Bronchial Asthma - Free MCQ Practice Test with solutions, NEET PG Medicine
MCQ Practice Test & Solutions: Test: Bronchial Asthma (30 Questions)
You can prepare effectively for NEET PG Medicine with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Bronchial Asthma". These 30 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 30 minutes
- - Number of Questions: 30
Sign up on EduRev for free to attempt this test and track your preparation progress.

A one-year old child presents with the following lesion on the face. His mother has a history of bronchial asthma. What is the diagnosis? (Recent Question 2019)
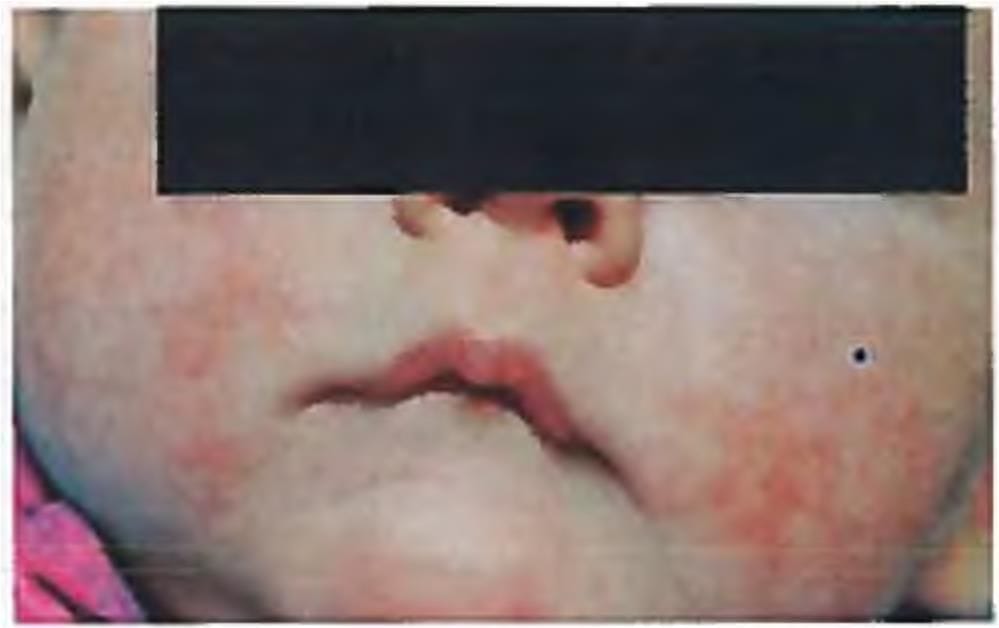
Detailed Solution: Question 1
A known asthmatic, presented to the emergency with severe exacerbation not relieved by Salbutamol. The patient was given corticosteroids and aminophylline. What is the rationale of giving corticosteroids? (AIIMS Nov 2017)
Detailed Solution: Question 2

Which of the following is not required in case a second puff is to be taken from an inhaler? (AIIMS Nov 2016)
Detailed Solution: Question 3
The following are indications for assisted ventilation in acute severe asthma EXCEPT? (APPG 2016)
Detailed Solution: Question 4
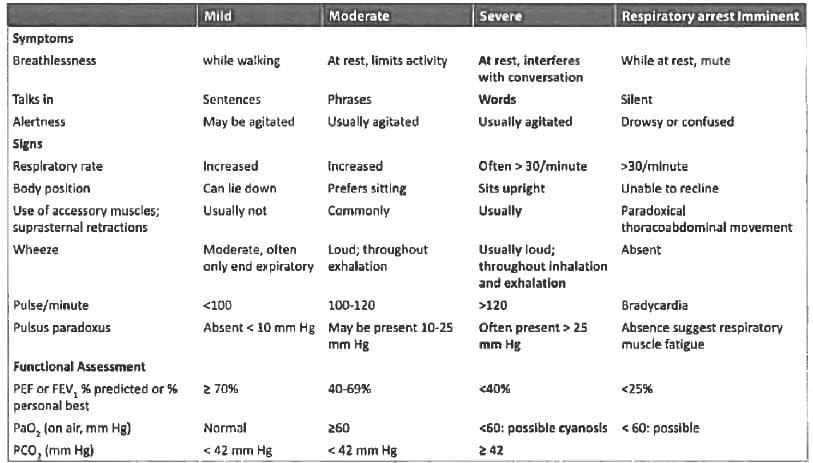
Which of the following features of severity are used in immediate assessment of acute severe asthma? (UPSC 2015)
- Pulse rate >110 per min
- Pulsus paradoxus
- Unable to speak in sentences
Select the correct answer using the code given below:
Detailed Solution: Question 5
Which one of the following is not recommended in immediate treatment of acute severe asthma? (UPSC 2015)
Detailed Solution: Question 6

The following are main diagnostic criteria for allergic bronchopulmonary aspergillosis except: (APPG 2015)
Detailed Solution: Question 7
Detailed Solution: Question 8
Thickening of pulmonary alveolar capillary membrane is seen in? (Bihar PG 2015)
Detailed Solution: Question 9
All are true about Aspirin sensitive asthma except? (Recent Question 2015-16)
Detailed Solution: Question 10
Detailed Solution: Question 11
Allergic broncho-pulmonary Aspergillosis presents with all except: (Recent Question 2015-16)
Detailed Solution: Question 12
Detailed Solution: Question 13
Which drugs are not used in severe persistent Asthma: (Recent Question 2015-16)
Detailed Solution: Question 14
Drug of choice for treatment of type 2 Brittle Asthma is? (Recent Question 2015-16)
Detailed Solution: Question 15
Child known case of bronchial asthma comes with respiratory rate 48/min, cannot speak 2 words, occasional wheeze and oxygen saturation of 95%. You give 3 doses of salbutamol nebulisation then he started to speak a sentence but saturation falls to 85%. Cause is? (AIIMS Nov 2014)
Detailed Solution: Question 16
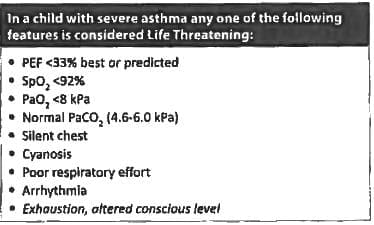
Consider the following statements:
Life threatening features of acute-severe asthma in children include?
- Altered sensorium
- Pulsus paradoxus
- Audible wheeze in both inspiration and expiration
- Oxygen saturation 92-95%
Which of these statements is/ are correct? (UPSC 2010)
Life threatening features of acute-severe asthma in children include?
Detailed Solution: Question 17
Aspirin sensitive asthma is associated with: (Recent Pattern 2014-15)
Detailed Solution: Question 18
A pediatric asthmatic patient presents with a severe attack of acute wheezing and breathlessness and drowsiness. Arterial blood gas analysis done after one hour of treatment with oxygen, nebulised salbutamol and intravenous corticosteroids show pH 7.26, PaO₂ of 60 mm Hg and PaCO₂ of 60 mm Hg. The next step in treatment should be: (AIPG 2011)
Detailed Solution: Question 19
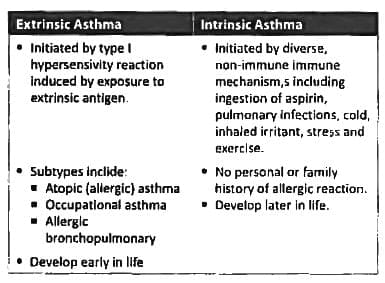
Consider the following statement:
Early onset extrinsic episodic asthma is characterized by:
- Family history of eczema or rhinitis
- Development of an early and late asthmatic reaction mediated by mast cells
- T lymphocytes that release cytokine like interleukin-4
Which of these statements are correct? (UPSC 2014)
Early onset extrinsic episodic asthma is characterized by:
Detailed Solution: Question 20
In bronchial asthma following pulmonary function abnormalities are present except: (Recent Pattern 2014-15)
Detailed Solution: Question 21
Consider the following statements:
The features of severe asthma include
- Central cyanosis
- Agitated behaviour
- Pulsus paradoxus
- Heart rate less than 60/minute
Which of these statements are correct? (UPSC 2013)
The features of severe asthma include
Detailed Solution: Question 22
Best for treatment of Exercise induced asthma? (Recent Pattern 2014-15)
Detailed Solution: Question 23
In severe bronchial asthma, true is: (Recent Pattern 2014-15)
Detailed Solution: Question 24
Which of the following is given in the maintenance of severe persistent asthma: (Recent Question 2015-16)
Detailed Solution: Question 25
All of the following are useful for treating acute bronchial asthma in children except: (Recent Pattern 2014-15)
Detailed Solution: Question 26
All of the following diseases are associated with peripheral blood eosinophilia except: (Recent Pattern 2014-15)
Detailed Solution: Question 27
The major diagnostic criteria for Allergic Bronchopulmonary Aspergillosis would include all the following except: (Recent Pattern 2014-15)
Detailed Solution: Question 28
Commonly used route of administration for Omalizumab in asthma is: (Recent Pattern 2014-15)
Detailed Solution: Question 29
Curschmann's Spirals in sputum is seen in: (Recent Pattern 2014-15)
Detailed Solution: Question 30
50 docs|64 tests |