NEET PG Exam > NEET PG Notes > Medicine > CheatSheet: Fluids and Electrolytes
CheatSheet: Fluids and Electrolytes


1. Body Fluid Compartments
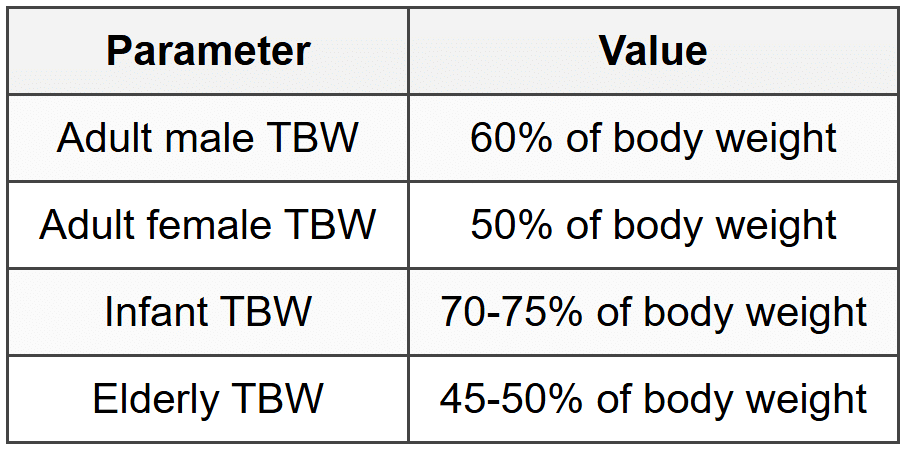
1.1 Total Body Water (TBW)
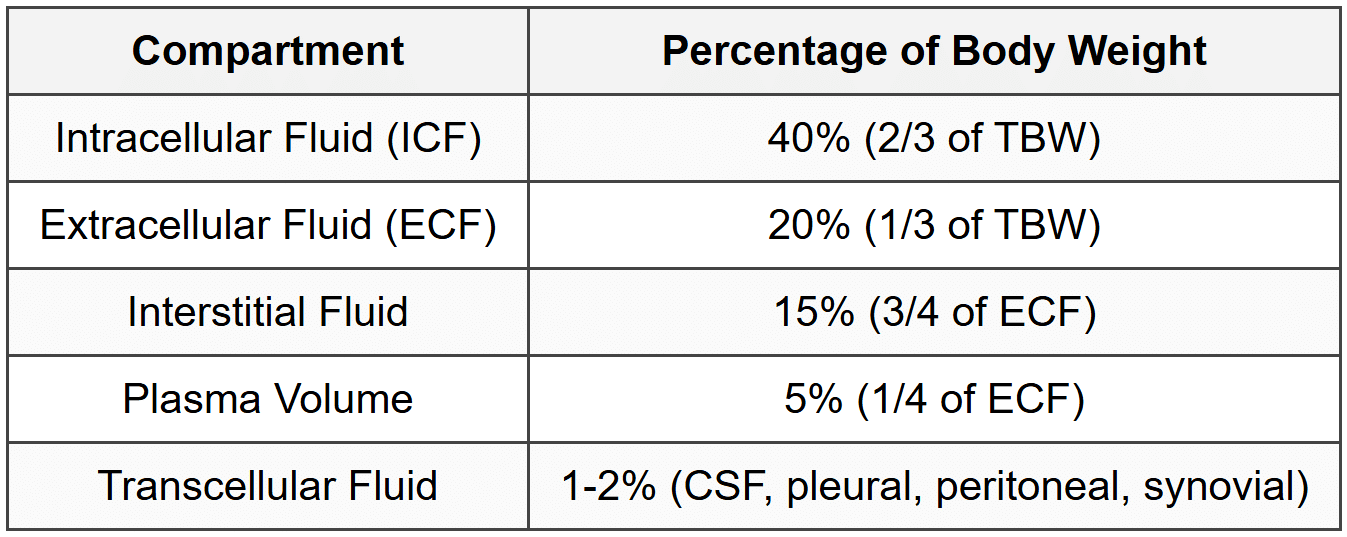
1.2 Fluid Distribution
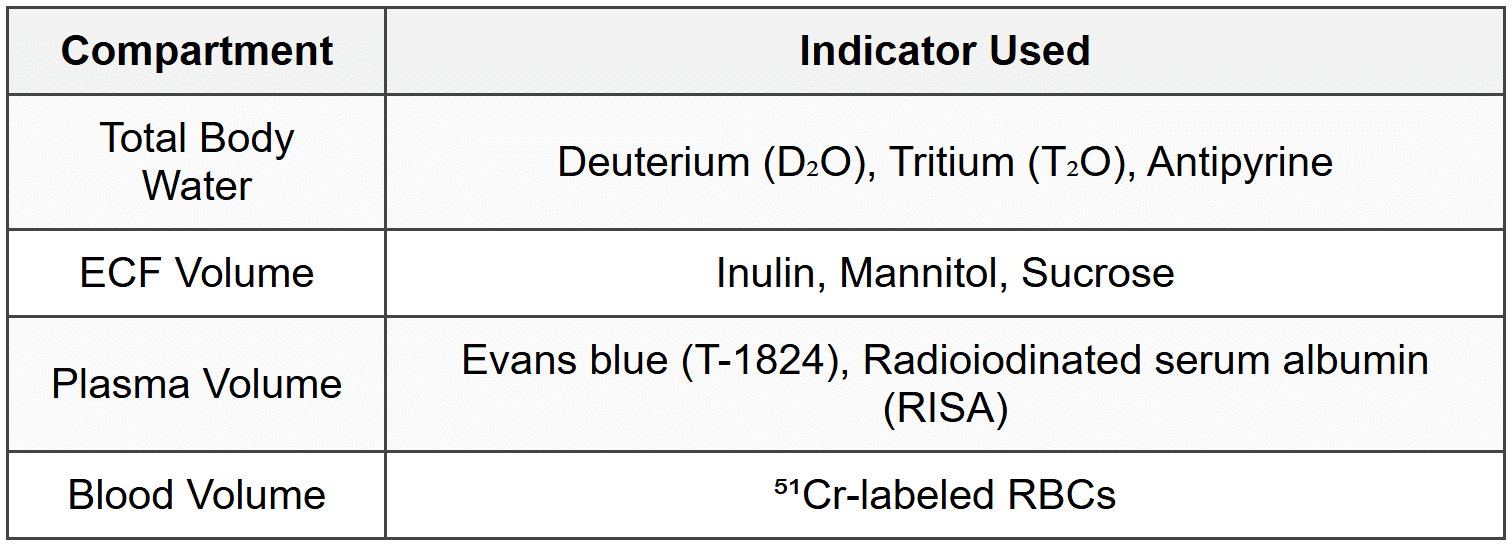
1.3 Measurement Methods
2. Electrolyte Composition
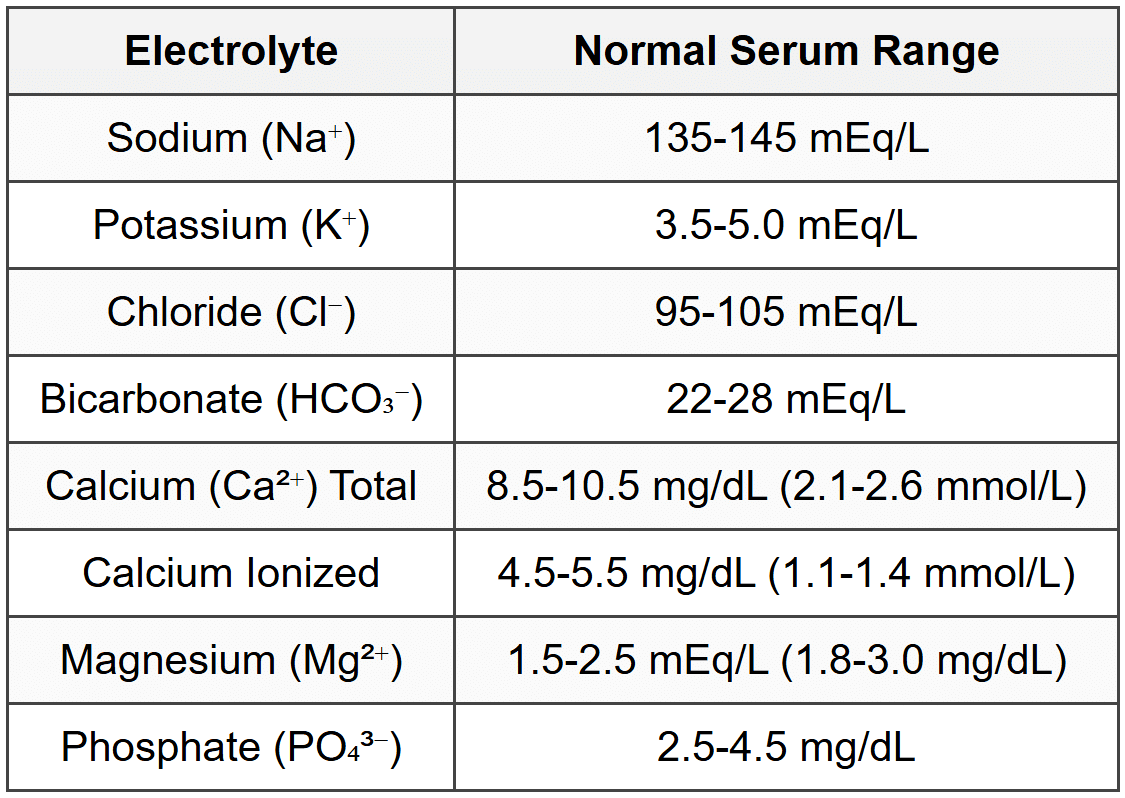
2.1 Normal Electrolyte Values
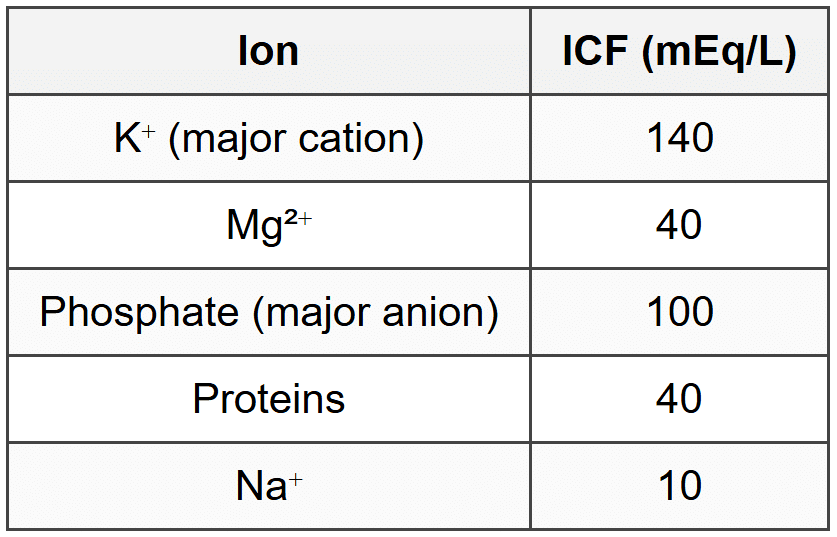
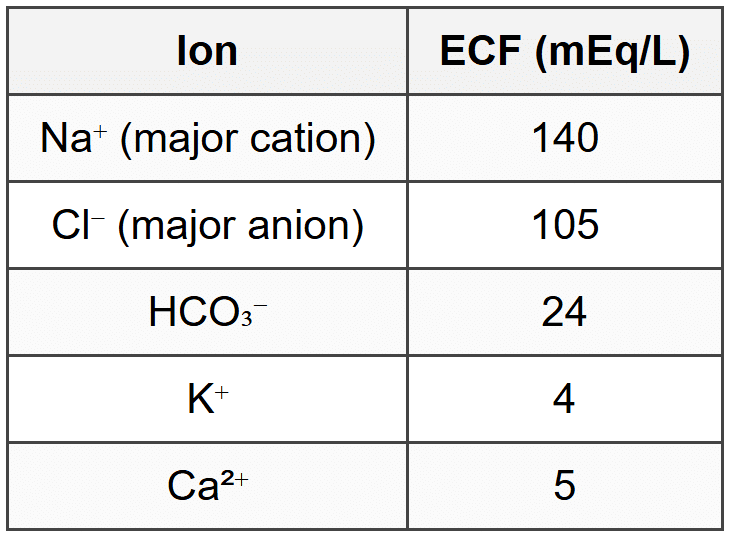
2.2 ICF vs ECF Composition
3. Sodium Disorders
3.1 Hyponatremia
3.1.1 Definition and Classification
- Serum Na⁺ < 135="">
- Mild: 130-135 mEq/L; Moderate: 125-130 mEq/L; Severe: < 125="">
- Acute: < 48="" hours;="" chronic:=""> 48 hours
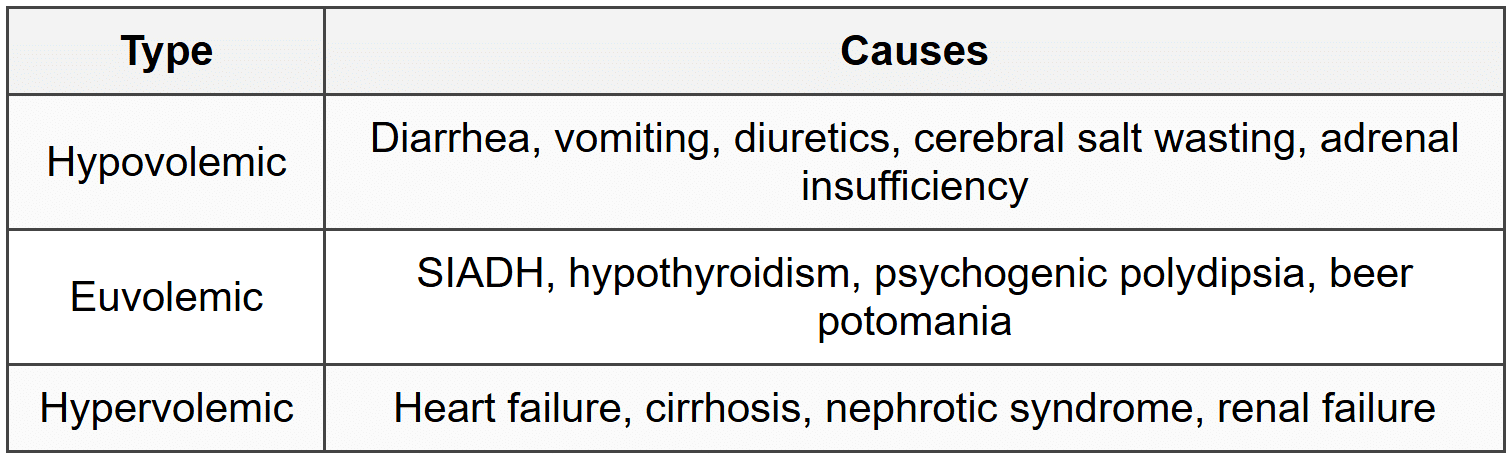
3.1.2 Classification by Volume Status
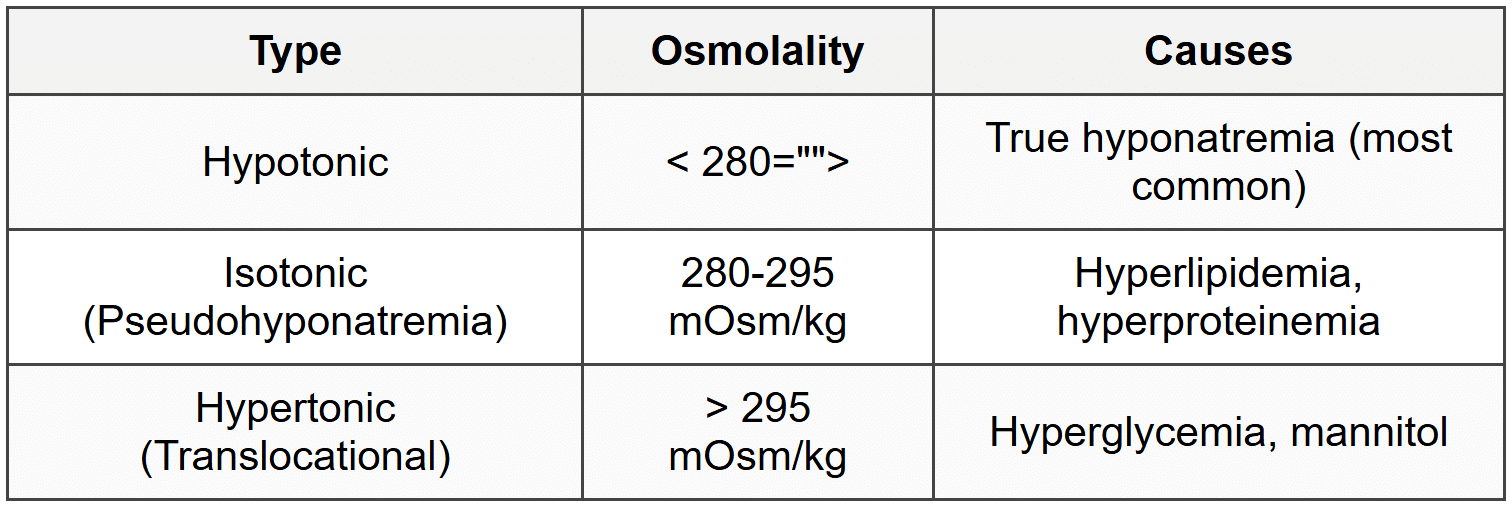
3.1.3 Classification by Osmolality
3.1.4 SIADH Criteria
- Serum osmolality < 275="">
- Urine osmolality > 100 mOsm/kg (inappropriately concentrated)
- Urine Na⁺ > 40 mEq/L
- Clinical euvolemia
- Normal thyroid and adrenal function
3.1.5 Clinical Features
- Nausea, vomiting, headache, confusion
- Lethargy, seizures, coma (severe cases)
- Symptoms more severe with acute onset
3.1.6 Treatment Principles
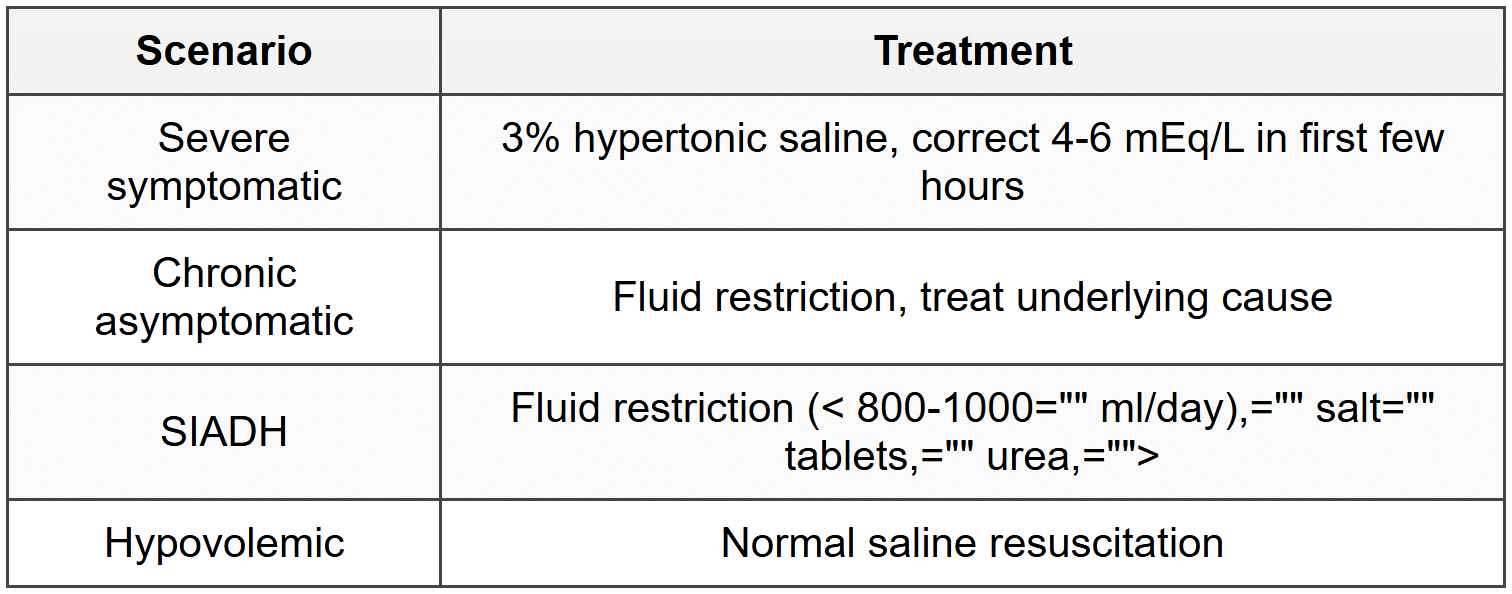
- Maximum correction rate: 8-10 mEq/L per 24 hours (avoid osmotic demyelination syndrome)
- Osmotic demyelination syndrome risk: correction > 12 mEq/L in 24 hours
3.2 Hypernatremia
3.2.1 Definition
- Serum Na⁺ > 145 mEq/L
- Always indicates hyperosmolar state
3.2.2 Causes by Volume Status
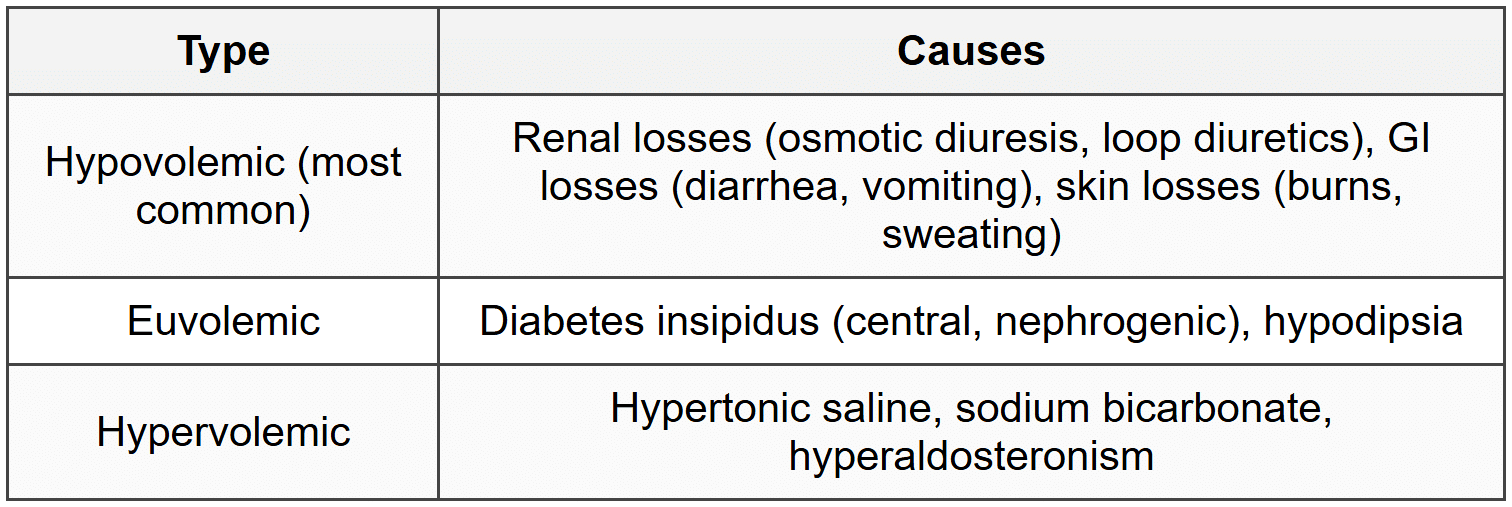
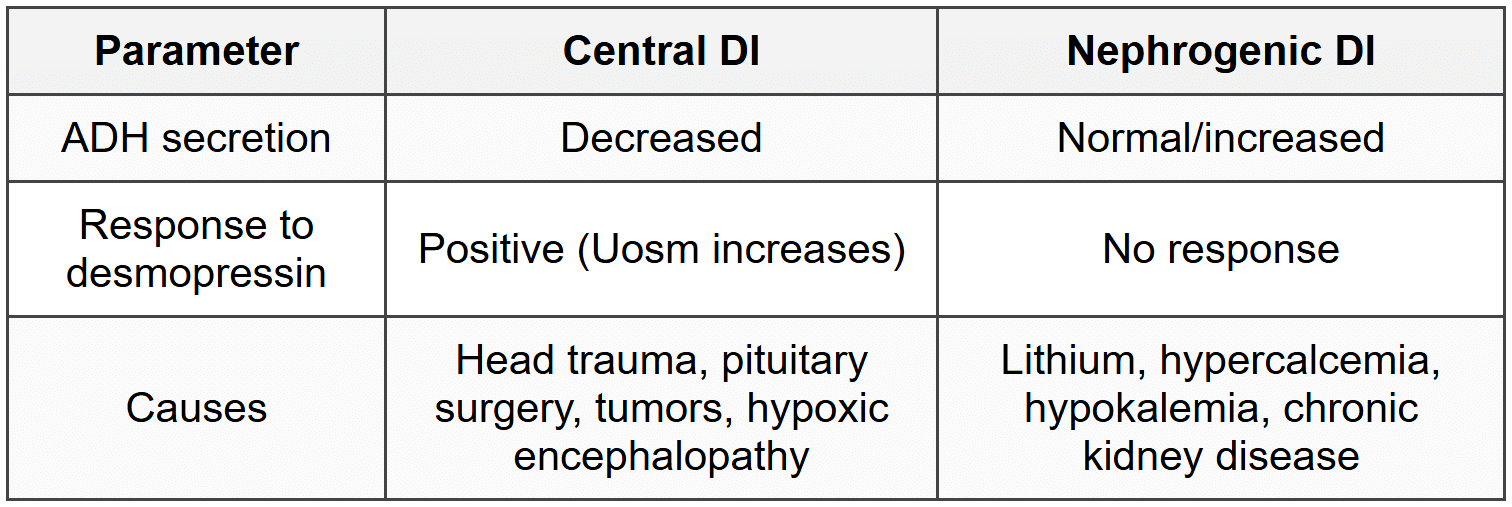
3.2.3 Diabetes Insipidus Differentiation
3.2.4 Clinical Features
- Thirst, restlessness, irritability
- Altered mental status, seizures, coma
- Muscle weakness, hyperreflexia
3.2.5 Treatment
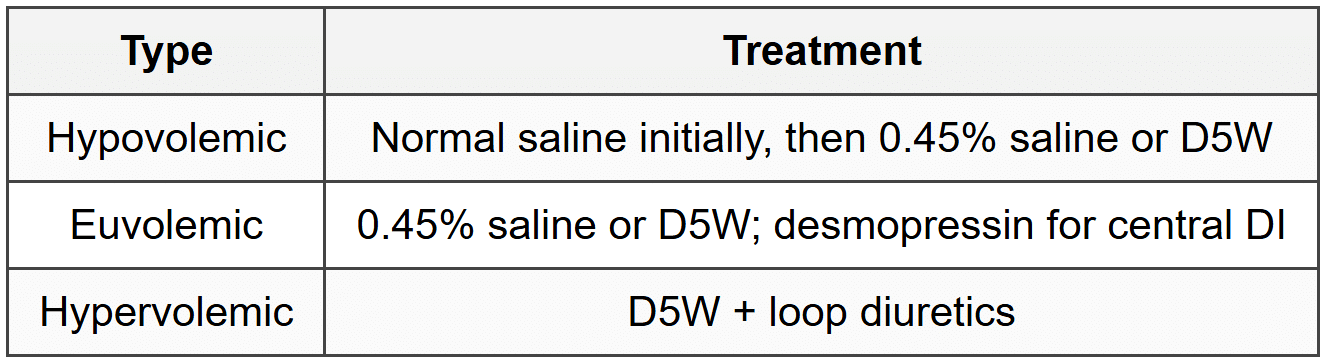
- Correction rate: 0.5 mEq/L/hour; maximum 10-12 mEq/L per 24 hours
- Rapid correction causes cerebral edema
4. Potassium Disorders
4.1 Hypokalemia
4.1.1 Definition
- Serum K⁺ < 3.5="">
- Mild: 3.0-3.5 mEq/L; Moderate: 2.5-3.0 mEq/L; Severe: < 2.5="">
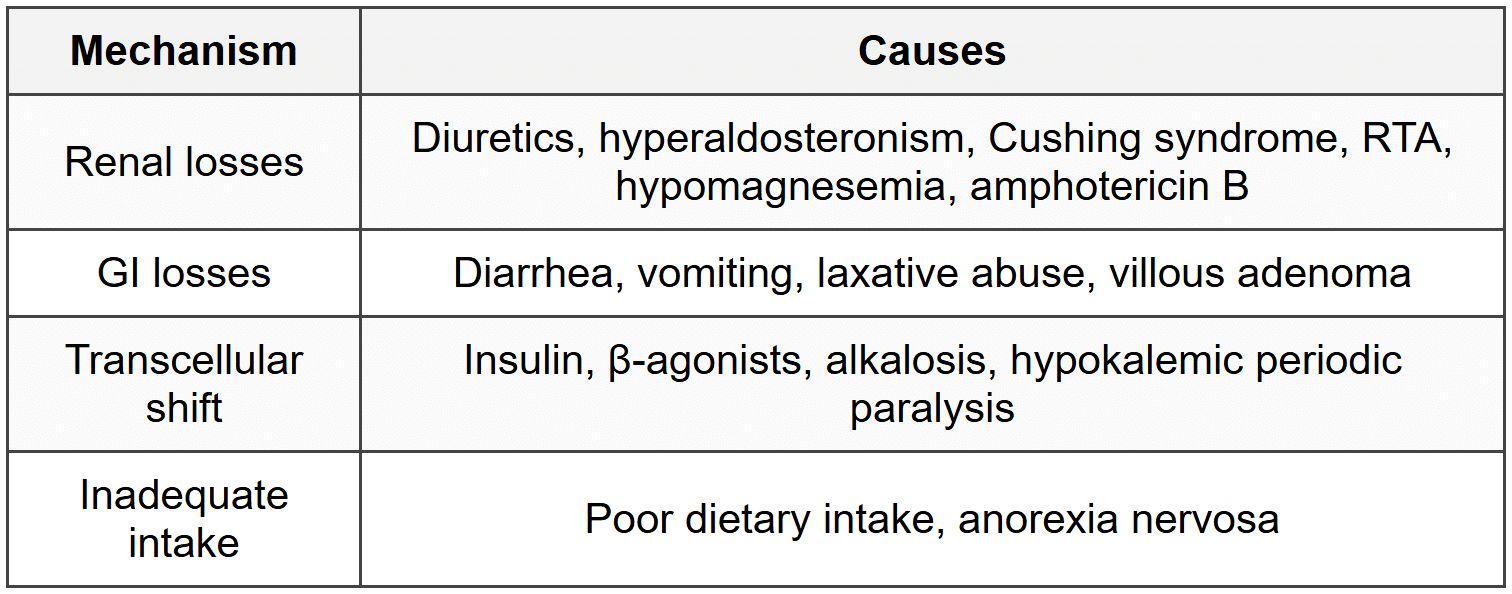
4.1.2 Causes
4.1.3 Clinical Features
- Muscle weakness, cramps, fatigue, hyporeflexia
- Paralytic ileus, constipation
- Polyuria, polydipsia (nephrogenic DI)
- Rhabdomyolysis (severe cases)
4.1.4 ECG Changes
- U waves (most characteristic)
- T wave flattening/inversion
- ST depression
- PR prolongation
- QT prolongation (actually QU prolongation)
- Increased arrhythmia risk, especially with digoxin
4.1.5 Treatment
- Oral replacement: preferred if mild-moderate and patient can tolerate
- IV replacement: severe (< 2.5="" meq/l)="" or="" symptomatic="">
- Maximum IV rate: 10-20 mEq/hour via peripheral line; up to 40 mEq/hour via central line (with cardiac monitoring)
- Correct hypomagnesemia simultaneously (refractory hypokalemia without Mg correction)
4.2 Hyperkalemia
4.2.1 Definition
- Serum K⁺ > 5.0 mEq/L
- Mild: 5.5-6.0 mEq/L; Moderate: 6.0-7.0 mEq/L; Severe: > 7.0 mEq/L
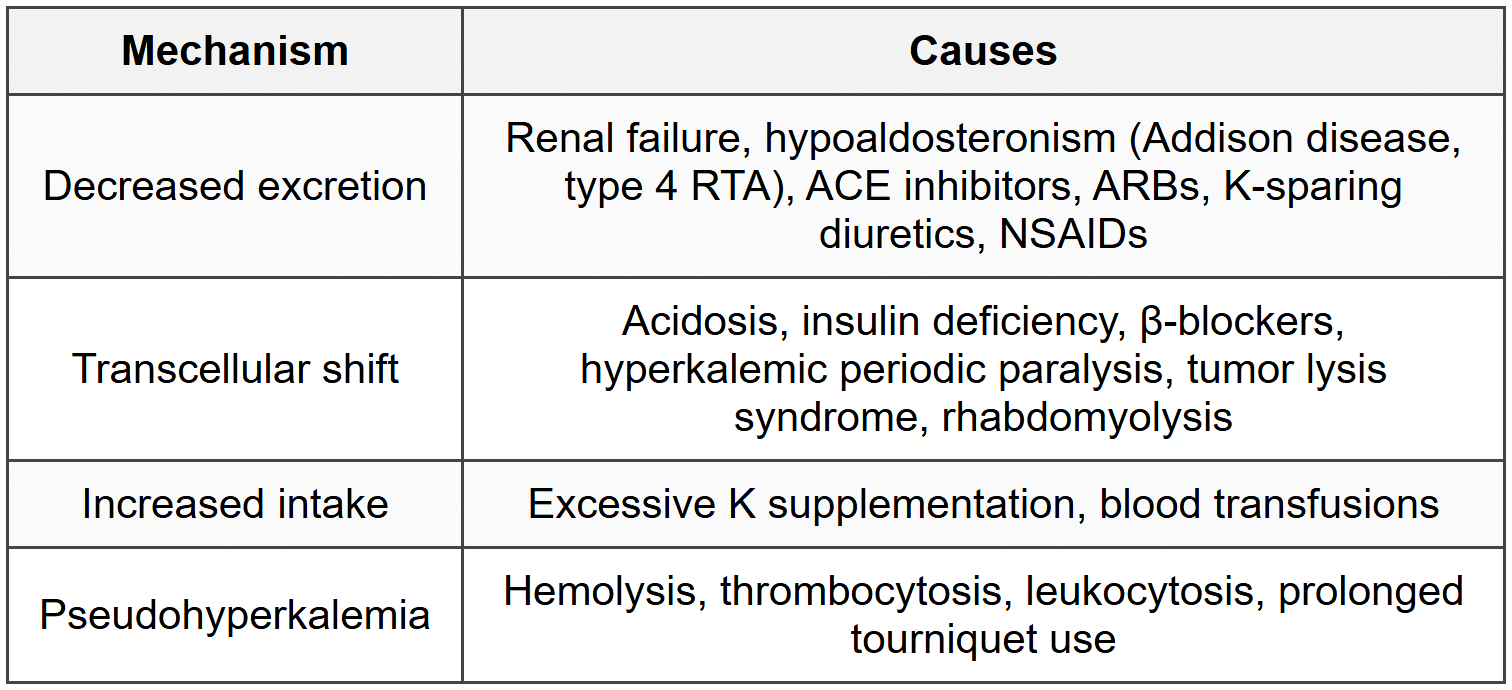
4.2.2 Causes
4.2.3 Clinical Features
- Muscle weakness, ascending paralysis
- Paresthesias
- Cardiac arrhythmias (life-threatening)
4.2.4 ECG Changes (Sequential)
- Peaked T waves (earliest, at K⁺ 5.5-6.5 mEq/L)
- Prolonged PR interval
- Widened QRS complex
- P wave flattening/disappearance
- Sine wave pattern (pre-terminal)
- Ventricular fibrillation/asystole
4.2.5 Treatment (Sequential Approach)
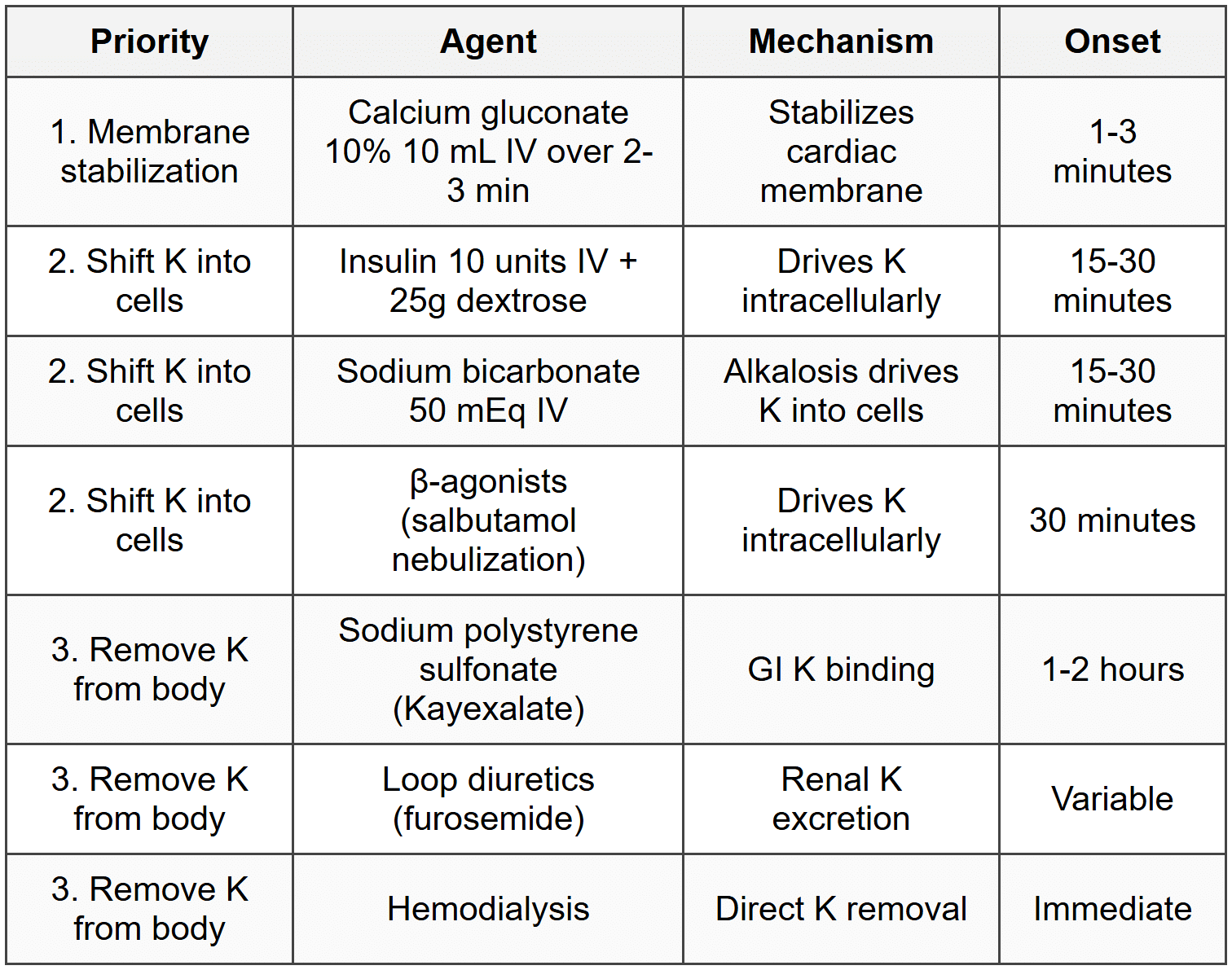
- Calcium gluconate does not lower K, only protects heart (duration 30-60 minutes, repeat if needed)
- Hemodialysis indicated for refractory cases, severe renal failure, or life-threatening hyperkalemia
5. Calcium Disorders
5.1 Calcium Homeostasis
- Total serum Ca²⁺: 50% ionized (active), 40% protein-bound (albumin), 10% complexed
- Corrected Ca²⁺ = measured Ca²⁺ + 0.8 × (4 - serum albumin)
- Hypercalcemia threshold: > 10.5 mg/dL (or ionized > 5.5 mg/dL)
- Hypocalcemia threshold: < 8.5="" mg/dl="" (or="" ionized="">< 4.5="">
5.2 Hypercalcemia
5.2.1 Common Causes (90% of cases)
- Primary hyperparathyroidism (outpatient)
- Malignancy (inpatient): PTHrP-mediated (squamous cell, renal, bladder), osteolytic metastases, multiple myeloma
5.2.2 Other Causes
- Vitamin D toxicity, granulomatous diseases (sarcoidosis, TB)
- Thiazide diuretics, lithium
- Familial hypocalciuric hypercalcemia (FHH)
- Immobilization, hyperthyroidism
5.2.3 Clinical Features (Bones, Stones, Groans, Moans, Psychiatric Overtones)
- Bones: bone pain, osteitis fibrosa cystica, pathologic fractures
- Stones: nephrolithiasis, nephrocalcinosis
- Groans: abdominal pain, constipation, peptic ulcers, pancreatitis
- Moans: polyuria, polydipsia, nocturia
- Psychiatric: depression, confusion, lethargy, coma
5.2.4 ECG Changes
- Shortened QT interval
- Bradycardia, AV blocks
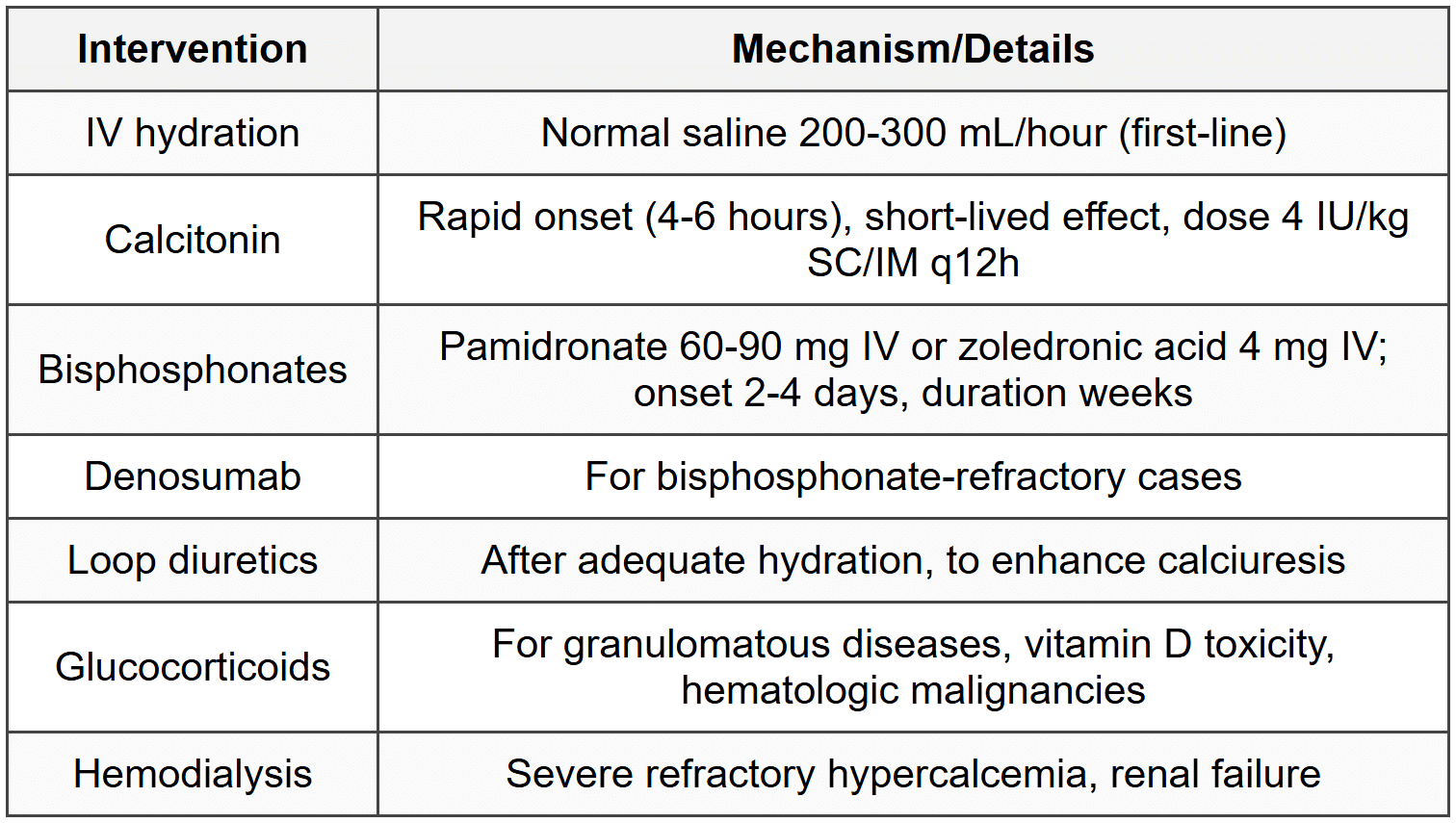
5.2.5 Treatment
5.3 Hypocalcemia
5.3.1 Causes
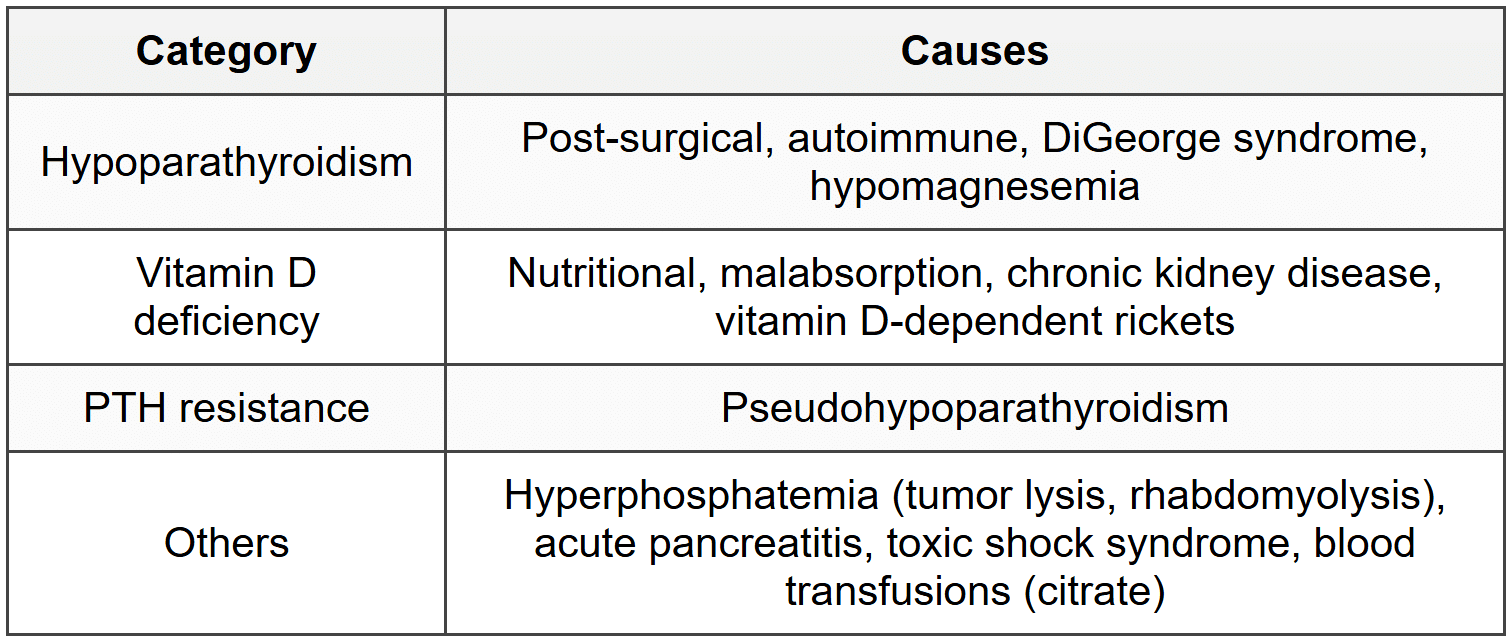
5.3.2 Clinical Features
- Neuromuscular irritability: paresthesias (perioral, fingertips), muscle cramps, tetany
- Chvostek sign: facial twitch with tapping facial nerve
- Trousseau sign: carpopedal spasm with BP cuff inflation above systolic for 3 minutes
- Seizures, laryngospasm, bronchospasm
- Papilledema, basal ganglia calcification
5.3.3 ECG Changes
- Prolonged QT interval
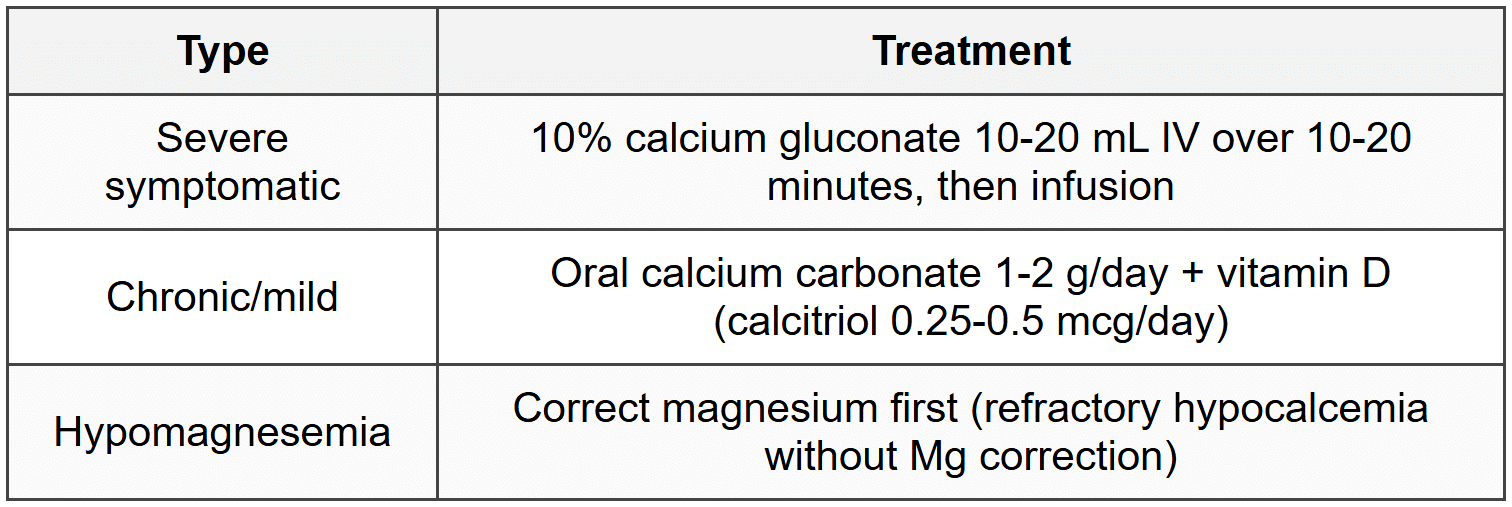
5.3.4 Treatment
6. Magnesium Disorders
6.1 Hypomagnesemia
6.1.1 Definition
- Serum Mg²⁺ < 1.5="" meq/l="">< 1.8="">
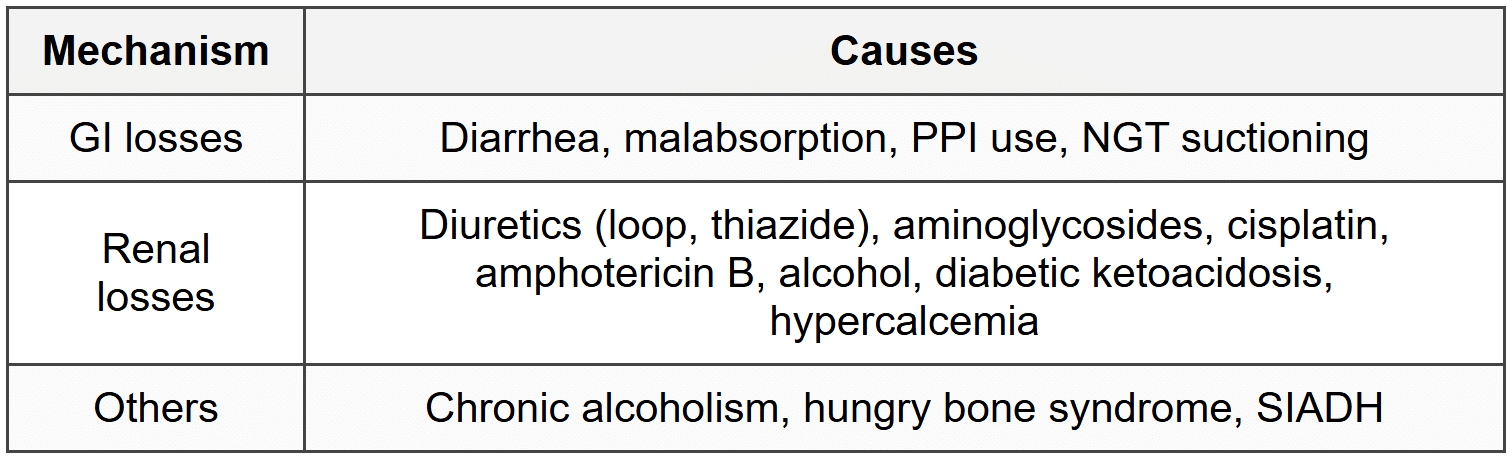
6.1.2 Causes
6.1.3 Clinical Features
- Neuromuscular: tremor, fasciculations, tetany, seizures, Chvostek and Trousseau signs
- Cardiac: arrhythmias (torsades de pointes), increased digoxin toxicity
- Associated with hypokalemia and hypocalcemia (refractory to treatment without Mg correction)
6.1.4 ECG Changes
- Prolonged QT interval, flattened T waves
- Torsades de pointes
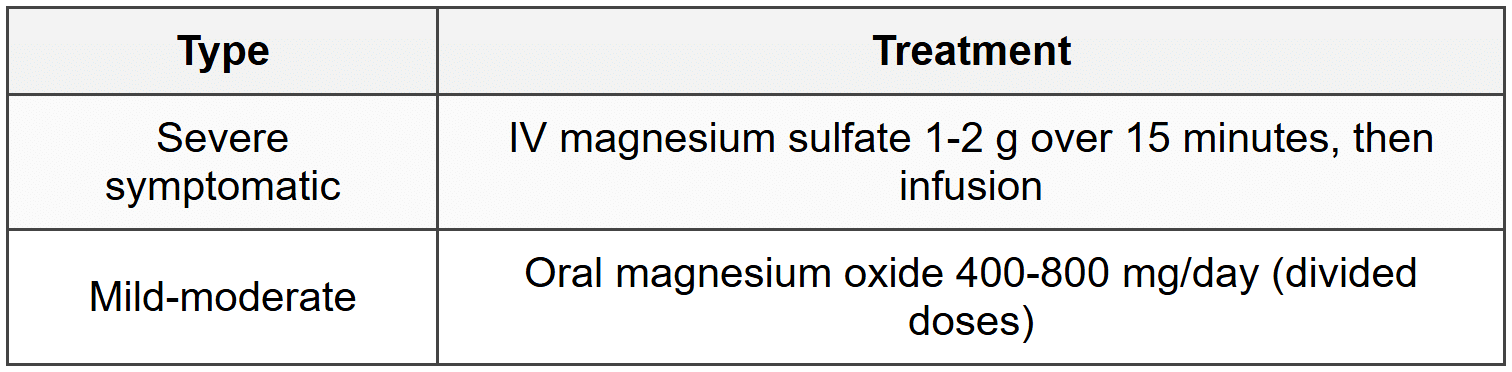
6.1.5 Treatment
6.2 Hypermagnesemia
6.2.1 Definition
- Serum Mg²⁺ > 2.5 mEq/L (> 3.0 mg/dL)
6.2.2 Causes
- Renal failure (most common)
- Excessive intake: Mg-containing antacids/laxatives, IV Mg for eclampsia
- Tumor lysis syndrome, rhabdomyolysis
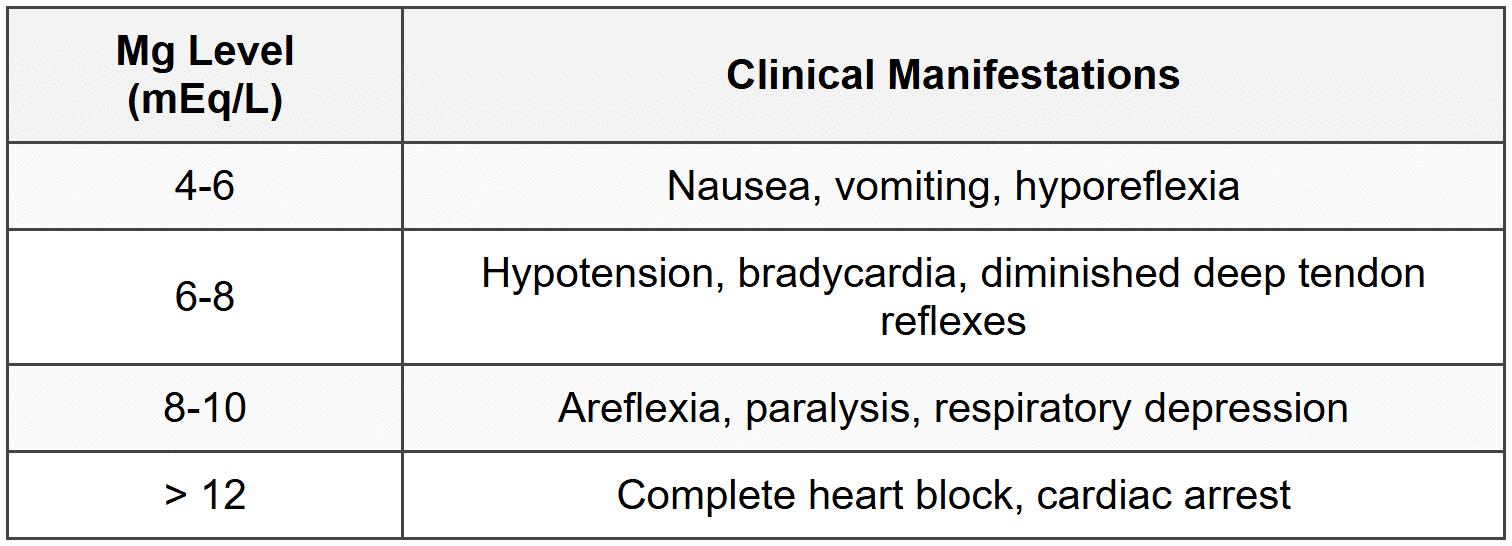
6.2.3 Clinical Features (Level-Dependent)
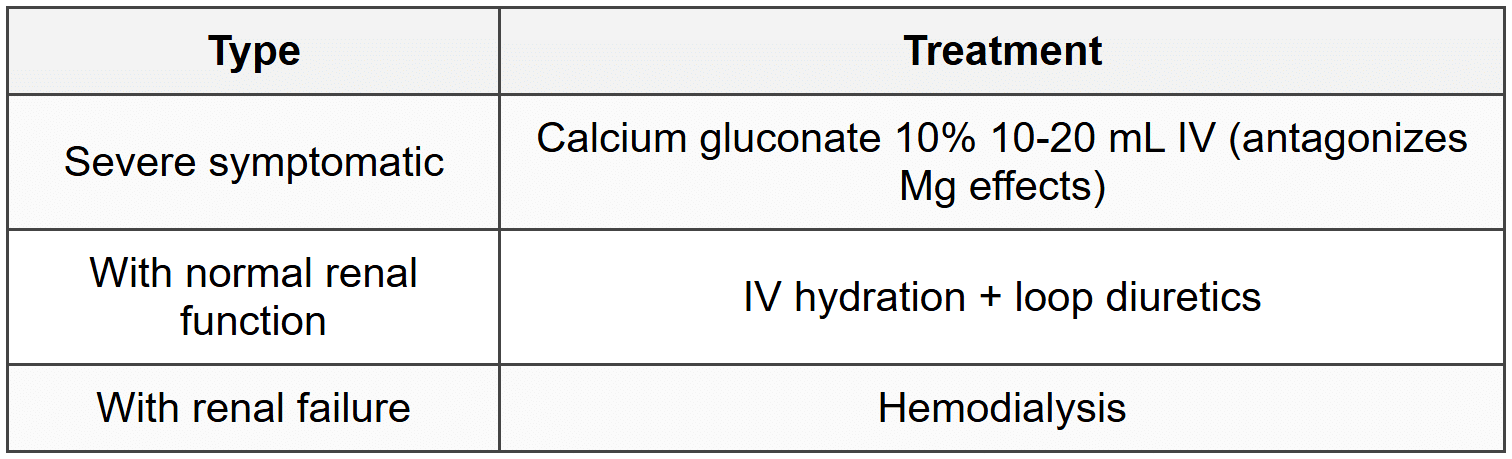
6.2.4 Treatment
7. Phosphate Disorders
7.1 Hypophosphatemia
7.1.1 Definition
- Serum PO₄³⁻ < 2.5="">
- Severe: < 1.0="">
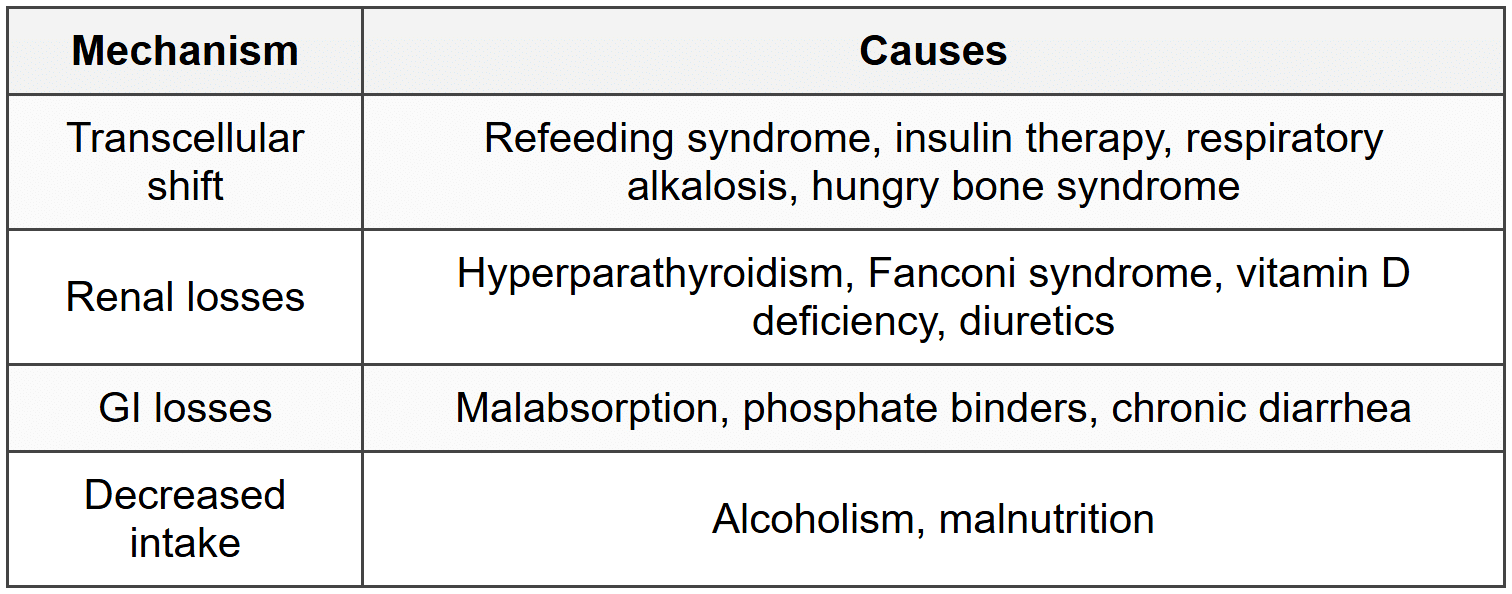
7.1.2 Causes
7.1.3 Clinical Features
- Muscle weakness, rhabdomyolysis (severe)
- Hemolytic anemia, impaired leukocyte function
- Respiratory failure (diaphragmatic weakness)
- Cardiomyopathy, arrhythmias
- Confusion, seizures, coma
- Impaired bone mineralization (chronic)
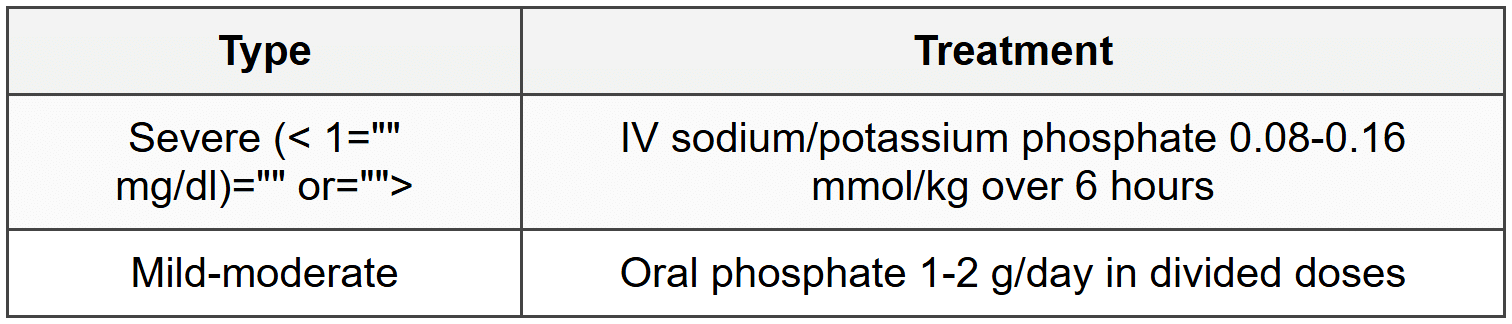
7.1.4 Treatment
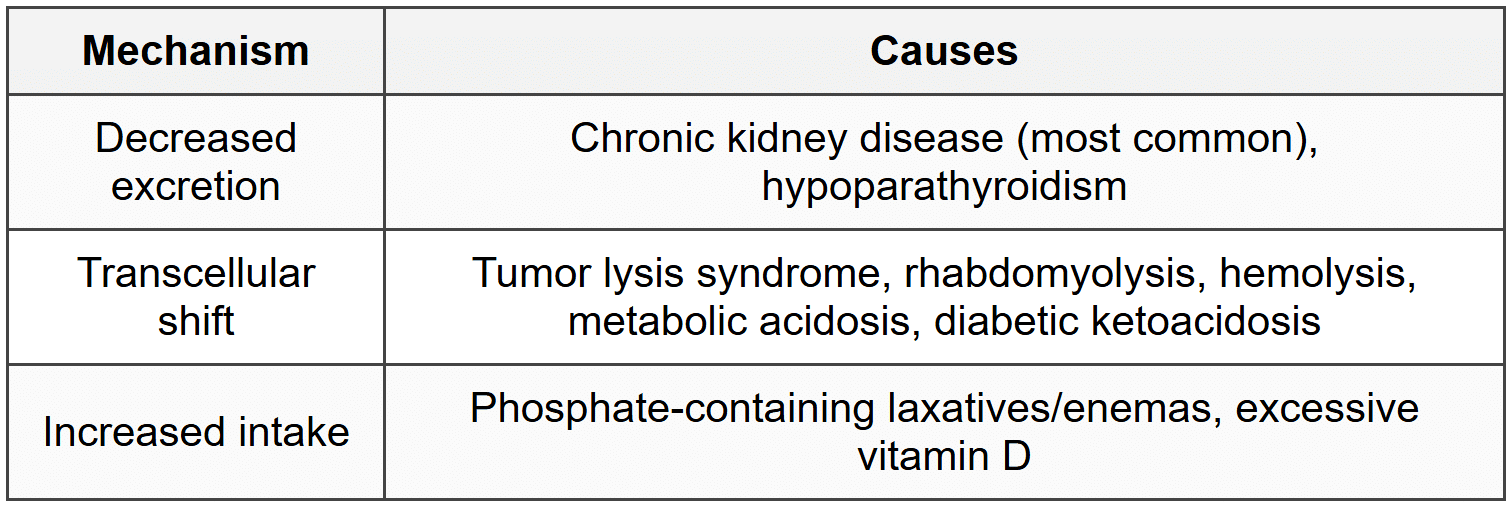
7.2 Hyperphosphatemia
7.2.1 Definition
- Serum PO₄³⁻ > 4.5 mg/dL
7.2.2 Causes
7.2.3 Clinical Features
- Secondary hypocalcemia symptoms (tetany, paresthesias)
- Metastatic calcification (soft tissue, vascular)
- Pruritus (with CKD)
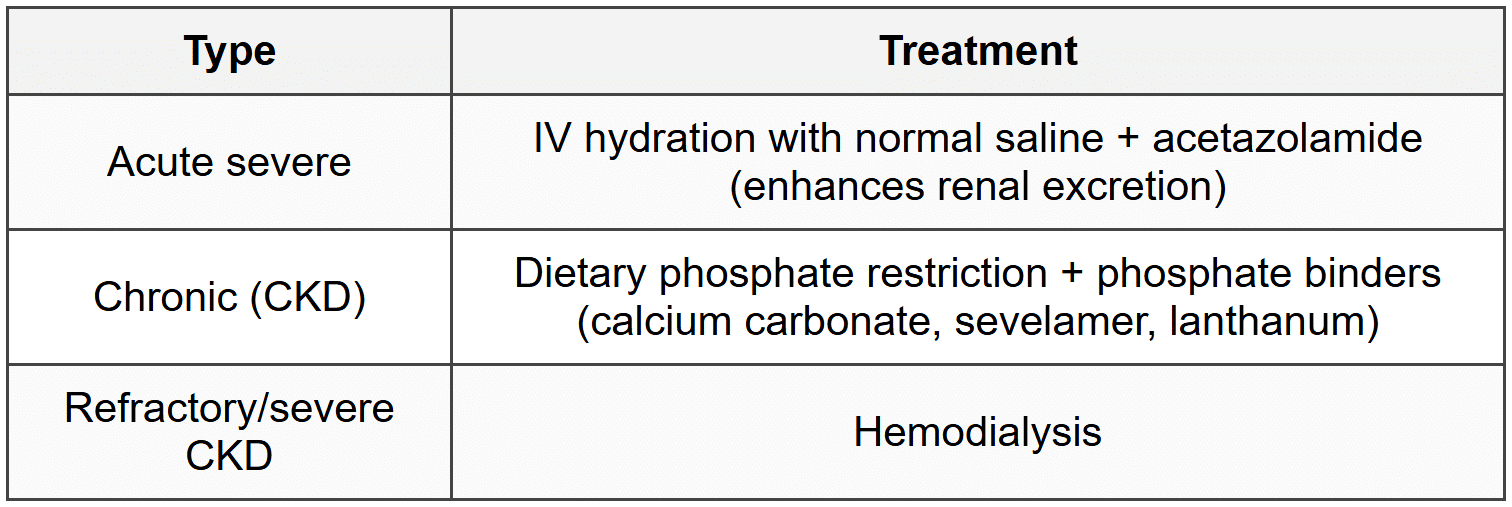
7.2.4 Treatment
8. Acid-Base Disorders
8.1 Normal Values and Definitions
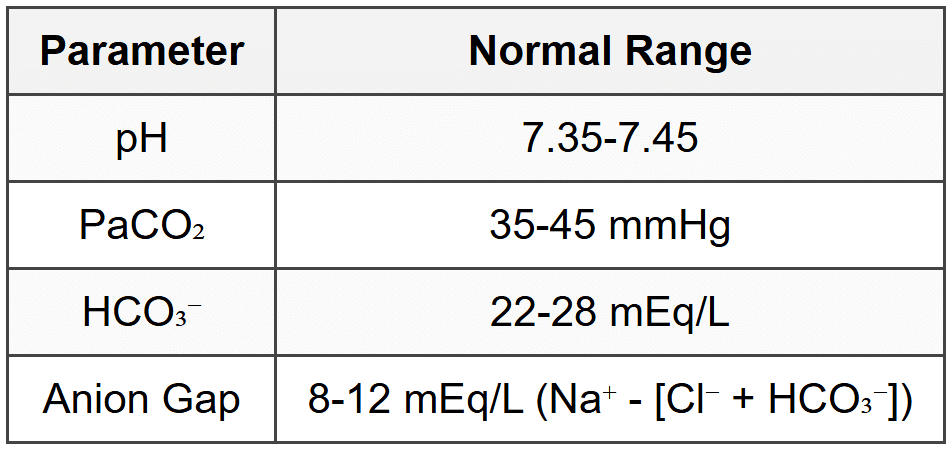
- Acidemia: pH < 7.35;="" alkalemia:="" ph=""> 7.45
- Acidosis: process that lowers pH; Alkalosis: process that raises pH
8.2 Metabolic Acidosis
8.2.1 High Anion Gap Metabolic Acidosis (MUDPILES)
- M: Methanol
- U: Uremia (renal failure)
- D: Diabetic ketoacidosis (DKA)
- P: Propylene glycol, Paraldehyde
- I: Iron, Isoniazid
- L: Lactic acidosis (Types A and B)
- E: Ethylene glycol
- S: Salicylates
8.2.2 Normal Anion Gap Metabolic Acidosis (Hyperchloremic)
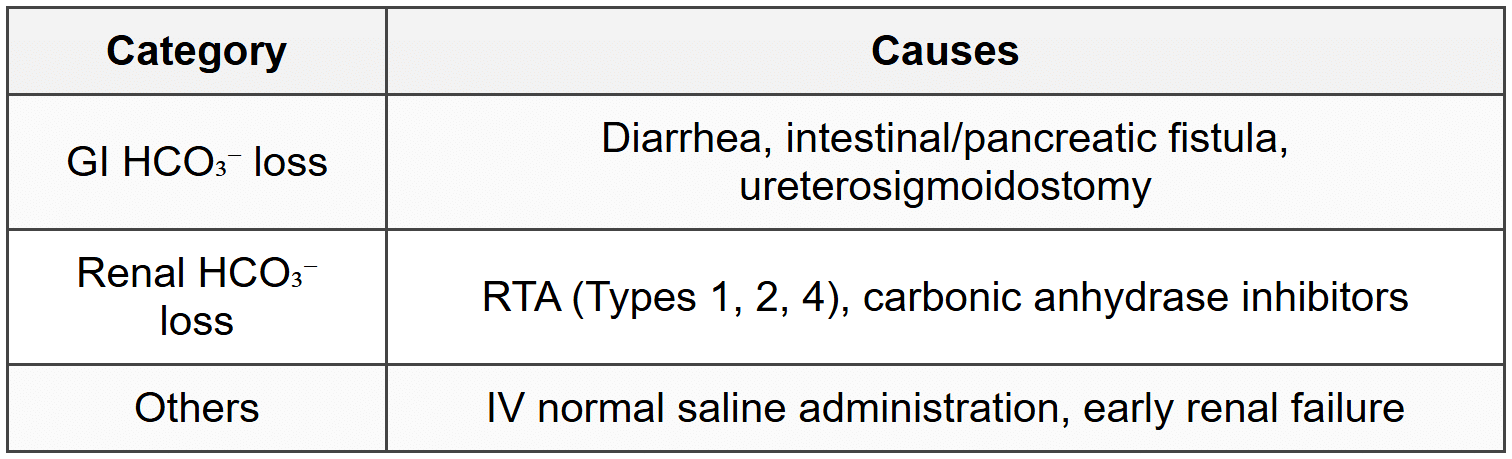
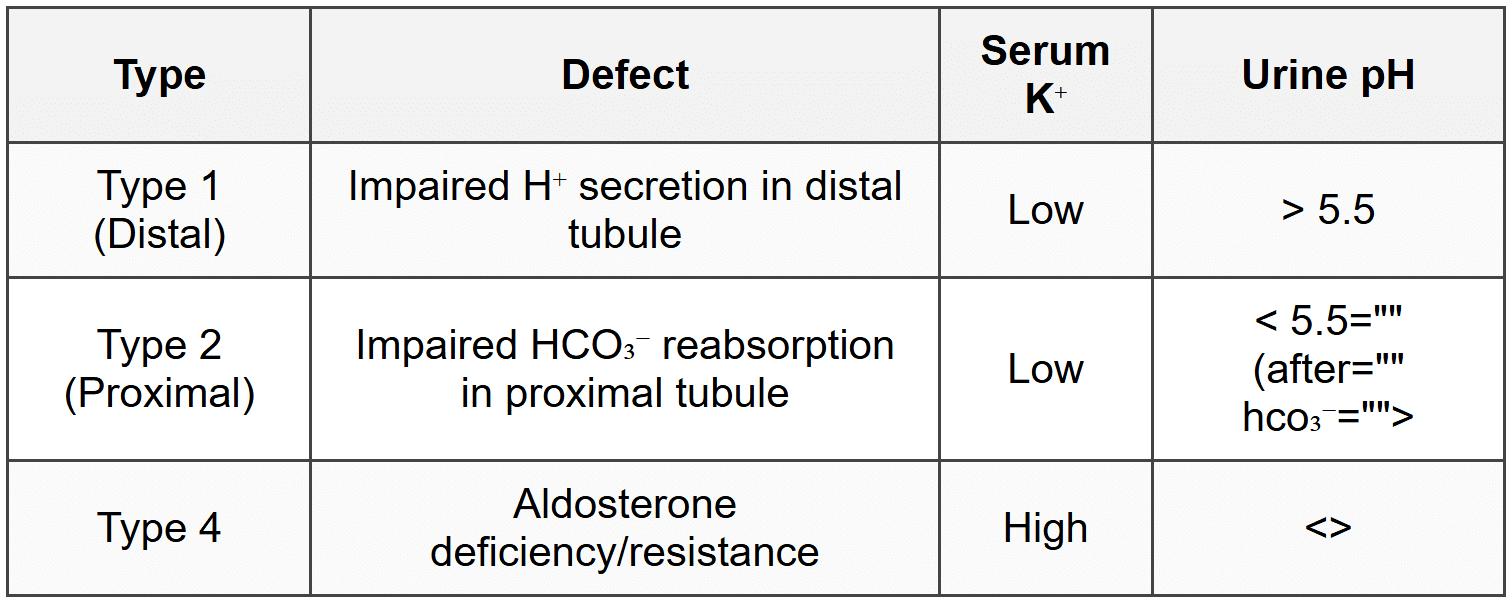
8.2.3 Renal Tubular Acidosis (RTA) Types
8.2.4 Compensation
- Expected PaCO₂ = 1.5 × HCO₃⁻ + 8 (±2) [Winter formula]
- PaCO₂ decreases by 1-1.3 mmHg for each 1 mEq/L decrease in HCO₃⁻
8.2.5 Treatment
- Treat underlying cause
- Sodium bicarbonate if pH < 7.1="" or="" severe="" symptoms="" (controversial="" in="" lactic="">
- Hemodialysis for severe cases, toxin removal
8.3 Metabolic Alkalosis
8.3.1 Saline-Responsive (Urine Cl⁻ < 20="">
- Vomiting, NG suction
- Diuretic use (remote)
- Post-hypercapnia
- Contraction alkalosis
8.3.2 Saline-Resistant (Urine Cl⁻ > 20 mEq/L)
- Hyperaldosteronism (primary, secondary)
- Cushing syndrome
- Current diuretic use
- Bartter/Gitelman syndrome
- Severe hypokalemia (< 2="">
8.3.3 Compensation
- PaCO₂ increases by 0.7 mmHg for each 1 mEq/L increase in HCO₃⁻
- PaCO₂ usually does not exceed 55 mmHg
8.3.4 Treatment
- Saline-responsive: IV normal saline, correct Cl⁻ and K⁺ deficits
- Saline-resistant: treat underlying cause, K⁺ supplementation, acetazolamide
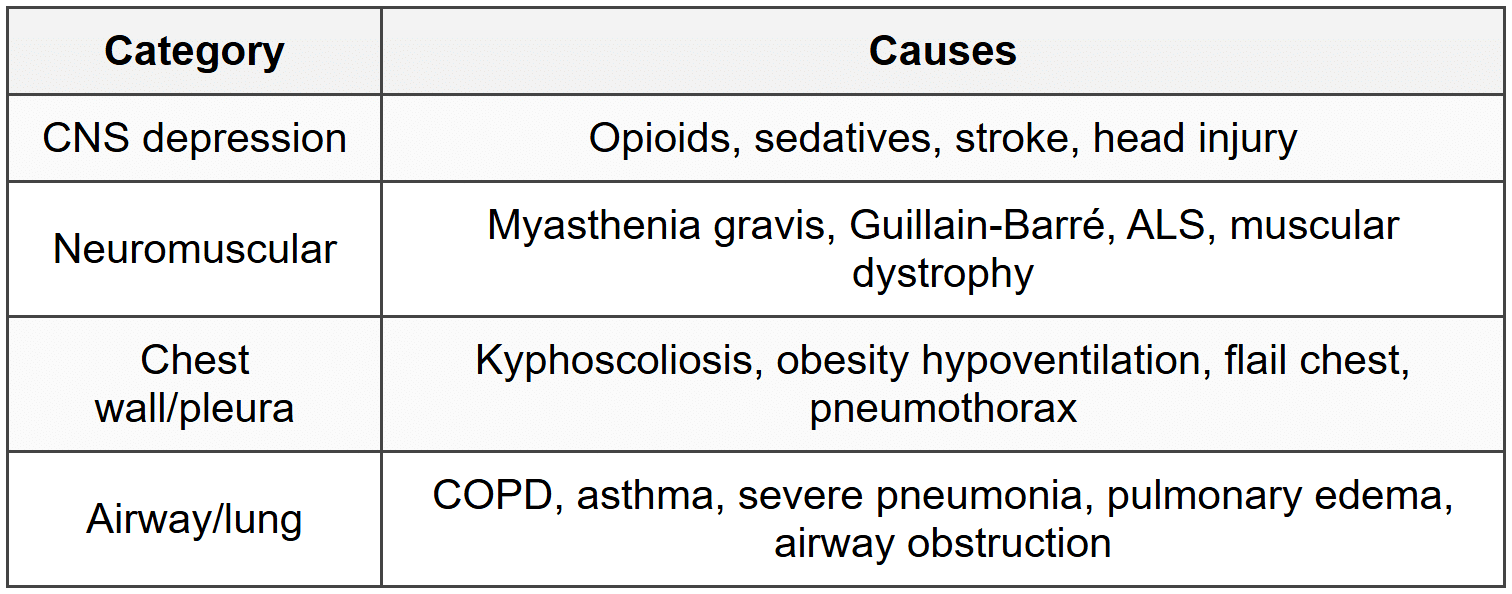
8.4 Respiratory Acidosis
8.4.1 Causes
8.4.2 Compensation
- Acute: HCO₃⁻ increases by 1 mEq/L for every 10 mmHg increase in PaCO₂
- Chronic: HCO₃⁻ increases by 3.5 mEq/L for every 10 mmHg increase in PaCO₂
8.4.3 Treatment
- Improve ventilation: treat underlying cause
- Mechanical ventilation if severe
- Avoid excessive bicarbonate (worsens CO₂ retention)
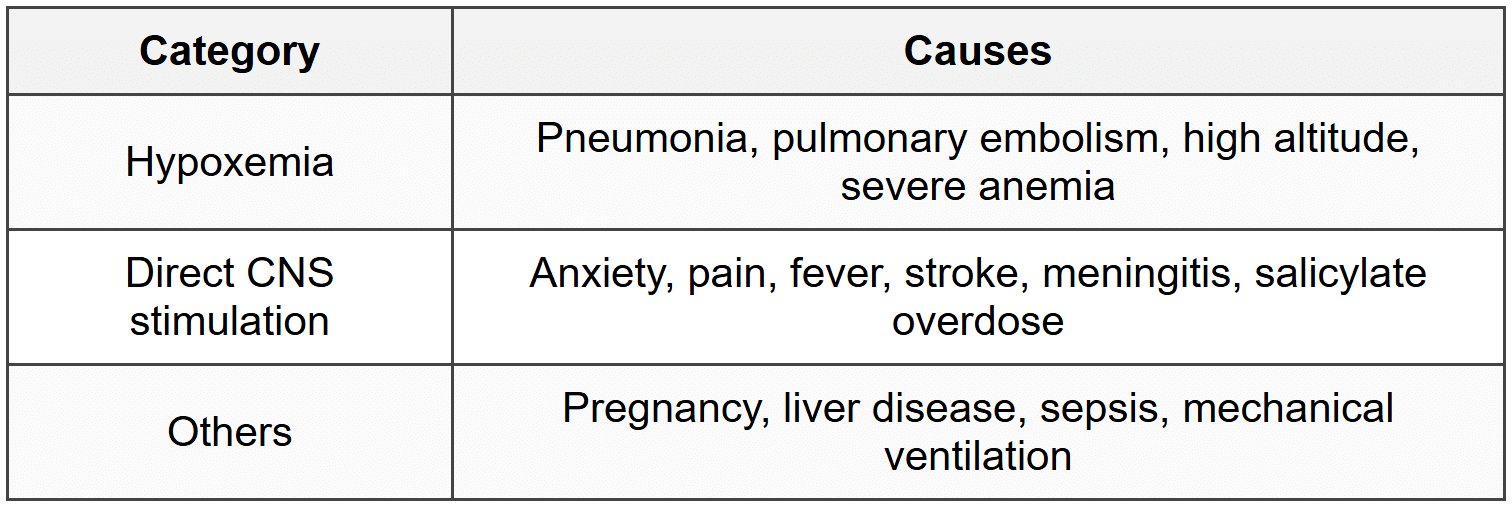
8.5 Respiratory Alkalosis
8.5.1 Causes
8.5.2 Compensation
- Acute: HCO₃⁻ decreases by 2 mEq/L for every 10 mmHg decrease in PaCO₂
- Chronic: HCO₃⁻ decreases by 5 mEq/L for every 10 mmHg decrease in PaCO₂
8.5.3 Treatment
- Treat underlying cause
- Reassurance (anxiety-induced hyperventilation)
- Adjust ventilator settings if mechanically ventilated
8.6 Stepwise Approach to ABG Analysis
- Check pH: acidemia (< 7.35)="" or="" alkalemia="" (=""> 7.45)
- Determine primary disorder: check PaCO₂ and HCO₃⁻
- Calculate anion gap (if metabolic acidosis)
- Assess compensation using formulas
- Check for mixed disorders: compensation incomplete or exceeds expected
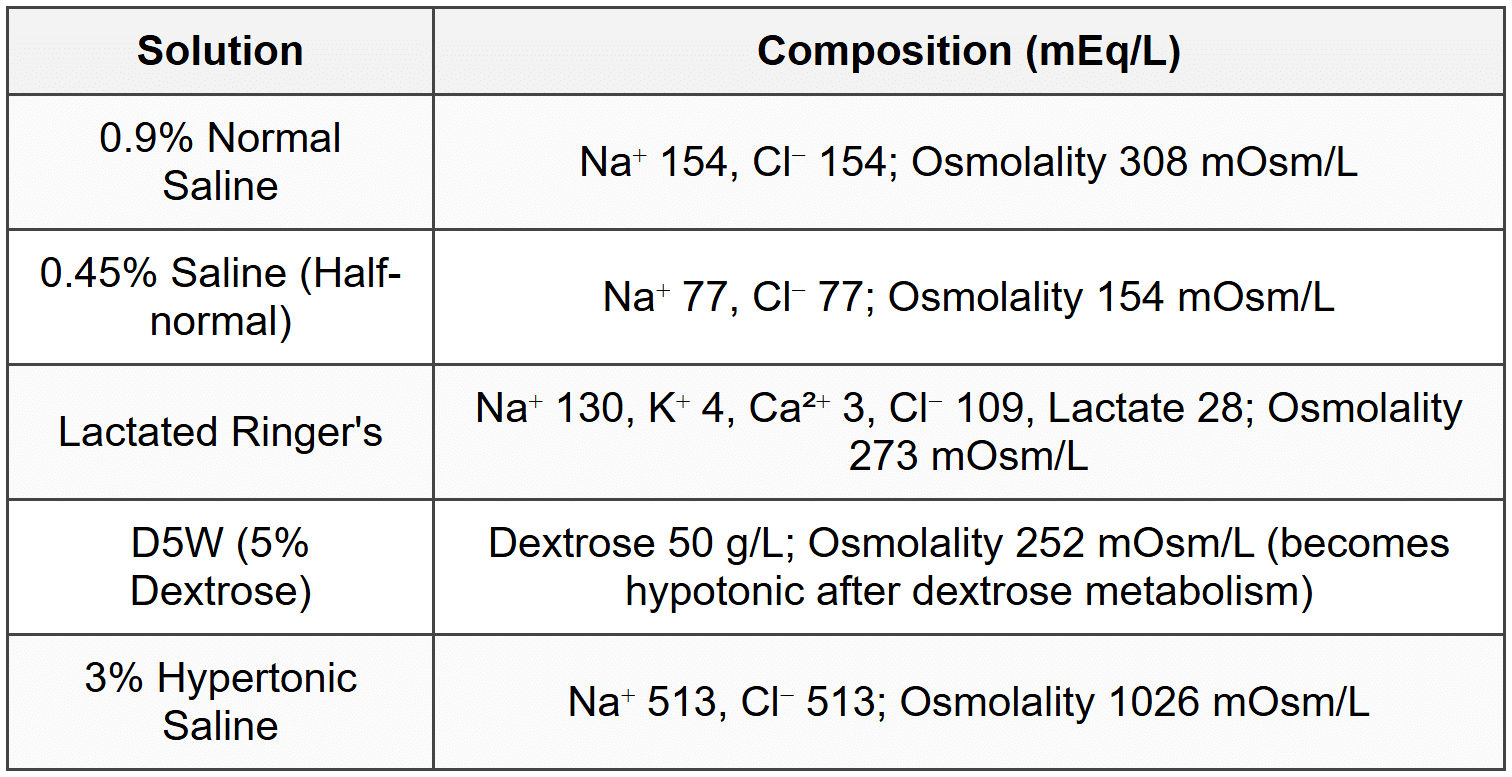
9. IV Fluid Therapy
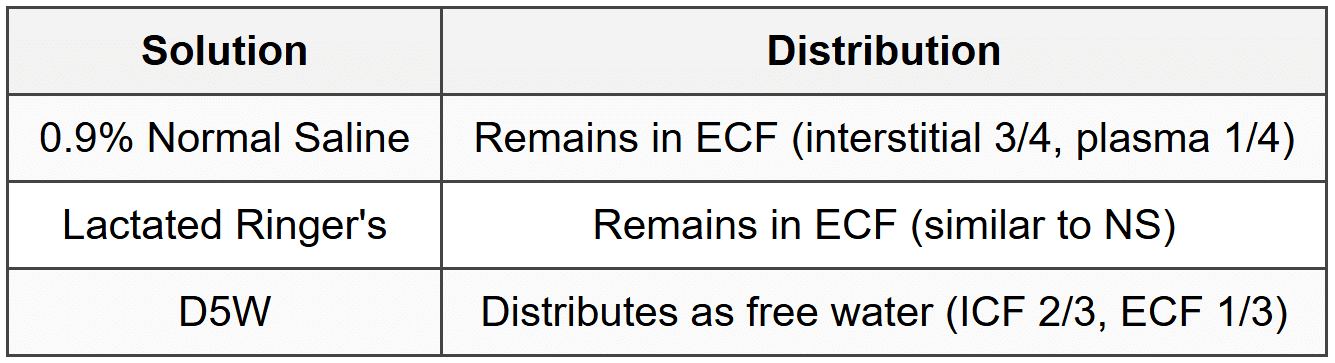
9.1 Crystalloid Solutions
9.2 Fluid Distribution After Infusion
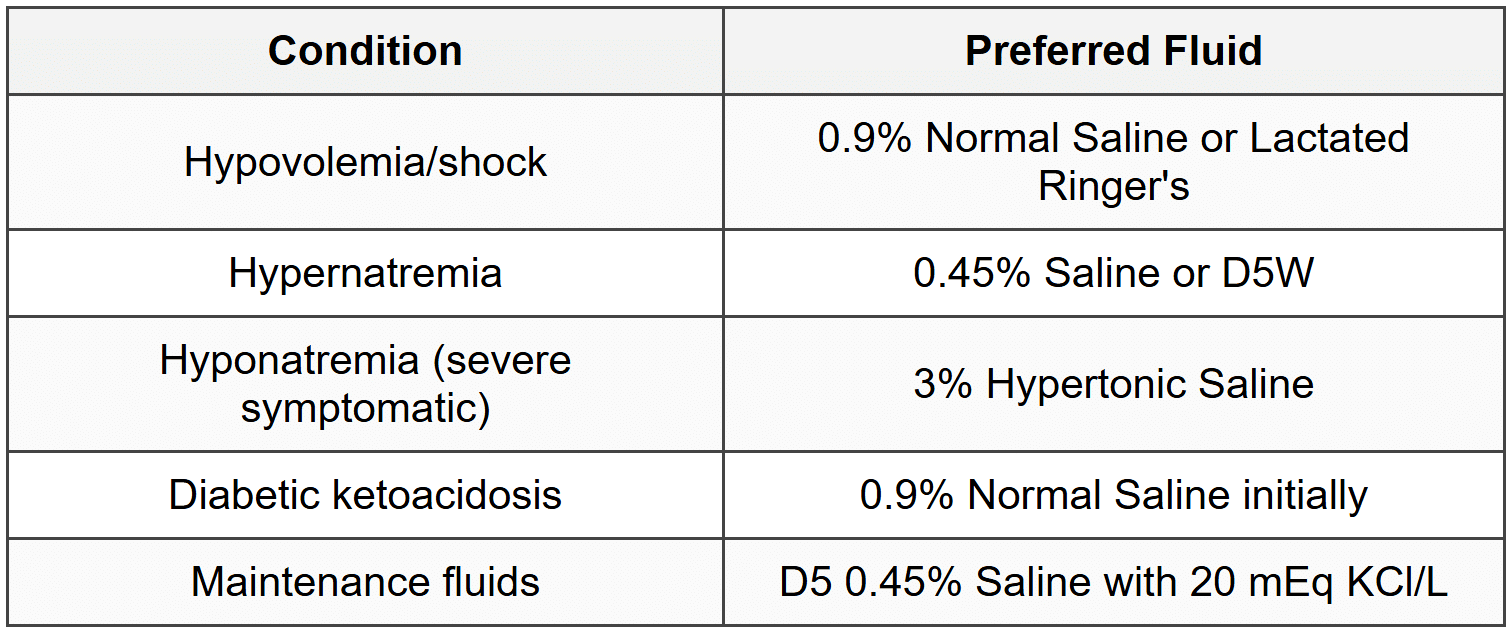
9.3 Clinical Indications
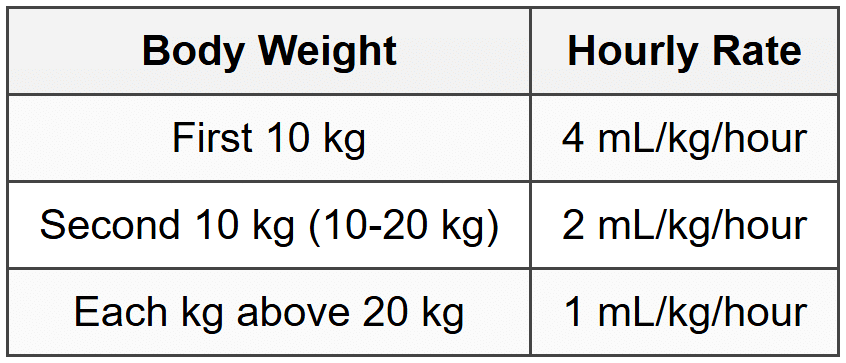
9.4 Maintenance Fluid Calculation (4-2-1 Rule)
9.5 Complications of IV Fluids
- 0.9% Normal Saline: hyperchloremic metabolic acidosis, hypernatremia
- Lactated Ringer's: contraindicated in hyperkalemia, hypercalcemia; can worsen lactic acidosis (theoretical)
- D5W: hyponatremia, hyperglycemia
- Fluid overload: pulmonary edema, peripheral edema, dilutional hyponatremia
10. Special Clinical Scenarios
10.1 Diabetic Ketoacidosis (DKA)
10.1.1 Electrolyte Abnormalities
- Hyperglycemia (> 250 mg/dL)
- High anion gap metabolic acidosis
- Hyperkalemia initially (transcellular shift due to acidosis and insulin deficiency)
- Total body potassium depleted (renal losses)
- Hypokalemia develops with treatment (insulin drives K into cells)
- Phosphate depletion (renal losses, shift into cells with insulin)
10.1.2 Fluid and Electrolyte Management
- IV normal saline 1-2 L in first hour
- Add potassium when K⁺ < 5.3="" meq/l="" and="" urine="" output="" adequate="" (20-40="" meq/l="" in="">
- Hold insulin if K⁺ < 3.3="" meq/l="" until="">
- Phosphate replacement if < 1="">
- Switch to D5 0.45% saline when glucose < 200="">
10.2 Tumor Lysis Syndrome
10.2.1 Laboratory Abnormalities
- Hyperkalemia, hyperphosphatemia, hyperuricemia
- Hypocalcemia (secondary to hyperphosphatemia)
- High anion gap metabolic acidosis
- Acute kidney injury
10.2.2 Management
- Aggressive IV hydration (normal saline 200-300 mL/hour)
- Rasburicase (recombinant urate oxidase) for hyperuricemia
- Avoid allopurinol (less effective, metabolites can worsen renal injury)
- Correct hyperkalemia (as per hyperkalemia protocol)
- Phosphate binders for hyperphosphatemia
- Hemodialysis if refractory or anuric
10.3 Refeeding Syndrome
10.3.1 Pathophysiology
- Occurs with reintroduction of nutrition after prolonged starvation
- Insulin surge drives electrolytes into cells
10.3.2 Electrolyte Abnormalities
- Hypophosphatemia (hallmark)
- Hypokalemia, hypomagnesemia
- Thiamine deficiency (Wernicke encephalopathy risk)
10.3.3 Prevention and Management
- Start refeeding slowly (25-50% of caloric needs initially)
- Thiamine supplementation before refeeding
- Aggressive electrolyte monitoring and replacement
- Monitor phosphate, potassium, magnesium daily
10.4 Syndrome of Inappropriate ADH (SIADH)
10.4.1 Common Causes
- CNS disorders: meningitis, encephalitis, head trauma, stroke, SAH
- Pulmonary: pneumonia, TB, aspergillosis, positive pressure ventilation
- Malignancy: small cell lung cancer (ectopic ADH)
- Drugs: SSRIs, carbamazepine, cyclophosphamide, NSAIDs, ecstasy
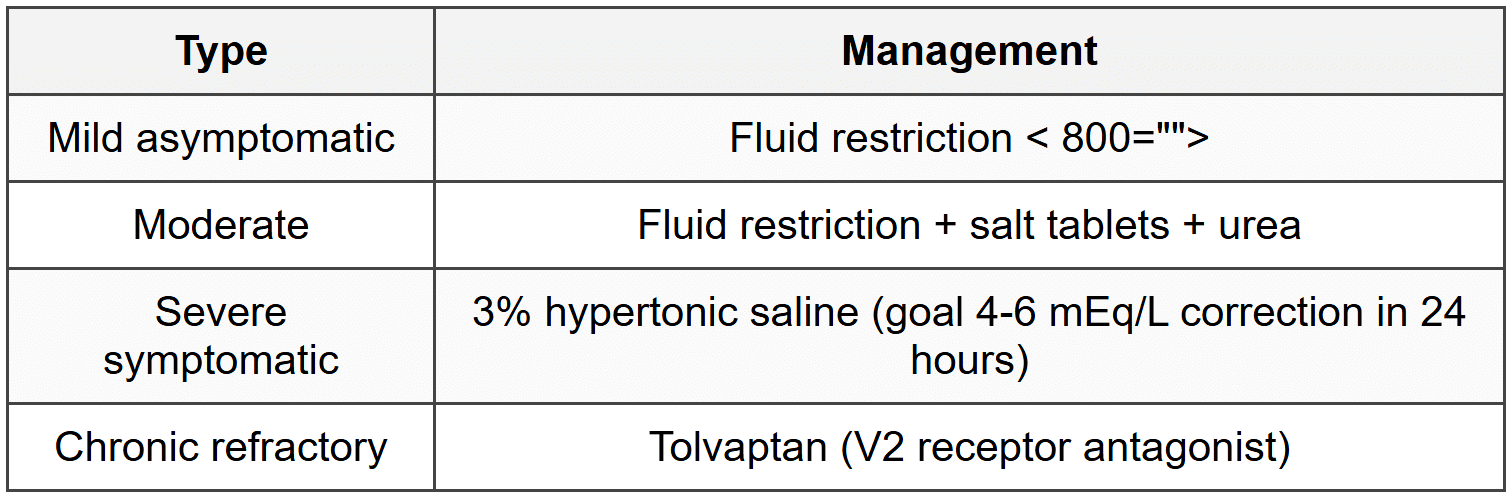
10.4.2 Management by Severity
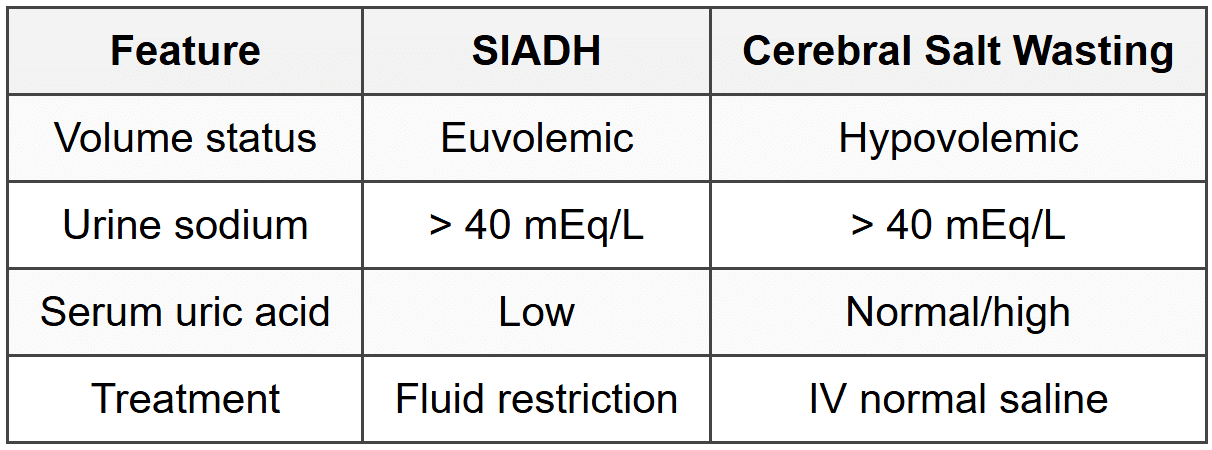
10.5 Cerebral Salt Wasting vs SIADH
About this Document

4.77/5 Rating

Apr 26, 2026 Last updated
Related Exams
Document Description: CheatSheet: Fluids and Electrolytes for NEET PG 2026 is part of Medicine preparation. The notes and questions for CheatSheet: Fluids and Electrolytes have been prepared according to the NEET PG exam syllabus. Information about CheatSheet: Fluids and Electrolytes covers topics like and CheatSheet: Fluids and Electrolytes Example, for NEET PG 2026 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for CheatSheet: Fluids and Electrolytes.
Introduction of CheatSheet: Fluids and Electrolytes in English is available as part of our Medicine for NEET PG & CheatSheet: Fluids and Electrolytes in Hindi for Medicine course. Download more important topics related with notes, lectures and mock test series for NEET PG Exam by signing up for free. NEET PG: CheatSheet: Fluids and Electrolytes
Description
CheatSheet: Fluids & Electrolytes of Medicine to help you remember important concepts with short tricks. Start learning for NEET PG exam & improve retention with EduRev.
Information about CheatSheet: Fluids and Electrolytes
In this doc you can find the meaning of CheatSheet: Fluids and Electrolytes defined & explained in the simplest way possible. Besides explaining types of CheatSheet: Fluids and Electrolytes theory, EduRev gives you an ample number of questions to practice CheatSheet: Fluids and Electrolytes tests, examples and also practice NEET PG tests


Related Searches
CheatSheet: Fluids and Electrolytes, Exam, CheatSheet: Fluids and Electrolytes, practice quizzes, Semester Notes, shortcuts and tricks, video lectures, Important questions, ppt, Summary, Free, past year papers, Previous Year Questions with Solutions, CheatSheet: Fluids and Electrolytes, MCQs, pdf , Sample Paper, mock tests for examination, Extra Questions, study material, Objective type Questions, Viva Questions;