NCERT Solutions: Breathing & Exchange of Gases

Q1: Define vital capacity. What is its significance?
Ans: Vital capacity is the maximum volume of air that can be expelled from the lungs after taking the deepest possible inspiration. In an average adult human, it is about 3.5-4.5 litres, though the exact value varies with age, sex, body size and physical conditioning.
Significance:
- It indicates the maximal ventilatory capacity of the lungs and is used clinically to assess lung function and respiratory health.
- A higher vital capacity improves the supply of fresh oxygen to the alveoli and helps remove a larger proportion of carbon dioxide-rich air, thereby enhancing gaseous exchange.
- Reduced vital capacity may indicate restrictive or obstructive lung disorders or decreased chest wall mobility.
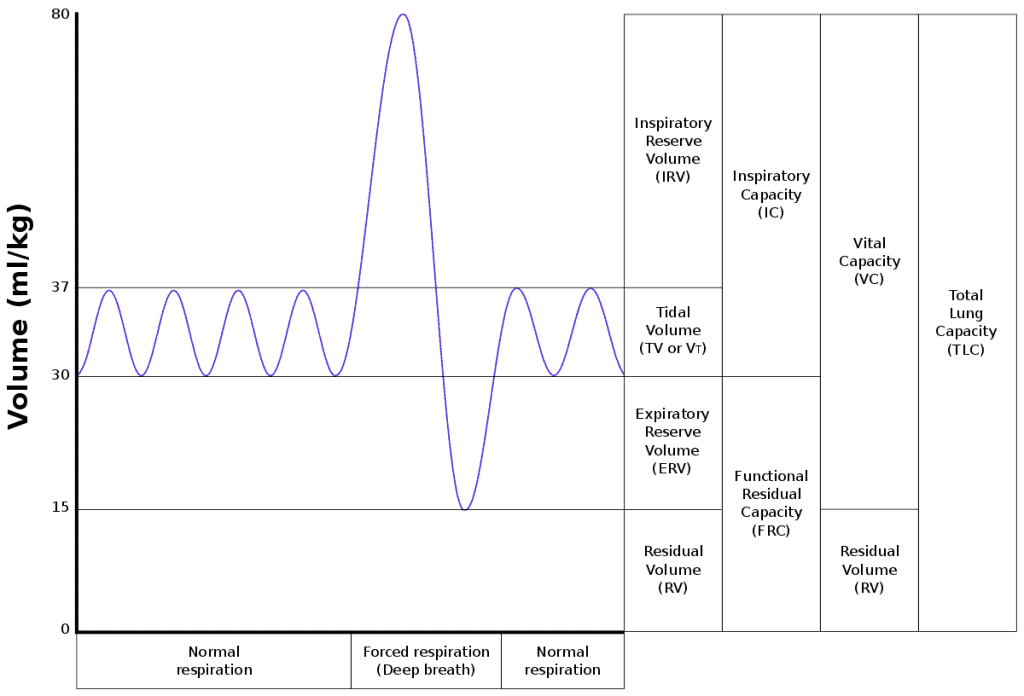 Vital Capacity Curve
Vital Capacity Curve
Q2: State the volume of air remaining in the lungs after a normal breathing.
Ans: The volume of air remaining in the lungs after a normal expiration is called the functional residual capacity (FRC). It is the sum of:
- Expiratory reserve volume (ERV): the extra volume that can be forcibly exhaled after a normal expiration - about 1000-1500 mL.
- Residual volume (RV): the volume left in the lungs even after a maximal expiration - about 1100-1500 mL.
Therefore, FRC = ERV + RV ≈ (1000-1500) + (1100-1500) mL ≈ 2500-3000 mL. This residual air prevents lung collapse and maintains continuous gas exchange between breaths.
Q3: Diffusion of gases occurs in the alveolar region only and not in the other parts of respiratory system. Why?
Ans:
- Each alveolus has a very thin lining of squamous epithelial cells and is surrounded by an extensive network of blood capillaries that also have thin walls. This thin barrier (alveolar epithelium + capillary endothelium) allows gases to diffuse rapidly.
- Alveoli provide a very large surface area for exchange and keep the surface moist, which favours diffusion of O2 and CO2.
- Other parts of the respiratory tract (nose, trachea, bronchi) have thicker walls, cartilage rings, ciliated epithelium and mucus - structures suited for air cleaning, warming and humidification, not rapid gas diffusion.
- Because of the difference in partial pressures of gases between alveolar air and blood, O2 diffuses into blood while CO2 diffuses out, across this thin alveolar-capillary barrier by simple diffusion.
Q4: What are the major transport mechanisms for CO2? Explain.
Ans: Carbon dioxide is transported from tissues to lungs by three main mechanisms. Plasma and red blood cells both participate.

(1) Dissolved in plasma: About ~7% of CO2 is carried dissolved directly in the plasma because CO2 is moderately soluble in water. Some CO2 also reacts with water to form carbonic acid (H2CO3), but this conversion is relatively slow without enzymatic help.
Since the uncatalysed formation of carbonic acid is slow, only a small fraction is present as dissolved gas.
(2) As carbaminohaemoglobin in RBCs: About 20-25% of CO2 is transported bound to haemoglobin, but not at the iron site. CO2 binds to the amino groups of the globin chains to form carbaminohaemoglobin. This form is reversible and releases CO2 at the lungs.
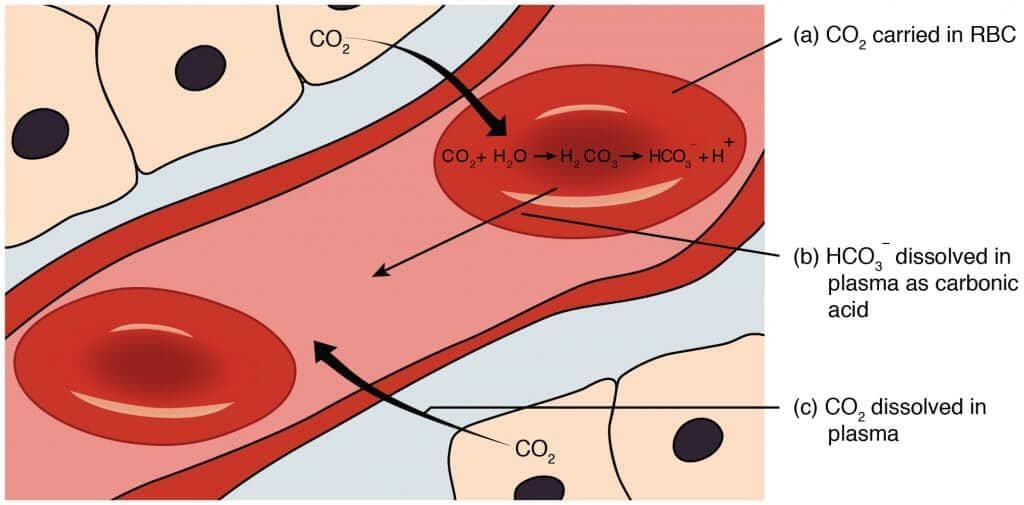 Transportation of CO2 through RBCs
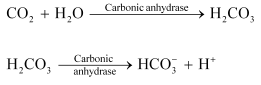
Transportation of CO2 through RBCs(3) As bicarbonate (HCO3-) - the major route: About ~70% of CO2 is transported as bicarbonate in plasma. In red blood cells, the enzyme carbonic anhydrase (a zinc-containing enzyme) rapidly catalyses:
CO2 + H2O ⇌ H2CO3 ⇌ H+ + HCO3-
Bicarbonate ions diffuse out of RBCs into plasma and are carried to lungs. To maintain electrical neutrality, chloride ions move into RBCs in exchange for bicarbonate (the chloride shift). At the lungs the reactions reverse and CO2 is released and exhaled.
Q5: What will be the pO2 and pCO2 in the atmospheric air compared to those in the alveolar air?
(i) pO2 lesser, pCO2 higher
(ii) pO2 higher, pCO2 lesser
(iii) pO2 higher, pCO2 higher
(iv) pO2 lesser, pCO2 lesser
Ans: (ii)
Explanation: Atmospheric air contains dry air with a high partial pressure of oxygen, about 159 mm Hg at sea level. By the time air reaches the alveoli, it is mixed with residual air, humidified and partly replaced by CO2 coming from blood; therefore alveolar pO2 is lower, approximately 104 mm Hg. Conversely, atmospheric pCO2 is very low (~0.3 mm Hg), while alveolar pCO2 is much higher (~40 mm Hg) because CO2 diffuses from blood into alveoli. These differences drive diffusion of O2 into blood and CO2 out of blood.
Q6: Explain the process of inspiration under normal conditions.
Ans:
- Inspiration is the active process of drawing air into the lungs by creating a pressure difference between the atmosphere and the alveoli.
- During quiet inspiration the diaphragm contracts and moves downward (toward the abdominal cavity), increasing the vertical dimension of the thoracic cavity. Simultaneously the external intercostal muscles contract, lifting the ribs and sternum to increase the anteroposterior and lateral dimensions of the thorax.
- Because the lungs are attached to the thoracic wall by the pleural membranes, an increase in thoracic volume causes the lungs to expand and pulmonary volume to increase.
- Expansion of the lungs lowers the intrapulmonary (intra-alveolar) pressure slightly below atmospheric pressure, so air flows into the lungs along the pressure gradient until pressures equalise.
- In quiet breathing the volume change per breath is small (tidal volume). Deeper inspiration uses accessory muscles (sternocleidomastoids, scalenes) to further increase thoracic volume.
Q7: How is respiration regulated?
Ans:
- The basic rhythm of breathing is generated by the respiratory rhythm centre in the medulla oblongata. Groups of neurons here set the rate and depth of breathing.
- The pneumotaxic centre (in the pons) can modify this rhythm by limiting inspiration and thus regulating respiratory rate and pattern.
- Chemoreceptors in and near the respiratory centres (central chemoreceptors) respond mainly to changes in CO2 and pH (H+) in the cerebrospinal fluid and stimulate the centre to increase ventilation when CO2 or H+ rise.
- Peripheral chemoreceptors in the carotid and aortic bodies detect changes in arterial pO2, pCO2 and pH and send signals to the respiratory centre to alter breathing when necessary.
- Reflexes from lung stretch receptors and higher brain centres (voluntary control, emotions) also influence respiration.
Q8: What is the effect of pCO2 on oxygen transport?
Ans: Partial pressure of carbon dioxide (pCO2) strongly influences how readily haemoglobin picks up or releases oxygen - a phenomenon closely related to the Bohr effect. Key points:
- At the alveoli: low pCO2 and high pO2 promote the formation of oxyhaemoglobin so oxygen binds to haemoglobin.
- At the tissues: high pCO2 (and lower pO2) reduce haemoglobin's affinity for oxygen, favouring oxygen release from oxyhaemoglobin.
- Thus, a decrease in pCO2 increases haemoglobin's affinity for O2, and an increase in pCO2 facilitates dissociation of O2 where it is needed.
Q9: What happens to the respiratory process in a man going up a hill?
Ans: As altitude increases, the atmospheric partial pressure of oxygen (pO2) falls. Consequences include:
- Each breath brings in less oxygen, so arterial oxygen content falls.
- The respiratory centre responds by increasing the rate and depth of breathing (hyperventilation) to take in more oxygen.
- Heart rate and cardiac output also increase to transport available oxygen more rapidly to tissues.
- Over days to weeks the body acclimatises (for example, by increasing red blood cell production) but initially the main responses are faster breathing and increased heart rate.
Q10: What is the site of gaseous exchange in an insect?
Ans: In insects gaseous exchange occurs through the tracheal system. Air enters the body through small external openings called spiracles, passes into larger tubes called tracheae and then into finer branches called tracheoles. The tracheoles reach very close to or into body cells and have thin walls, allowing direct diffusion of oxygen into cells and of carbon dioxide out. The spiracles can open and close to regulate airflow and reduce water loss.
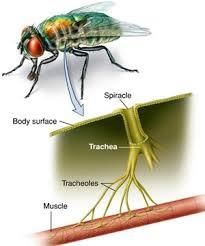
The movement of carbon dioxide follows the reverse path. The CO2 from the cells of the body first enters the tracheae and then leaves the body through the spiracles.
Q11: Define oxygen dissociation curve. Can you suggest any reason for its sigmoidal pattern?
Ans:
The oxygen dissociation curve is a graph that shows the percentage saturation of haemoglobin with oxygen (oxyhaemoglobin) at different partial pressures of oxygen (pO2).
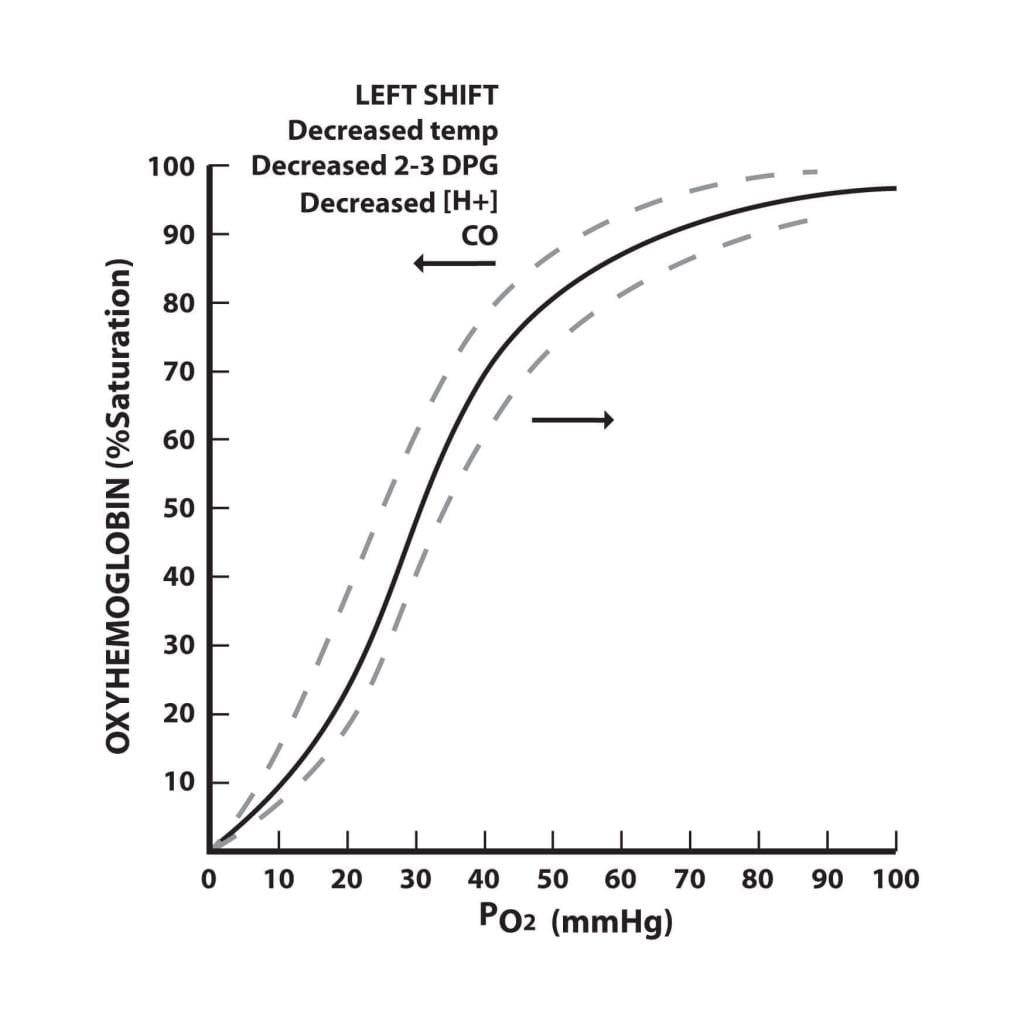
- At high pO2 (lungs) haemoglobin readily binds O2 to form oxyhaemoglobin; at low pO2 (tissues) it releases O2.
- The curve is sigmoidal (S-shaped) because of cooperative binding: when one O2 molecule binds to a haemoglobin subunit, it increases the affinity of the remaining subunits for O2, making subsequent binding easier. This cooperative behaviour produces the characteristic sigmoid shape and allows efficient loading in the lungs and unloading in the tissues.
Q12: Have you heard about hypoxia? Try to gather information about it, and discuss with your friends.
Ans: Hypoxia is a condition in which tissues are not receiving adequate oxygen. It may arise from different causes and is classified into several types:
Hypoxemic hypoxia: Caused by low arterial pO2, for example at high altitudes or in lung diseases where gas exchange is impaired.
Anaemic hypoxia: Occurs when the oxygen-carrying capacity of blood is reduced due to low haemoglobin concentration or dysfunctional haemoglobin (for example, anaemia or CO poisoning).
Stagnant (ischaemic) hypoxia: Due to poor blood flow (reduced perfusion) so oxygen cannot reach tissues adequately - for example in heart failure or local ischaemia. Prolonged exposure to cold can also reduce circulation.
Histotoxic hypoxia: Tissues are unable to use available oxygen, often due to metabolic poisons such as cyanide or because of certain enzyme defects.
Q13: Distinguish between
(a) IRV and ERV
(b) Inspiratory capacity and Expiratory capacity
(c) Vital capacity and Total lung capacity
Ans: (a) IRV and ERV
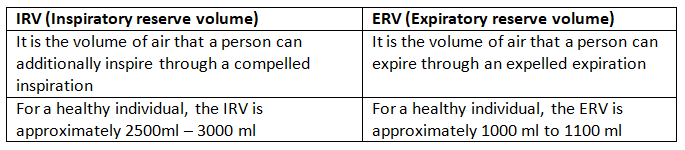
- Inspiration reserve volume (IRV): additional volume that can be forcibly inhaled after a normal inspiration (approx. 1900-3100 mL depending on the person).
- Expiratory reserve volume (ERV): additional volume that can be forcibly exhaled after a normal expiration (approx. 1000-1500 mL).
- IRV is the extra air taken in above the tidal volume, while ERV is the extra air pushed out beyond a normal exhalation.
(b) Inspiratory capacity and Expiratory capacity
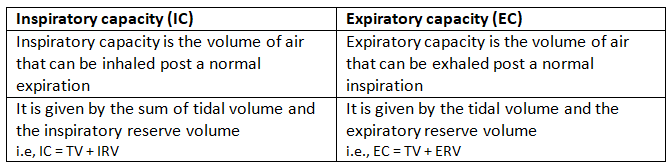
- Inspiratory capacity (IC) = Tidal volume (TV) + Inspiratory reserve volume (IRV). It is the maximum volume that can be inspired after a normal expiration.
- Expiratory capacity is not a standard single term in spirometry but commonly refers to volumes available for active expiration; many texts use FRC (functional residual capacity) or ERV depending on context. (When contrasted with IC, the complementary volumes are ERV and RV which together form FRC.)
(c) Vital capacity and Total lung capacity
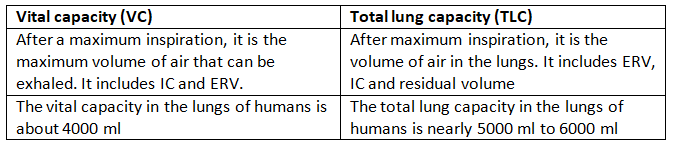
- Vital capacity (VC) = IRV + TV + ERV. It is the maximum volume that can be exhaled after a maximal inspiration (≈ 3.5-4.5 L).
- Total lung capacity (TLC) = VC + Residual volume (RV). It is the total volume the lungs can hold after a maximal inspiration (≈ 5-6 L in an average adult).
- Thus, VC is the usable portion of lung volume that can be exchanged, while TLC includes the residual air that cannot be voluntarily expelled.
Q14: What is Tidal volume? Find out the Tidal volume (approximate value) for a healthy human in an hour.
Ans: Tidal volume (TV) is the volume of air inspired or expired during a normal quiet breath. For an average healthy adult the tidal volume is about ~500 mL per breath.
To estimate the total tidal air moved in an hour, use a typical resting respiratory rate of 12-16 breaths per minute:
Minute ventilation = TV × respiratory rate ≈ 500 mL × (12-16) ≈ 6000-8000 mL/min (i.e. 6-8 L/min).
Tidal volume in an hour = 6-8 L/min × 60 min = 360-480 L = 3.6 × 105 to 4.8 × 105 mL.
Therefore, a healthy person at rest moves approximately 3.6 × 105 to 4.8 × 105 mL of tidal air in one hour, depending on breathing rate.
FAQs on NCERT Solutions: Breathing & Exchange of Gases
| 1. What is the process of breathing? |  |
| 2. How does the exchange of gases occur in the lungs? | |
| 3. What are the main respiratory organs involved in breathing? | |
| 4. How does the respiratory system help in maintaining the body's pH balance? | |
| 5. What are some common respiratory disorders that affect breathing? | |