Arrhythmias and Emergency Medicine- 1 - Free MCQ Practice Test with solutions,
MCQ Practice Test & Solutions: Test: Arrhythmias and Emergency Medicine- 1 (30 Questions)
You can prepare effectively for NEET PG Medicine with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Arrhythmias and Emergency Medicine- 1". These 30 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 30 minutes
- - Number of Questions: 30
Sign up on EduRev for free to attempt this test and track your preparation progress.

A patient presents with recent onset breathlessness and ECG was done. The diagnosis is? (AIIMS May 2019, Nov 2018)
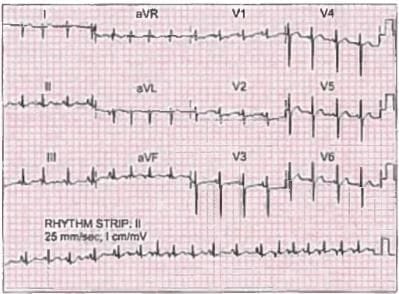
Detailed Solution: Question 1


Which of the following is the most common heart block in neonatal lupus. (Recent Pattern 2014-15)
Detailed Solution: Question 2

True about Torsades de pointes? (Recent Pattern 2014-15)
Detailed Solution: Question 3
A 40-year-old male presents to the office with a history of palpitations that last for a few seconds and occur two or three times a week. There are no other symptoms. ECG shows a single unifocal premature ventricular contraction. The most likely cause of this finding is: (Recent Pattern 2014-15)
Detailed Solution: Question 4
A 78-year-old male with hypertension (controlled on antihypertensive drugs) presents with new onset of mild left hemiparesis and ECG finding of atrial fibrillation. Which of the following must be done? (Recent Pattern 2014-15)
Detailed Solution: Question 5
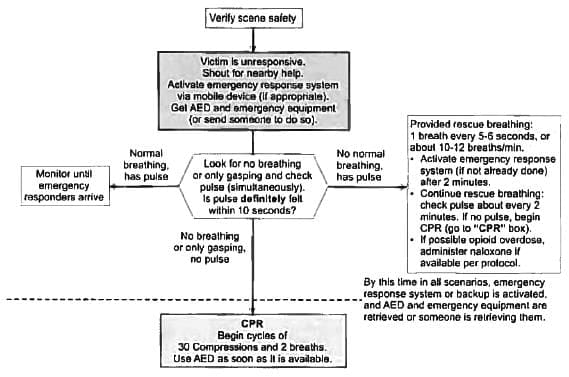
While at the ward round, you see an elderly lady attendant slump to the floor. Going to her aid, you notice her to be unresponsive and apneic. Your first step in Adult Basic Life Support(CPR) should be the following?
Detailed Solution: Question 6
In the ICU, a patient suddenly becomes unresponsive, pulseless, and hypotensive, with cardiac monitor indicating ventricular tachycardia. The first therapeutic step among the following should be: (Recent Pattern 2014-15)
Detailed Solution: Question 7
A 12-year-old wheel chair bound boy with scoliosis has presented with Dyspnea. ECG shows deep QS waves in V₂, V₃ with tall R waves in V₅, V₆. Probable diagnosis: (Recent Pattern 2014-15)
Detailed Solution: Question 8
Treatment of asymptomatic bradycardia is: (Recent Pattern 2014-15)
Detailed Solution: Question 9
Which is incorrect about a pacemaker: (Recent Pattern 2014-15)
Detailed Solution: Question 10
Frog sign is seen in: (Recent Pattern 2014-15)
Detailed Solution: Question 11
Sinus Bradycardia is defined as heart rate of? (Recent Pattern 2014-15)
Detailed Solution: Question 12
A person with mitral regurgitation and atrial fibrillation presents with syncope. On examination the person has a heart rate of 55. What is the most probable cause? (Recent Pattern 2014-15)
Detailed Solution: Question 13
Congenital long QT syndrome causes death due to? (Recent Pattern 2014-15)
Detailed Solution: Question 14
All are true about WPW syndrome except? (Recent Pattern 2014-IS)
Detailed Solution: Question 15
Broad complex tachycardia, due to ventricular tachycardia is suggested by all except? (Recent Pattern 2014-15)
Detailed Solution: Question 16
Drug of choice in maintenance therapy in P.S.V.T is: (Recent Pattern 2014-15)
Detailed Solution: Question 17
The drug of choice in patients with Wolff-Parkinson-White syndrome with atrial fibrillation is: (AIIMS Nov 2003)
Detailed Solution: Question 18
All of the following are features of Mobitz Type I block, except: (AI-1992)
Detailed Solution: Question 19
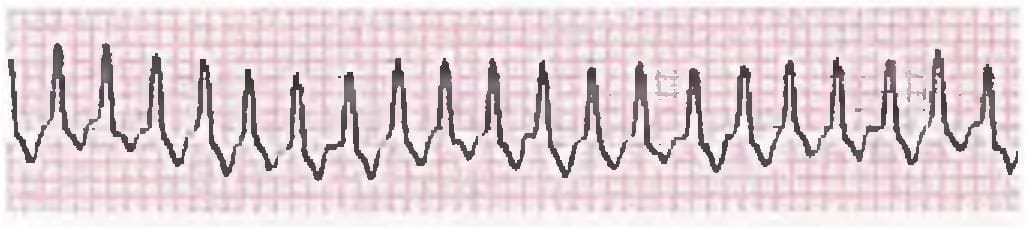
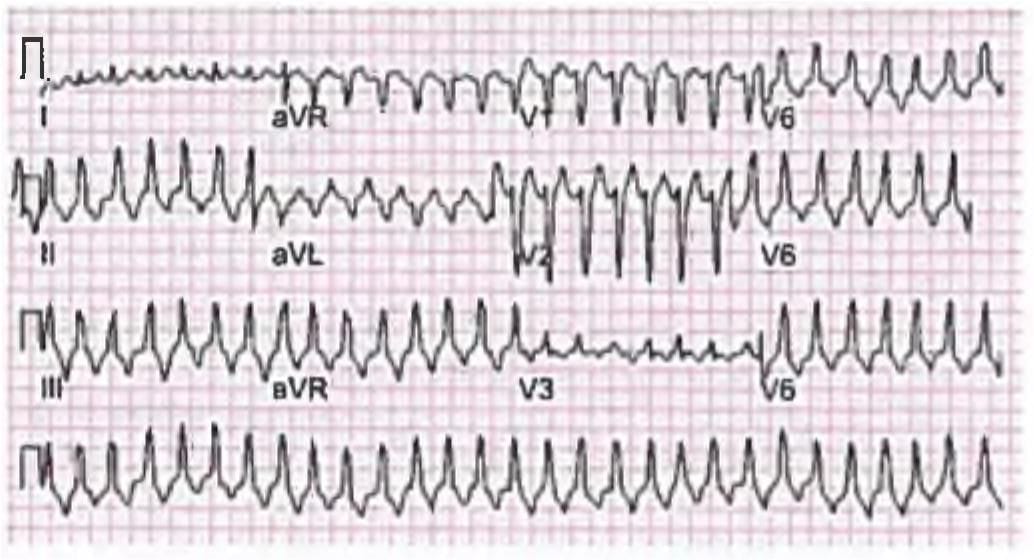
A 25-year-old female presented to ER unconscious. Her mother tells you about her having recurrent episodes of syncopal episodes. Her BP is 80/60 mm Hg and you order an ECG. Treatment is? (Recent Question 2019)
Detailed Solution: Question 20
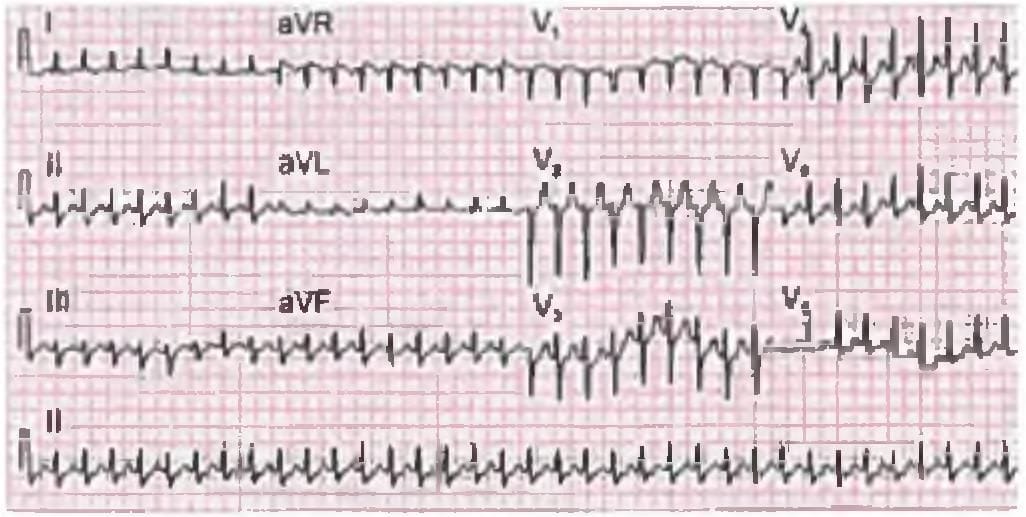
Comment on the diagnosis of the patient? (Recent Question 2019)
Detailed Solution: Question 21
Which of the following is assoclated with AV block? (Recent Pattern 2018)
Detailed Solution: Question 22
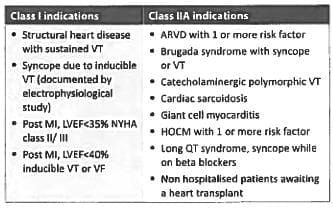
Implantable cardioverter defibrillator is useful in? (Recent Pattern 2018)
Detailed Solution: Question 23
Heart block is seen with all except? (Recent Pattern 2018)
Detailed Solution: Question 24
What is the correct sequence of events according to BLS? (AIMS Nov 2017)
Detailed Solution: Question 25
A patient has presented with complaints of amblyopin, episodes of palpitations and occasional exertional chest pain. ECG shows ventricular extra systoles. Which of the following is the probable cause? (AIIMS May 2017)
Detailed Solution: Question 26
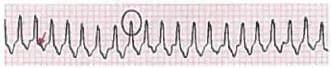
This 50-year-old patient developed syncope after having a coffee. ECG was done. Which is the most appropriate therapy for a patient suffering from the condition shown below? (AIIMS May 2017)
Detailed Solution: Question 27
Which of the following statements about premature ventricular beat is false? (Recent Pattern 2014-15)
Detailed Solution: Question 28
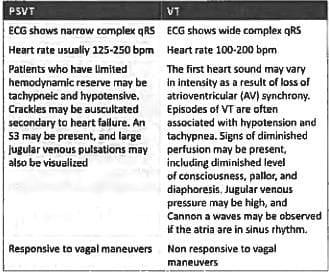
All of the following features can differentiate between ventricular tachycardia and supraventricular tachycardia except: (Recent Pattern 2014-15)
Detailed Solution: Question 29
Feature of Torsades de pointes is: (Recent Pattern 2014-15)
Detailed Solution: Question 30
50 docs|64 tests |