESWL (stones <20 mm),="" ureteroscopy,="" pcnl="" (large/staghorn="">
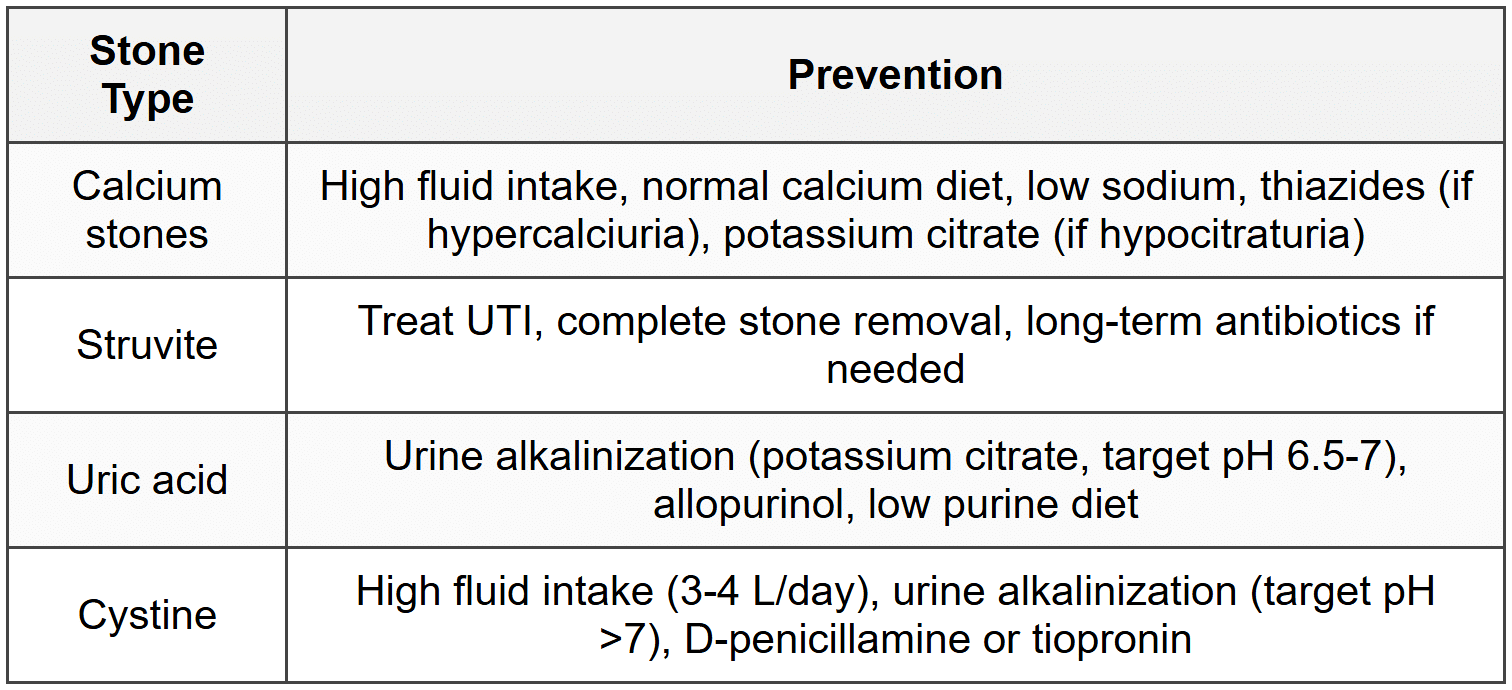
8.5 Prevention
9. Diabetic Nephropathy
9.1 Stages
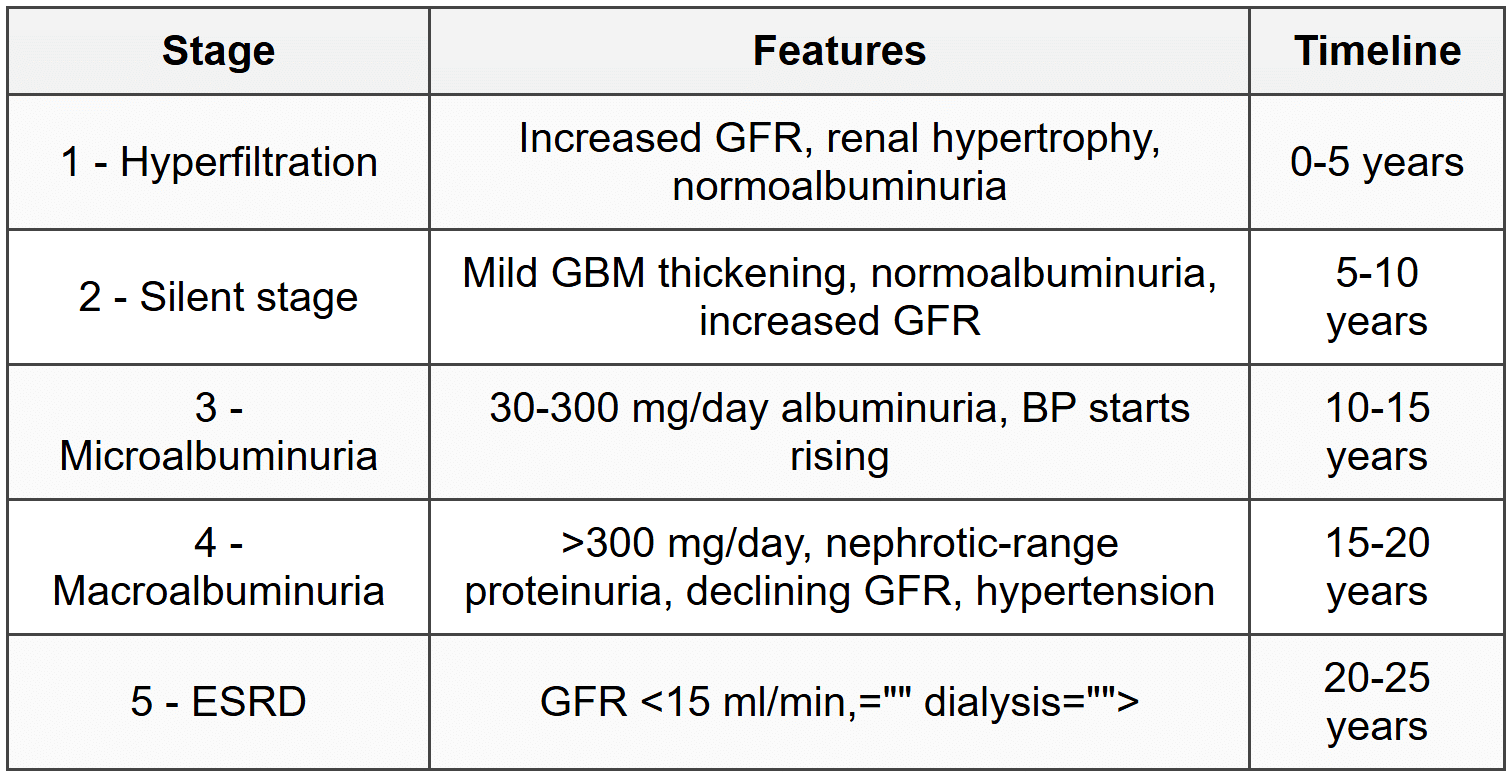
9.2 Pathology
- Kimmelstiel-Wilson nodules: nodular glomerulosclerosis (pathognomonic)
- Diffuse glomerulosclerosis (more common)
- GBM thickening, mesangial expansion, arteriolar hyalinosis
- IF and EM: linear IgG and albumin along GBM
9.3 Clinical Features
- Albuminuria precedes decline in GFR
- Non-nephrotic proteinuria initially, progresses to nephrotic syndrome
- Retinopathy present in >90% cases (if absent, consider other causes)
- Hypertension, accelerated CVD
9.4 Management
- Glycemic control: HbA1c <7%; intensive="" control="" prevents="" onset="" but="" limited="" benefit="" once="">
- BP control: target <130 0;="" acei="" or="" arb="" (first-line,="" antiproteinuric,="">
- SGLT2 inhibitors: reduce albuminuria, slow GFR decline, reduce CV events (canagliflozin, dapagliflozin, empagliflozin)
- GLP-1 agonists: reduce albuminuria and CV events (liraglutide, semaglutide)
- Finerenone (non-steroidal MRA): reduces CKD progression and CV events
- Protein restriction: 0.8 g/kg/day
- Lipid control: statin therapy
10. Hypertensive Nephropathy
10.1 Pathophysiology
- Chronic hypertension → renal arteriosclerosis → ischemic injury → nephrosclerosis
- Benign nephrosclerosis: gradual decline in GFR, mild proteinuria (<1>
- Accelerated by diabetes, smoking, hyperlipidemia
10.2 Pathology
- Arteriolosclerosis: hyaline arteriolosclerosis (benign hypertension), hyperplastic arteriolosclerosis (malignant hypertension)
- Glomerulosclerosis, tubular atrophy, interstitial fibrosis
- Granular contracted kidneys bilaterally
10.3 Clinical Features
- Long-standing hypertension, slowly progressive CKD
- Mild proteinuria, bland urine sediment, no RBC casts
- Left ventricular hypertrophy, retinopathy
10.4 Management
- BP target: <130 0="" mmhg="" in="">
- ACEi/ARB preferred if proteinuria present
- Multi-drug regimen often needed
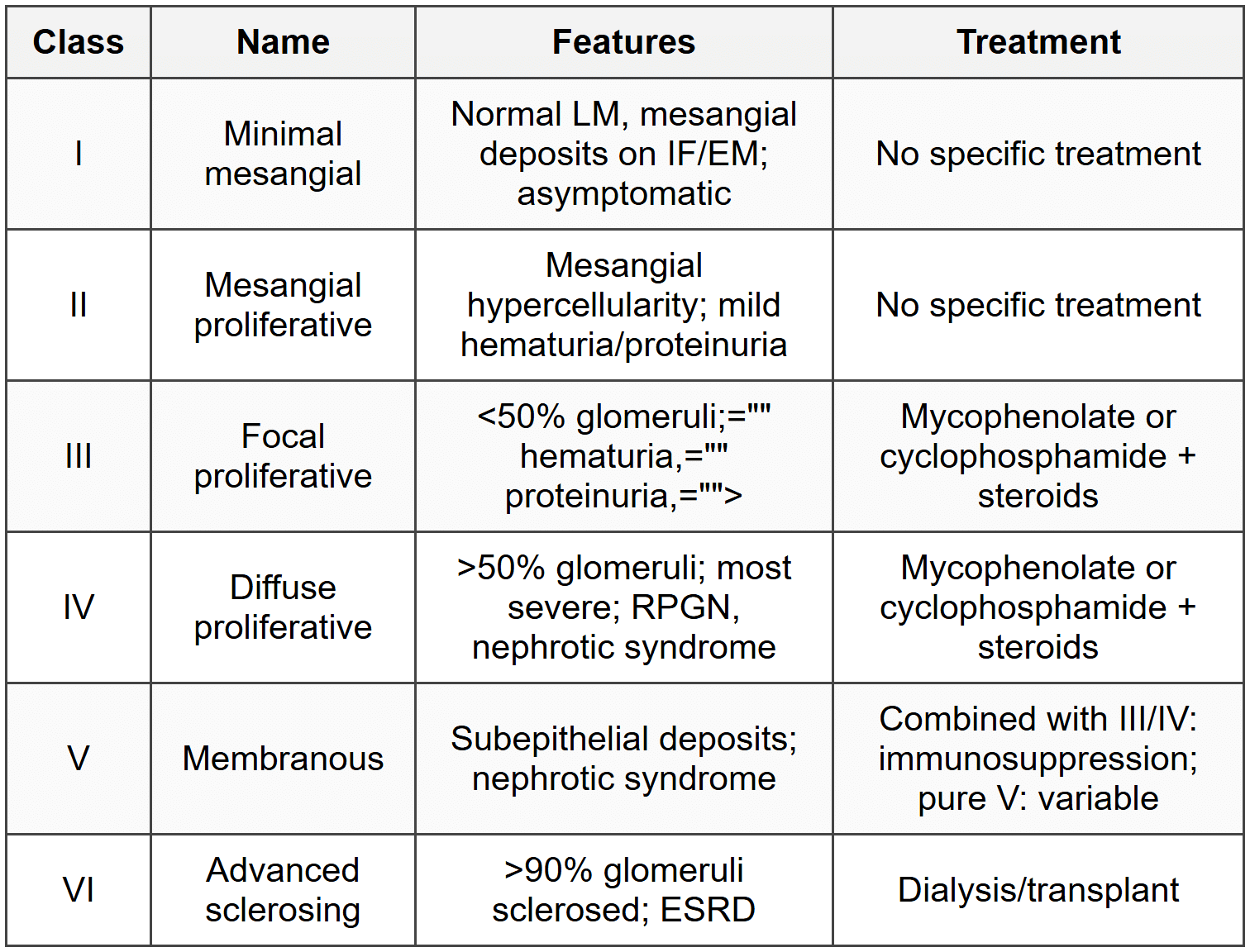
11. Lupus Nephritis
11.1 ISN/RPS Classification
11.2 Diagnosis
- Renal biopsy required for classification and treatment planning
- IF: full house pattern (IgG, IgA, IgM, C3, C1q); C1q deposition highly specific
- Low C3 and C4 (consume both classical and alternative pathways)
- Anti-dsDNA antibodies correlate with disease activity
11.3 Clinical Features
- Hematuria, proteinuria (nephritic, nephrotic, or mixed), hypertension, renal insufficiency
- Extrarenal lupus manifestations
11.4 Treatment
- Induction (Class III/IV): mycophenolate mofetil or cyclophosphamide + high-dose steroids for 6 months
- Maintenance: mycophenolate or azathioprine + low-dose steroids
- Adjunct: hydroxychloroquine, ACEi/ARB
- Refractory: rituximab, belimumab, voclosporin
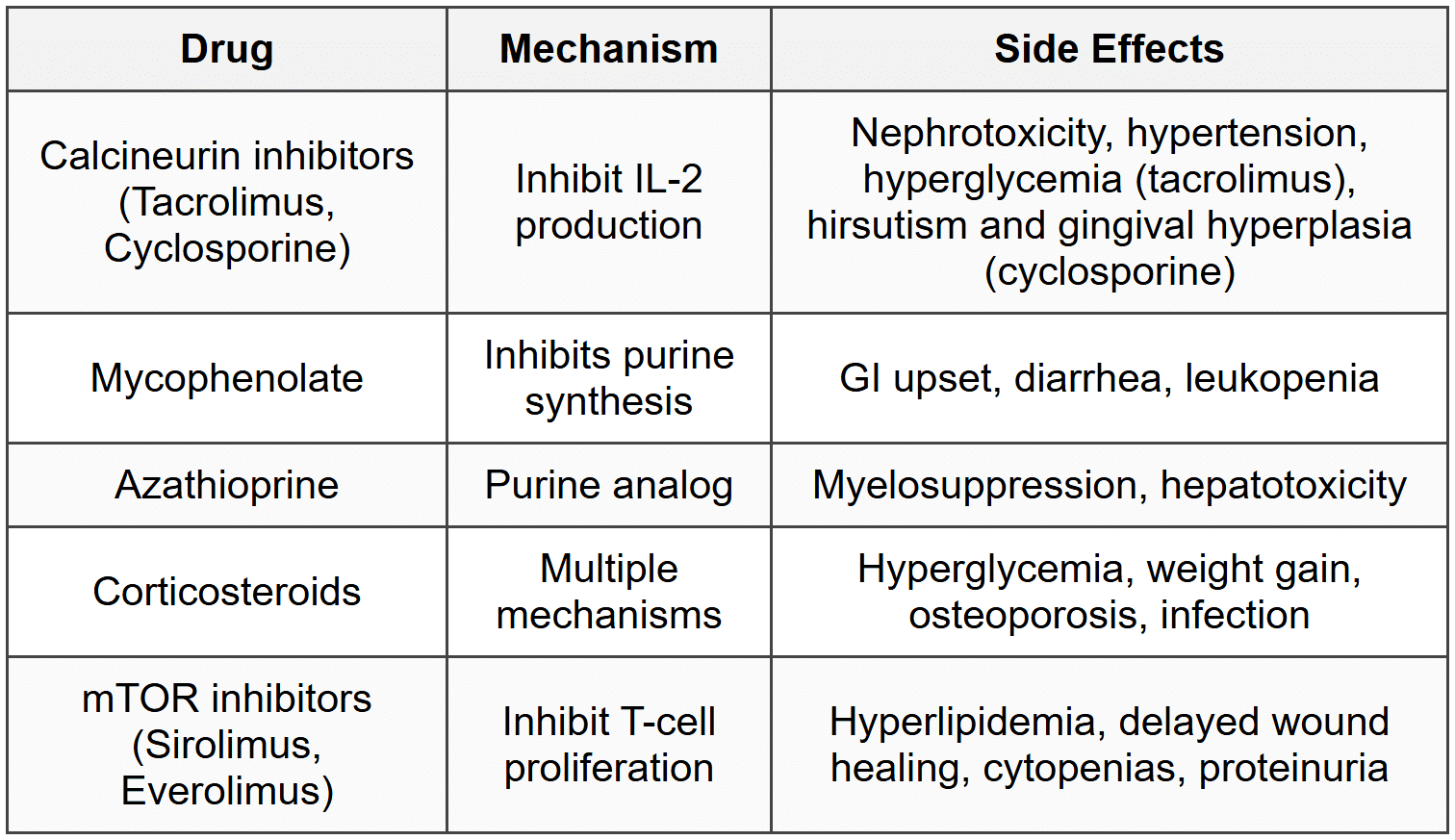
12. Renal Transplantation
12.1 Immunosuppression
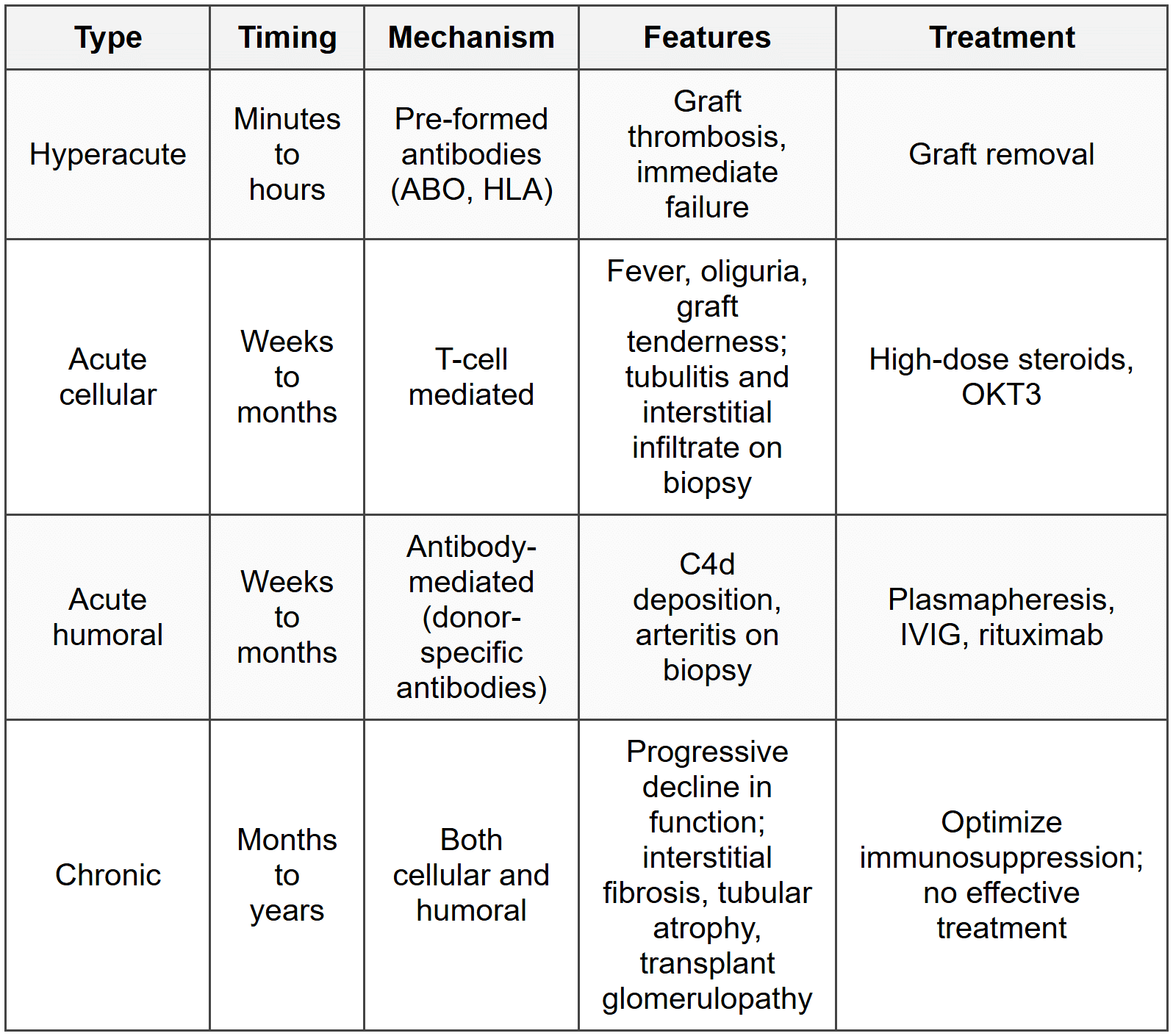
12.2 Rejection
12.3 BK Virus Nephropathy
- Polyomavirus reactivation in immunosuppressed transplant recipients
- Progressive graft dysfunction; decoy cells in urine
- Diagnosis: BK viremia, viruria; biopsy shows tubular injury with viral inclusions
- Treatment: reduce immunosuppression; cidofovir or leflunomide in severe cases
12.4 Post-Transplant Complications
- Infections: CMV (most common 1-6 months), PCP, Nocardia, Aspergillus, BK virus
- Malignancy: PTLD (EBV-related), skin cancer (SCC > BCC), Kaposi sarcoma
- Recurrent disease: FSGS, IgA nephropathy, membranoproliferative GN, diabetic nephropathy
- New-onset diabetes after transplantation (NODAT): risk with tacrolimus, steroids
13. Acid-Base and Electrolyte Disorders
13.1 Hyperkalemia
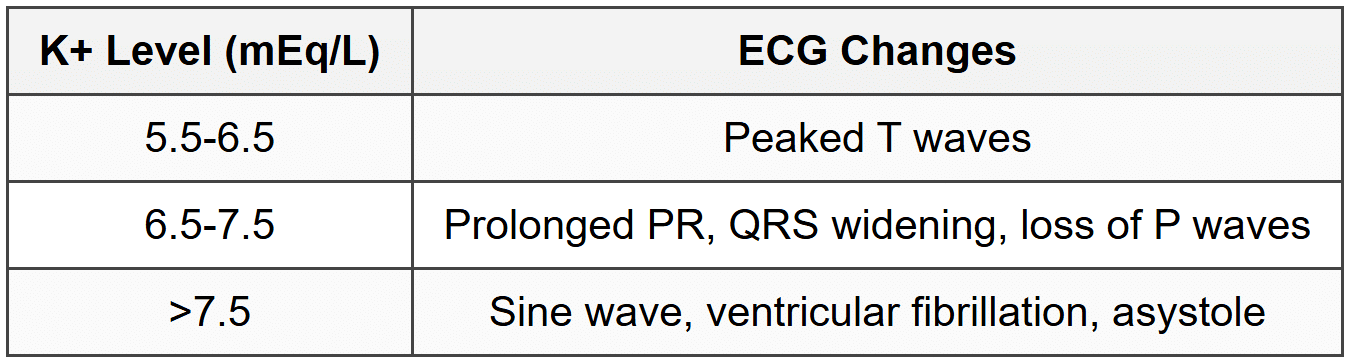
- Treatment: calcium gluconate (membrane stabilization), insulin + glucose (shift K into cells), beta-agonists, sodium bicarbonate (if acidotic), loop diuretics, K-binders (patiromer, sodium zirconium cyclosilicate), dialysis
13.2 Hypokalemia
- Causes: GI losses, renal losses (diuretics, RTA, hyperaldosteronism), intracellular shift
- ECG: U waves, flattened T waves, ST depression, prolonged QT
- Complications: muscle weakness, rhabdomyolysis, ileus, arrhythmias
- Treatment: potassium replacement (oral or IV); treat underlying cause
13.3 Hypernatremia
- Hypovolemic: dehydration, GI losses, osmotic diuresis
- Euvolemic: diabetes insipidus (central or nephrogenic), insensible losses
- Hypervolemic: hypertonic saline, hyperaldosteronism
- Treatment: correct slowly (<10-12 meq/l="" per="" 24="" hours)="" to="" avoid="" cerebral="" edema;="" use="" d5w="" or="" hypotonic="">
13.4 Hyponatremia
- Hypovolemic: GI losses, diuretics, renal losses; urine Na <20 (extrarenal)="" or="">20 (renal)
- Euvolemic: SIADH, hypothyroidism, adrenal insufficiency, psychogenic polydipsia
- Hypervolemic: CHF, cirrhosis, nephrotic syndrome; urine Na <>
- Treatment: treat underlying cause; hypertonic saline if severe/symptomatic; fluid restriction in SIADH; tolvaptan (V2 receptor antagonist)
- Correct slowly (<10-12 meq/l="" per="" 24="" hours)="" to="" avoid="" osmotic="" demyelination="">
13.5 Syndrome of Inappropriate ADH (SIADH)
- Euvolemic hypotonic hyponatremia with urine osmolality >100 mOsm/kg and urine Na >40 mEq/L
- Causes: CNS disorders, pulmonary disease (pneumonia, TB), malignancy (SCLC), drugs (SSRIs, carbamazepine, cyclophosphamide)
- Treatment: fluid restriction, salt tablets, demeclocycline, tolvaptan
13.6 Diabetes Insipidus
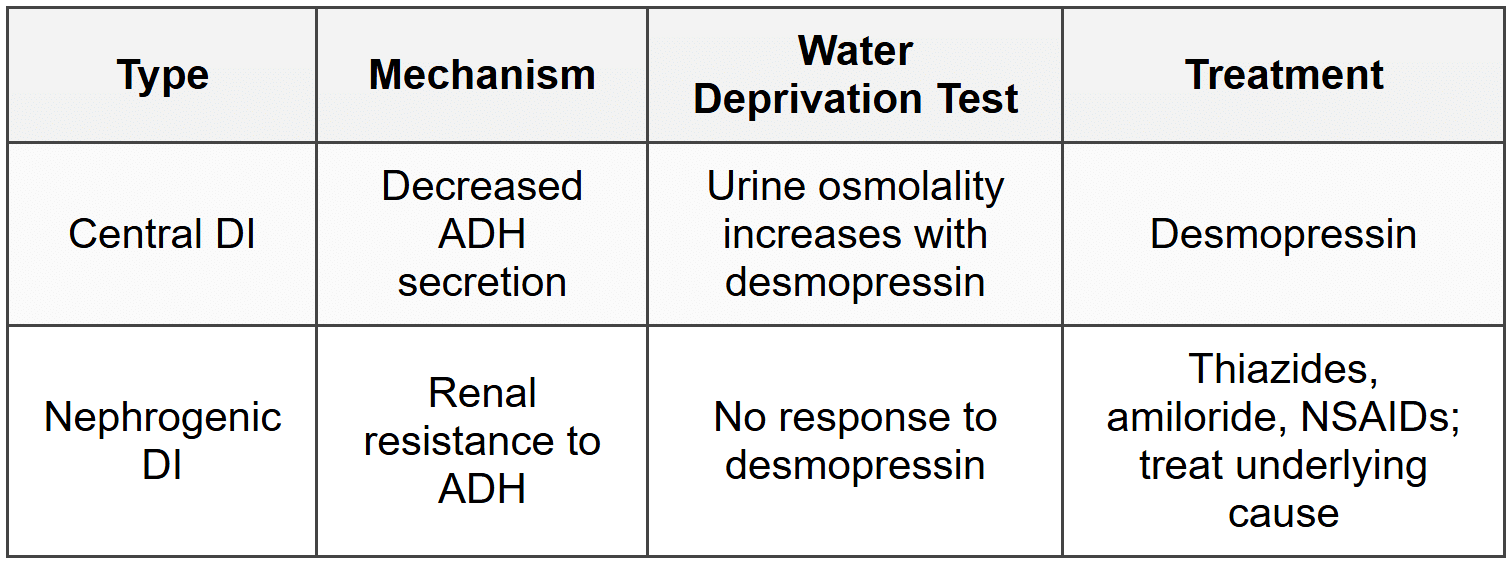
- Central DI causes: trauma, surgery, tumors (craniopharyngioma), infiltrative (sarcoid, histiocytosis)
- Nephrogenic DI causes: lithium, hypercalcemia, hypokalemia, chronic kidney disease, congenital
13.7 Hypercalcemia
- Causes: hyperparathyroidism (most common outpatient), malignancy (most common inpatient - PTHrP, lytic lesions, calcitriol in lymphoma)
- Other: vitamin D intoxication, granulomatous disease, thiazides, milk-alkali syndrome, immobilization
- Treatment: IV saline, loop diuretics, bisphosphonates, calcitonin, dialysis
13.8 Hypocalcemia
- Causes: hypoparathyroidism, vitamin D deficiency, CKD, hypomagnesemia, acute pancreatitis, tumor lysis
- Clinical: Chvostek sign, Trousseau sign, tetany, seizures, prolonged QT
- Treatment: calcium gluconate (IV if symptomatic), oral calcium, vitamin D; correct hypomagnesemia
14. Urinary Tract Infections and Related Disorders
14.1 Acute Pyelonephritis
- Fever, chills, flank pain, costovertebral angle tenderness, nausea, vomiting
- Urine: pyuria, WBC casts, bacteriuria, positive culture
- Organisms: E. coli (80%), Klebsiella, Proteus, Enterococcus
- Treatment: fluoroquinolone or ceftriaxone for 7-14 days; hospitalize if septic or unable to tolerate oral
14.2 Chronic Pyelonephritis
- Recurrent kidney infections → chronic tubulointerstitial inflammation and scarring
- Causes: VUR, obstruction, chronic stones
- Imaging: cortical scarring overlying blunted calyces
- Treatment: treat UTI, correct anatomic abnormalities
14.3 Xanthogranulomatous Pyelonephritis
- Chronic severe infection with foamy lipid-laden macrophages
- Associated with Proteus infection and staghorn calculi
- CT: enlarged kidney with mass-like appearance
- Treatment: nephrectomy
14.4 Renal Papillary Necrosis
- Ischemic necrosis of renal papillae
- Causes (POSTCARDS): Pyelonephritis, Obstruction, Sickle cell, TB, Cirrhosis, Analgesics (NSAIDs), Renal vein thrombosis, Diabetes, Systemic vasculitis
- Hematuria, flank pain, passing of tissue fragments in urine
- IVP: ring sign or contrast in necrotic papillae
14.5 Perinephric Abscess
- Collection of pus in perinephric space
- Causes: extension from pyelonephritis, hematogenous spread (S. aureus)
- Fever, flank pain persisting despite antibiotics
- CT: fluid collection with rim enhancement
- Treatment: drainage + antibiotics
15. Renal Neoplasms
15.1 Renal Cell Carcinoma
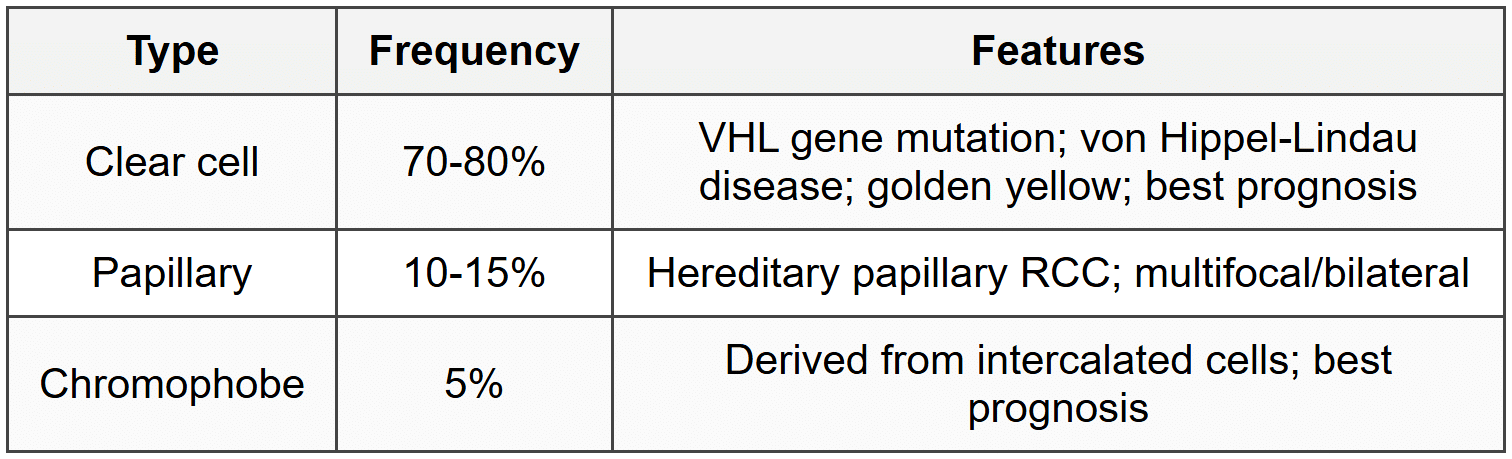
- Risk factors: smoking, obesity, hypertension, VHL, acquired cystic kidney disease in dialysis patients
- Classic triad (10%): hematuria, flank pain, palpable mass
- Paraneoplastic: polycythemia (EPO), hypercalcemia (PTHrP), hypertension (renin), Stauffer syndrome (reversible hepatic dysfunction)
- Metastases: lung, bone, brain; cannonball metastases in lungs
- Diagnosis: CT/MRI abdomen; renal mass protocol CT
- Treatment: partial or radical nephrectomy; sunitinib, pazopanib (VEGF inhibitors), nivolumab (immunotherapy) for metastatic
15.2 Wilms Tumor (Nephroblastoma)
- Most common renal malignancy in children (peak age 2-5 years)
- WAGR syndrome: Wilms, Aniridia, Genitourinary abnormalities, mental Retardation; WT1 gene deletion
- Denys-Drash syndrome: male pseudohermaphroditism, glomerulopathy, Wilms tumor
- Beckwith-Wiedemann syndrome: macroglossia, organomegaly, hemihypertrophy, Wilms tumor
- Presentation: asymptomatic abdominal mass, hematuria, hypertension
- Treatment: nephrectomy + chemotherapy (vincristine, actinomycin D, doxorubicin); excellent prognosis (>90% cure)
15.3 Angiomyolipoma
- Benign tumor composed of blood vessels, smooth muscle, and fat
- Associated with tuberous sclerosis (bilateral, multiple); sporadic cases (unilateral, single)
- Risk of spontaneous hemorrhage if >4 cm
- Diagnosis: CT showing fat density (negative Hounsfield units)
- Treatment: observation if <4 cm;="" embolization="" or="" resection="" if="">4 cm or symptomatic
15.4 Oncocytoma
- Benign renal tumor; mahogany brown with central scar
- Cannot distinguish from RCC on imaging; diagnosed after nephrectomy
- No malignant potential
15.5 Transitional Cell Carcinoma (Urothelial Carcinoma)
- Arises from renal pelvis, ureter, bladder
- Risk factors: smoking, analgesic nephropathy, Balkan nephropathy, cyclophosphamide, aromatic amines
- Painless gross hematuria
- Treatment: nephroureterectomy for upper tract; TURBT for bladder
About this Document

4.98/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: CheatSheet: Disorders of Kidney for NEET PG 2026 is part of Medicine preparation. The notes and questions for CheatSheet: Disorders of Kidney have been prepared according to the NEET PG exam syllabus. Information about CheatSheet: Disorders of Kidney covers topics like and CheatSheet: Disorders of Kidney Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for CheatSheet: Disorders of Kidney.
Introduction of CheatSheet: Disorders of Kidney in English is available as part of our Medicine for NEET PG & CheatSheet: Disorders of Kidney in Hindi for Medicine course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: CheatSheet: Disorders of Kidney
Description
CheatSheet: Disorders of Kidney of Medicine to help you remember important concepts with short tricks. Start learning for NEET PG exam & improve retention with EduRev.
Information about CheatSheet: Disorders of Kidney
In this doc you can find the meaning of CheatSheet: Disorders of Kidney defined & explained in the simplest way possible. Besides explaining types of CheatSheet: Disorders of Kidney theory, EduRev gives you an ample number of questions to practice CheatSheet: Disorders of Kidney tests, examples and also practice NEET PG tests


Related Searches
Summary, Semester Notes, practice quizzes, CheatSheet: Disorders of Kidney, Free, study material, ppt, MCQs, past year papers, pdf , Objective type Questions, Extra Questions, Viva Questions, Previous Year Questions with Solutions, video lectures, Exam, Important questions, mock tests for examination, CheatSheet: Disorders of Kidney, shortcuts and tricks, CheatSheet: Disorders of Kidney, Sample Paper;