Disorders of WBC & Leukemias - Free MCQ Practice Test with solutions, NEET
MCQ Practice Test & Solutions: Test: Disorders of WBC & Leukemias (39 Questions)
You can prepare effectively for NEET PG Medicine with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Disorders of WBC & Leukemias". These 39 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 20 minutes
- - Number of Questions: 39
Sign up on EduRev for free to attempt this test and track your preparation progress.


Detailed Solution: Question 1
All of the following are associated with HHV8 except? (AIIMS May 2018)
Detailed Solution: Question 2

A young girl with APML on day 3 of treatment develops tachypnea, weight gain and fever. CXR shows bilateral pulmonary infiltrates. What is the best management for the patient? (AIIMS May 2017)
Detailed Solution: Question 3
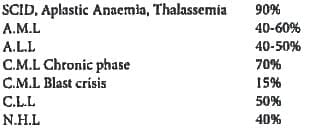
Which of the following has the least 5 year survival rate following allogenic bone marrow transplantation? (Recent Question 2016-17)
Detailed Solution: Question 4
Leukostasis is common with which of the following? (Recent Question 2016-17)
Detailed Solution: Question 5
Which organ is mainly affected in Leukostasis? (Recent Question 2016-17)
Detailed Solution: Question 6
Steroids are not indicated in the treatment of? (AIIMS Nov 2015)
Detailed Solution: Question 7
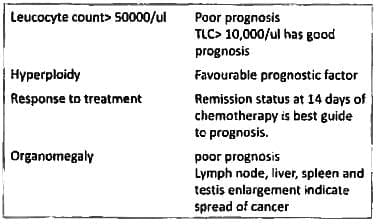
Most important best prognostic marker in ALL? (AIIMS Nov 2015)
Detailed Solution: Question 8
Which of the following statements is true regarding juvenile chronic myeloid leukemia? (UPSC 2015)
Detailed Solution: Question 9
Treatment of choice in hairy cell leukemia is? (Bihar PG 2015)
Detailed Solution: Question 10
2-year-old child with ALL, which of the following has the best prognosis? (Recent Question 2015-16)
Detailed Solution: Question 11
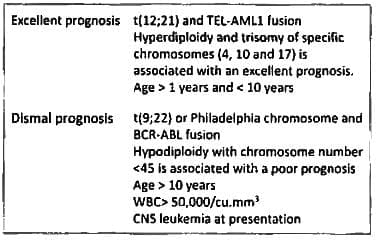
Philadelphia chromosome refers: (Recent Question 2015-16)
Detailed Solution: Question 12
Vitamin B, level in chronic myeloid leukemia is: (Recent Pattern 2014-15)
Detailed Solution: Question 13
Agranulocytosis is defined as neutrophil count less than: (Recent Pattern 2014-15)
Detailed Solution: Question 14
What is the most effective treatment for chronic myeloid leukaemia? (Recent Pattern 2014-15)
Detailed Solution: Question 15
What is the Neutrophil count for moderate neutropenia: (Recent Pattern 2014-15)
Radiation exposure does not cause: (Recent Pattern 2014-15)

Filgrastim is used for the treatment of: (Recent Pattern 2014-15)
Arsenic is used in treatment of: (Recent Pattern 2014-I5)
Most common type of acute myeloid leukemia: (Recent Pattern 2014-15)
Which one of the following laboratory tests differentiates leukamoid reaction from chronic myeloid leukemia? (Recent Pattern 2014-15)
DIC is seen in the following type of AML: (Recent Pattern 2014-15)
A 2-year-old child comes with ear discharge, seborrheic dermatitis, polyuria and hepato-splenomegaly. Which of the following is the most likely diagnosis:
80-year-old, asymptomatic man present with a Total leucocyte count of 1 lakh, with 80% lymphocytes and 20% PMCs. What is the most probable diagnosis? (Recent Pattern 2014-15)
According to FAB classification, promyelocytic blood picture belongs to which type of AML? (Recent Pattern 2014 15)
Cis-Retinoic acid syndrome is used for? (Recent Pattern 2014-15)
All of the following are features of juvenile CML except: (Recent Pattern 2014-15)
A peripheral smear with increased neutrophils, basophils, eosinophils, and platelets is highly suggestive of: (Recent Pattern 2014-15)

52 docs|64 tests |