Test: Anatomy - 5 - NEET PG MCQ
25 Questions MCQ Test - Test: Anatomy - 5

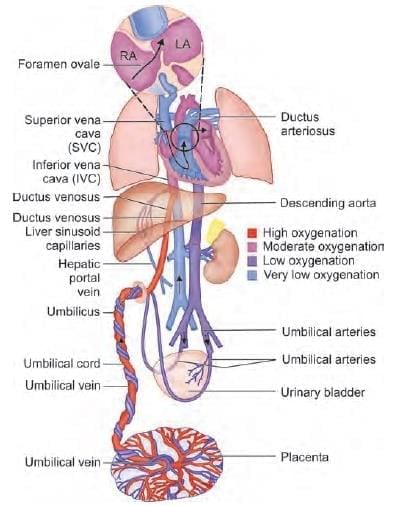
Highest oxygen concentration of fetal circulation is at which site? (NEET-PG 2020p)
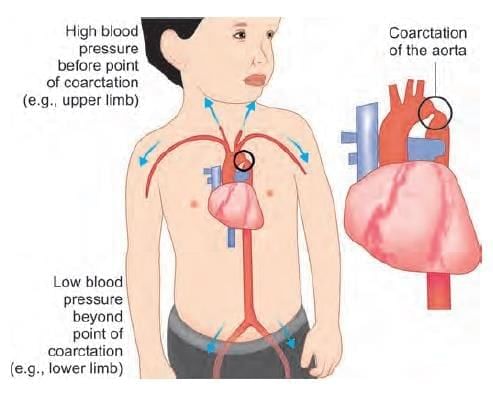
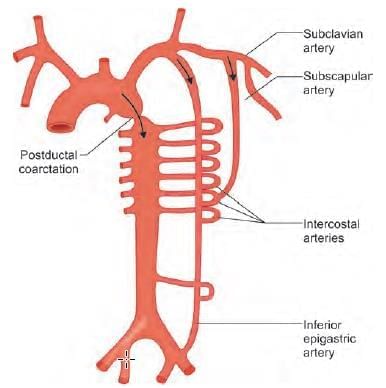
A 10-year-oId child presents with upper limb hypertension, and feeble lower limb pulses. Chest X-ray showed notching of ribs. What is the likely diagnosis? (NEET-PG 2021)

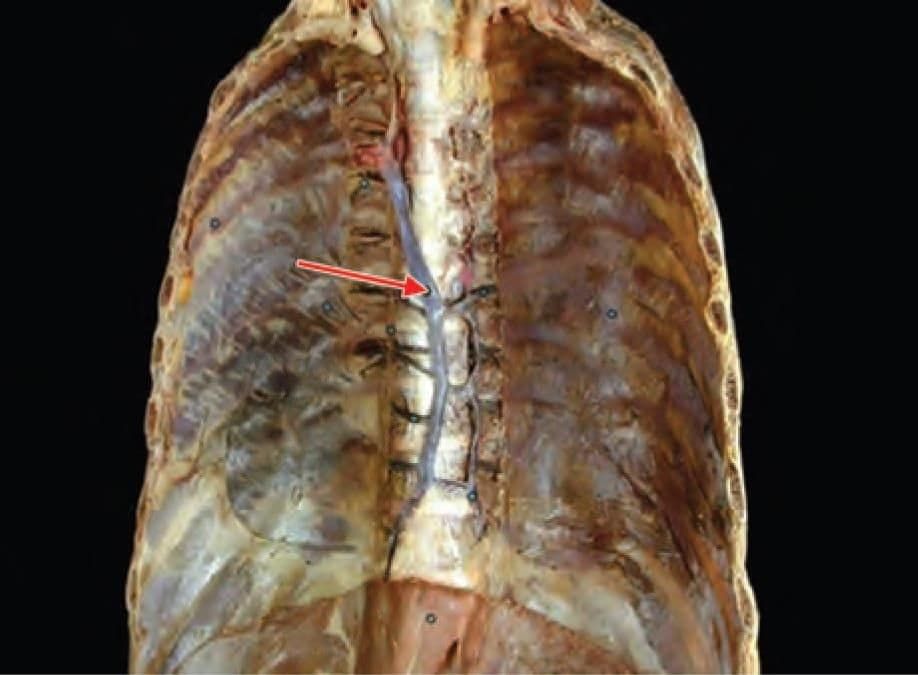
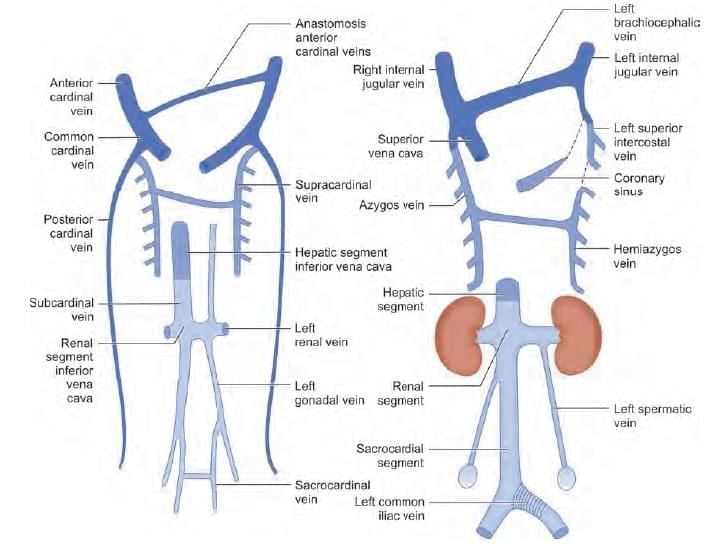
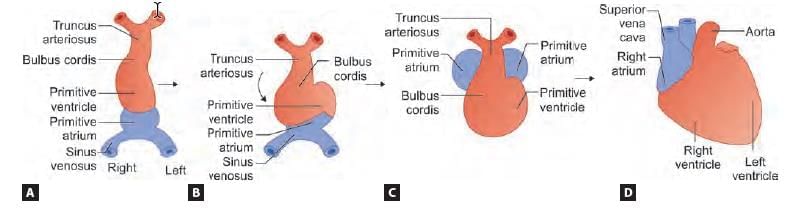
Identify the vein shown below and choose its embryological origin: (INI-CET Nov 2021)
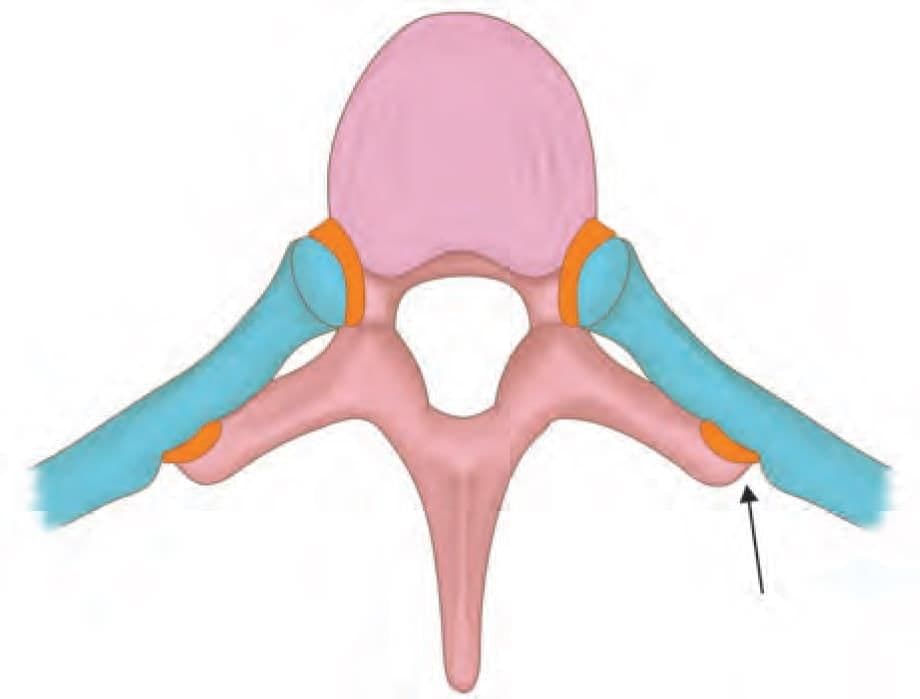
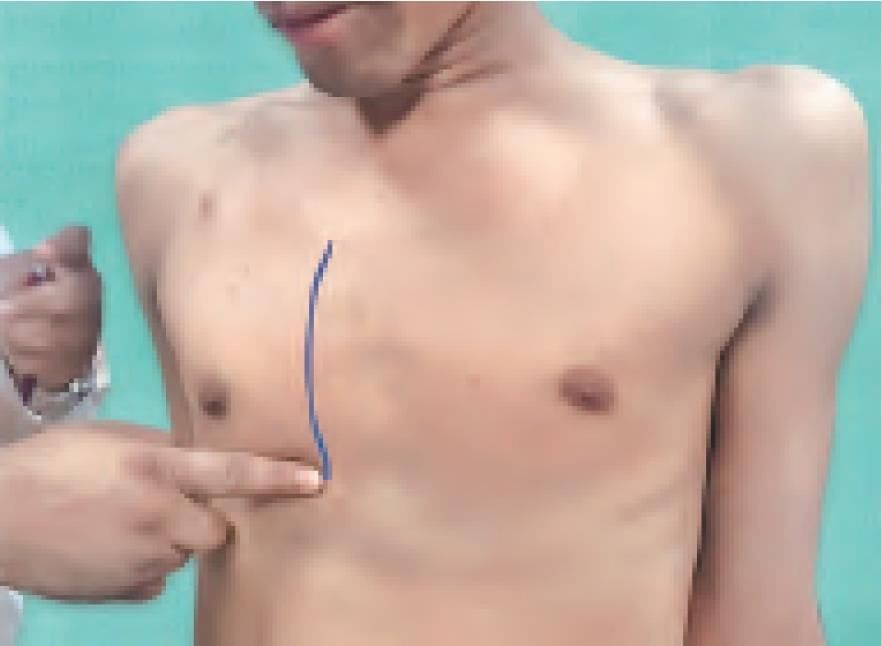
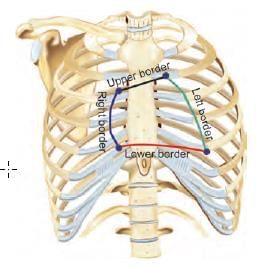
Surface marking of which of the following is demonstrated in the video. A convex line (towards right) is being drawn, starting at right 3rd costal cartilage to the right 6th costal cartilage, as shown in the diagram below: (AIIMS May 2019)
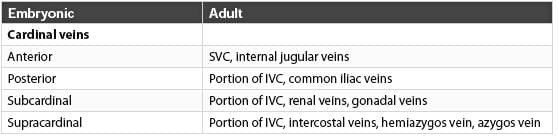
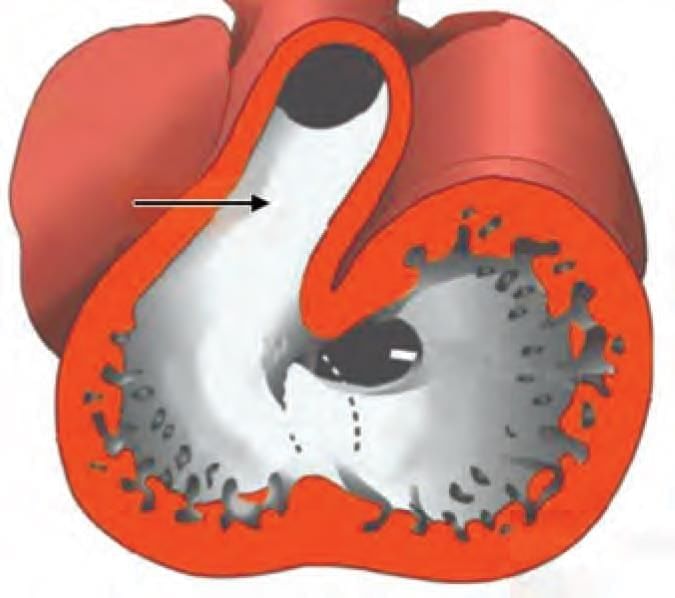
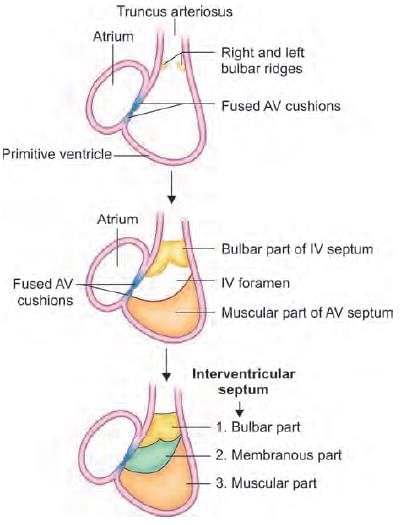
Which of the following structure develop from the arrow marked area? (AIIMS June 2020)
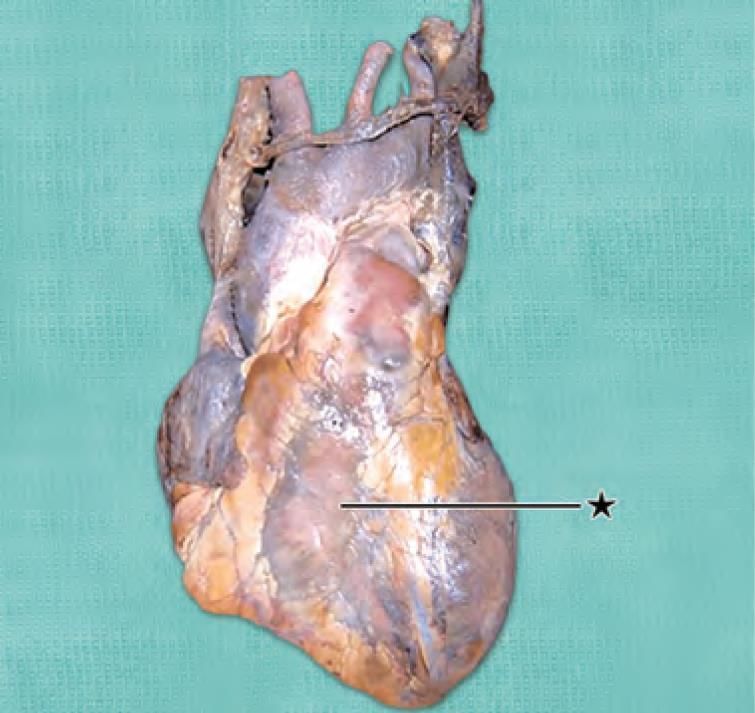
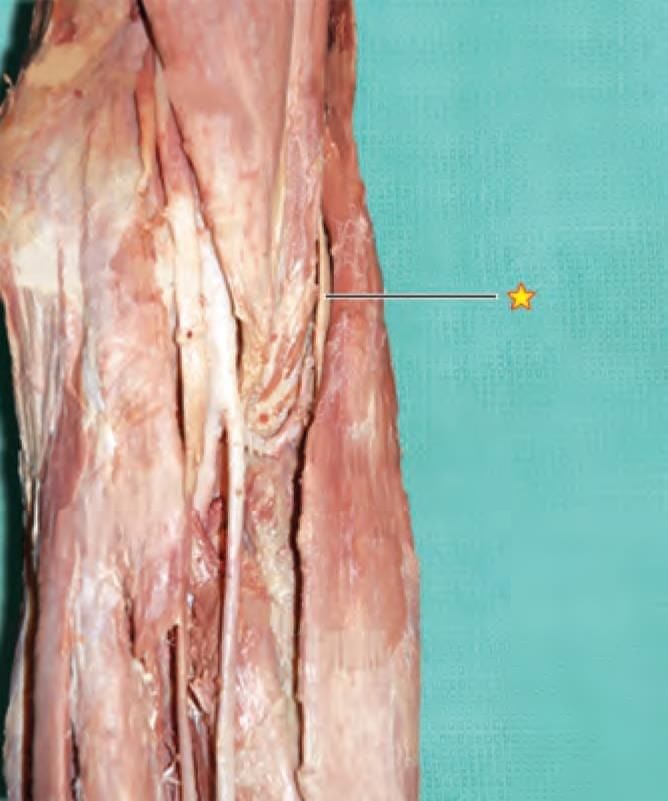
Marked structure is supplied by all the following arteries, except: (AIIMS Nov 2019)
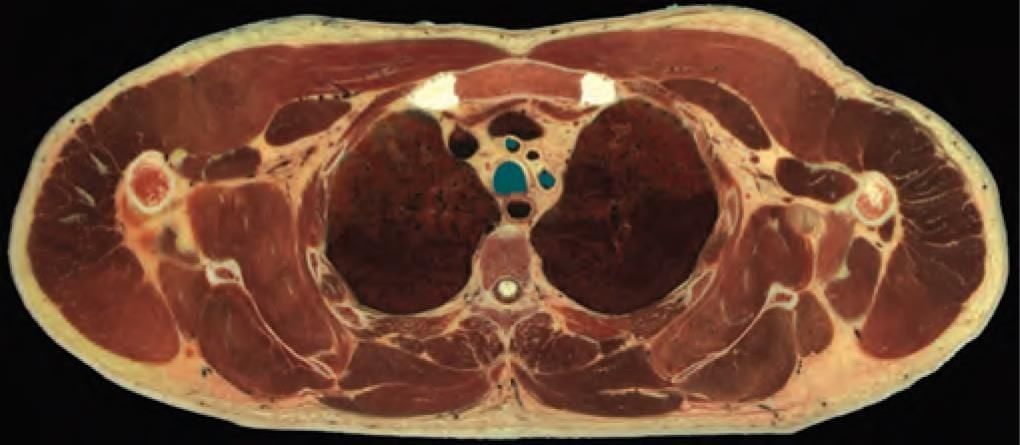
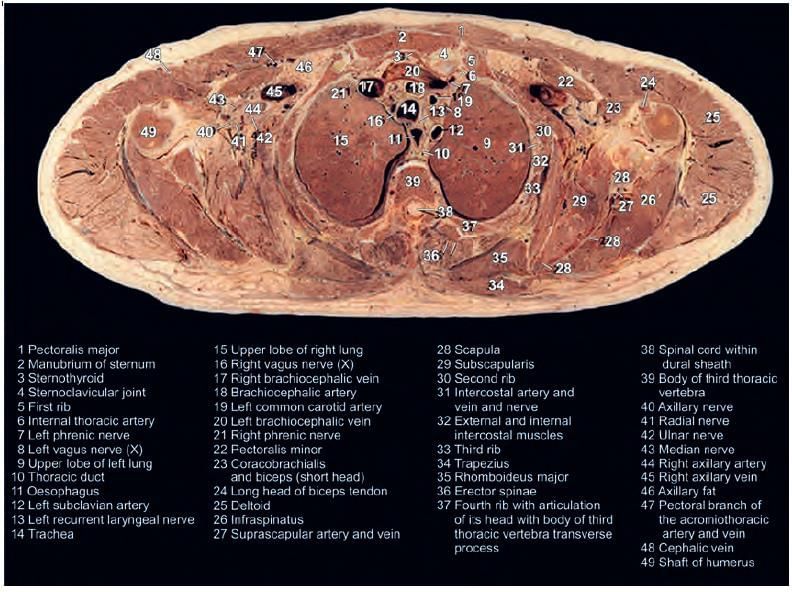
The present transverse section has been taken at which vertebra level? (INI-CET Nov 2020)
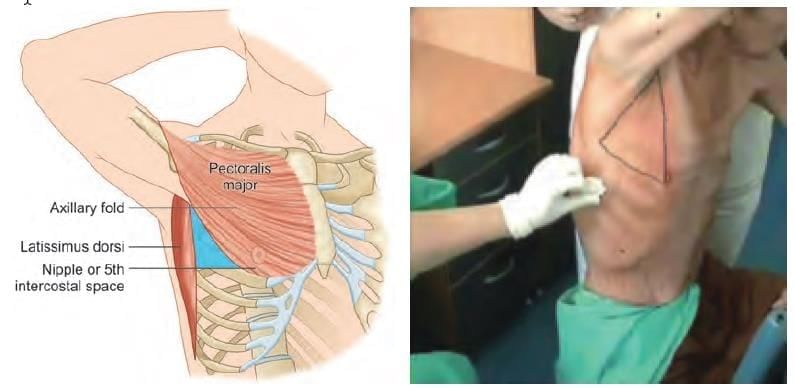
Which of the following is NOT a boundary for triangle of safety? (INI-CET Nov 2022)
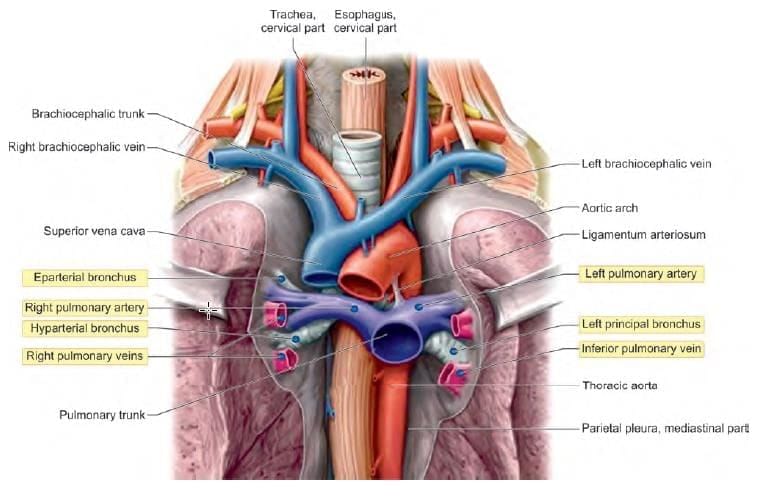
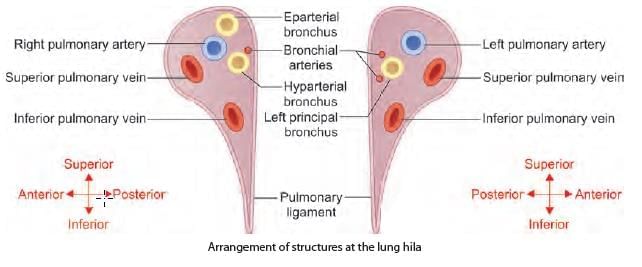
Arrangement of the structures in anterior to posterior relations at lung hilum: (INI-CET May 2022)
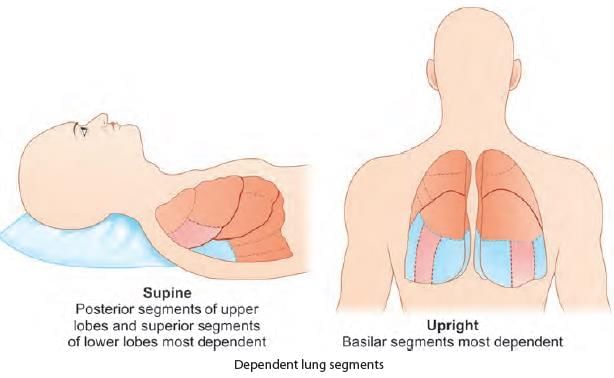
In a bed ridden patient, aspiration pneumonitis is most likely to involve which of the following bronchopulmonary segment? (INI-CET Nov 2022)
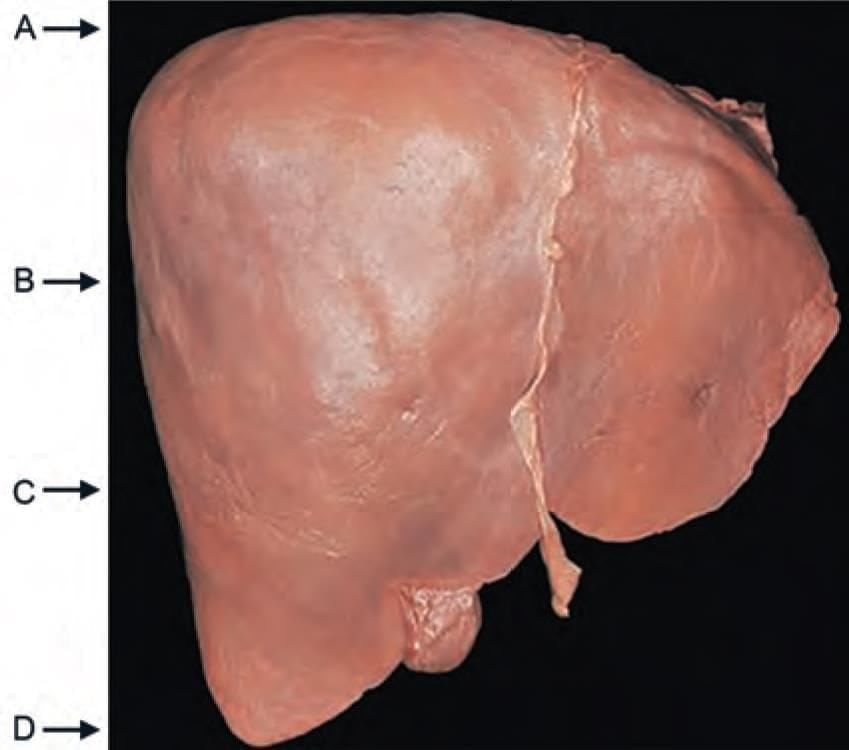
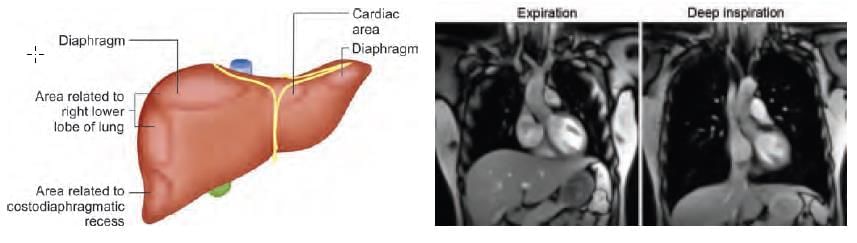
The lung (with visceral pleura) extend upto which level of liver during deep inspiration? (INI-CET Nov 2020)
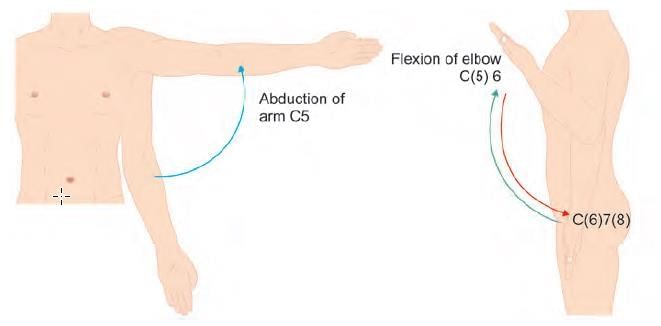
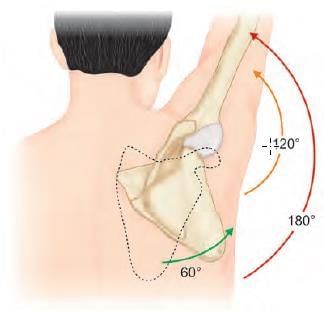
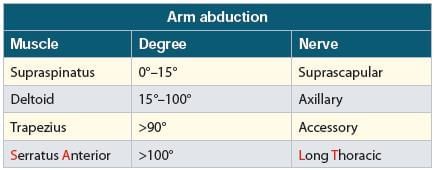
After cervical surgery shoulder abduction NOT possible due to lesioned: (INI-CET Nov 2020)
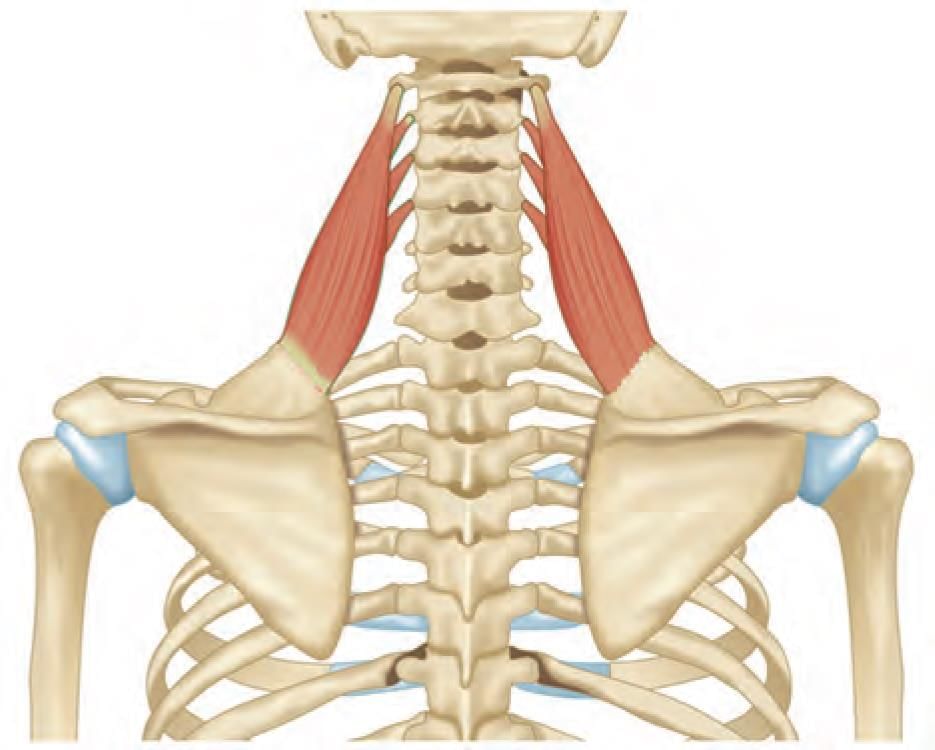
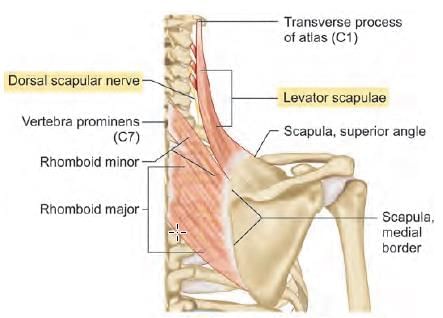
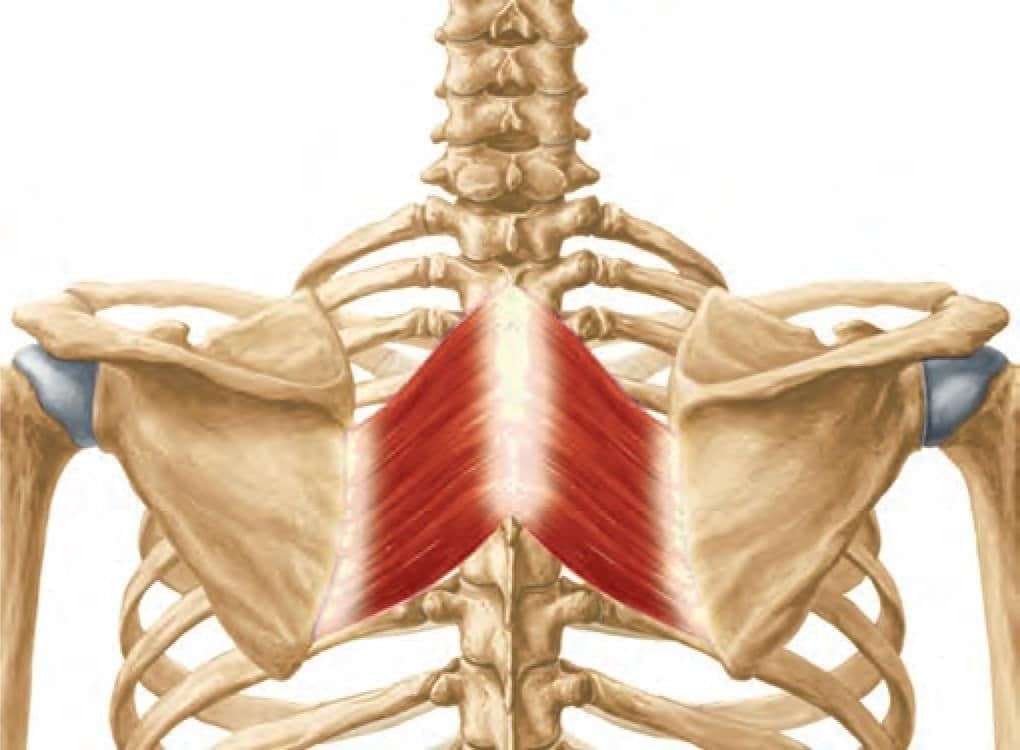
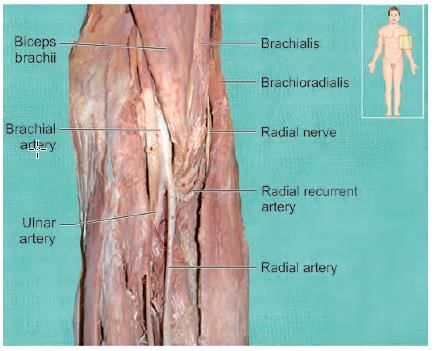
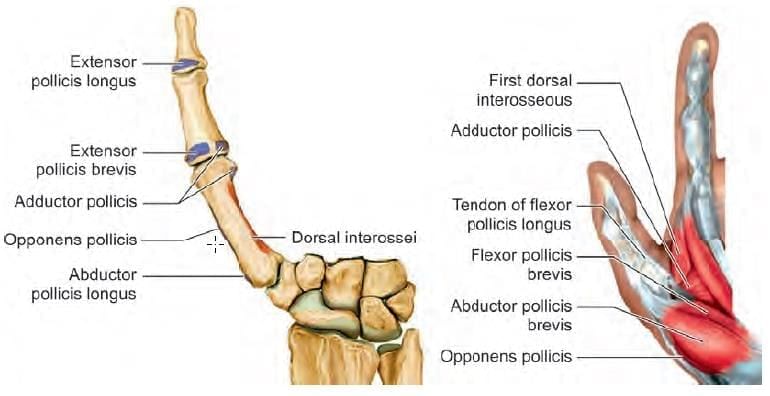
Nerve supply of the shown muscle is: (INI-CET Nov 2020) (NEET-PG 2020p)
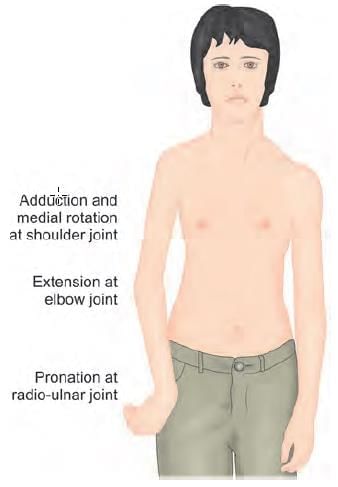
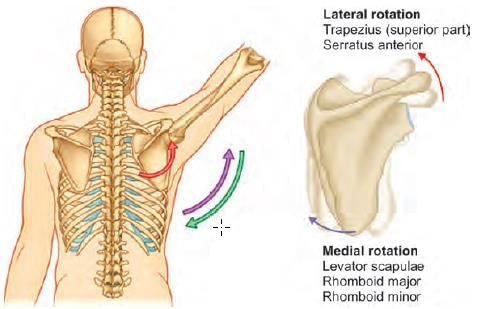
The mechanism of action of the marked muscle is: (INI-CET May 2023)
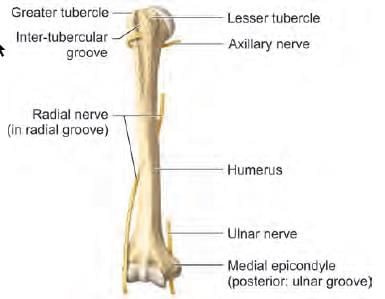
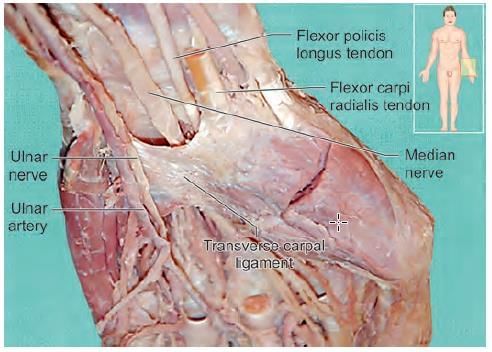
A patient has presented with inability to flex the distal interphalangeal joint of fourth and fifth fingers in right hand. Patient is also unable to hold a paper between fingers. At which of the following marked site, the nerve is most likely injured? (INI-CET July 2021, May 2022, 23)

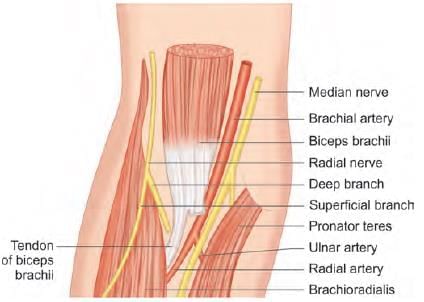
Arrangement of the structures in medial to lateral relations at cubital fossa: (INI-CET May 2022)
1. Biceps tendon
2. Brachial artery
3. Median nerve
4. Radial nerve

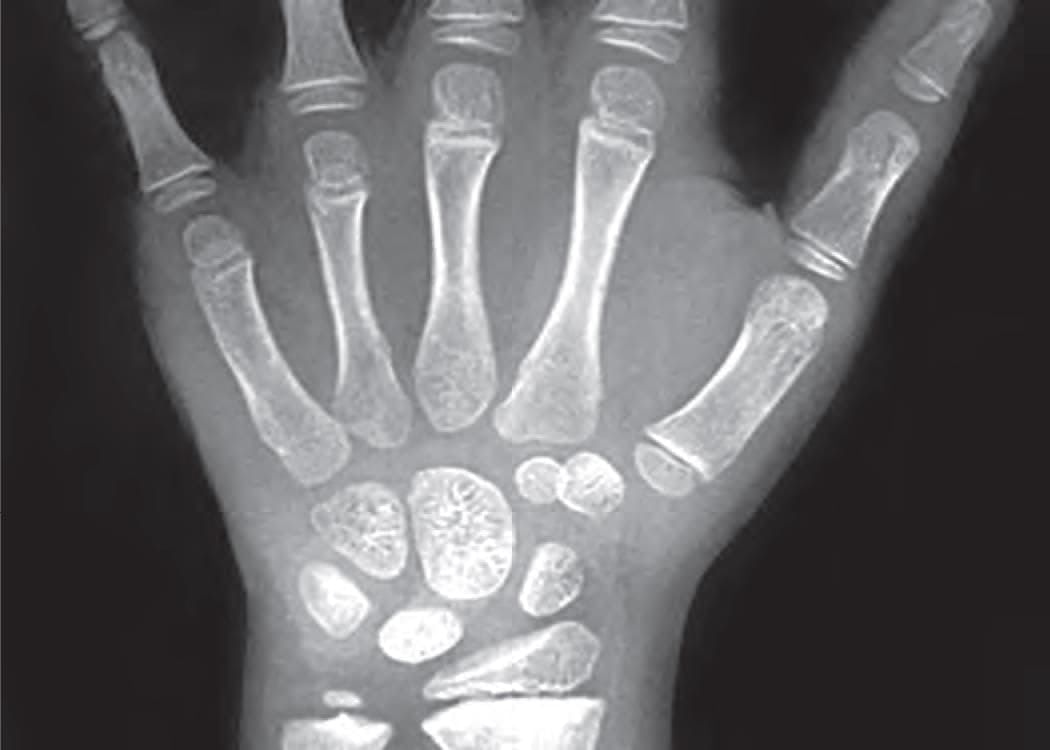
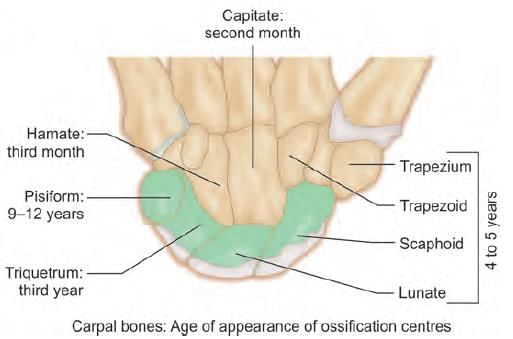
What is the most likely age of this child, a victim of rape being examined under POCSO act? (NEET-PG 2020p)

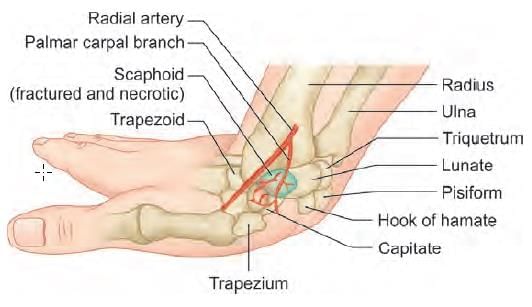
Assertion: In Scaphoid fracture, distal portion gets necrosed
Reason: Scaphoid has arterial supply in retrograde fashion (AIIMS May 2019)
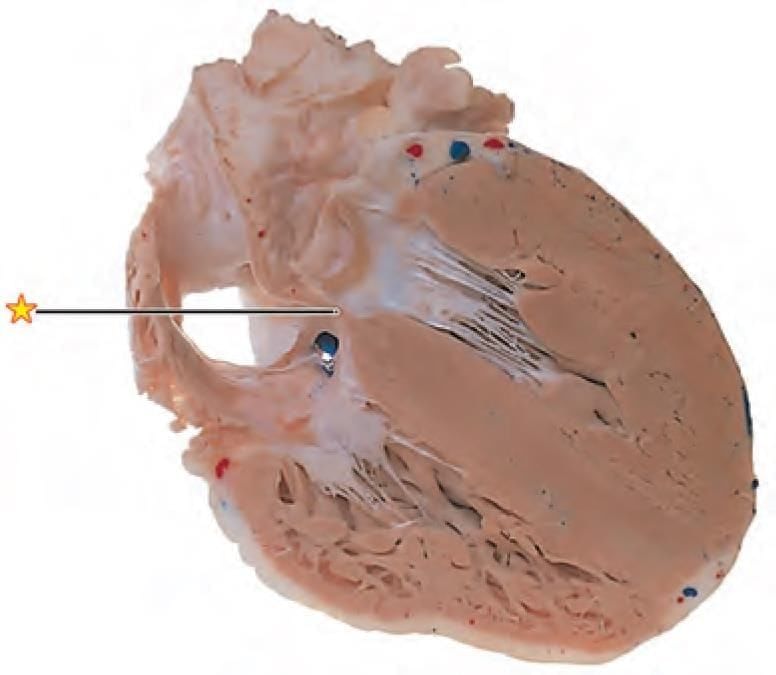
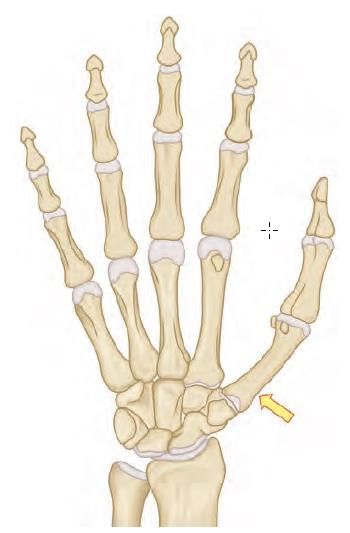
Name the muscle attached to the arrow marked area: (INI-CET Nov 2020)




Important Questions for Anatomy - 5
Anatomy - 5 MCQs with Answers
Online Tests for Anatomy - 5
|
© EduRev
|
Education Revolution
|



|









within 7 days!