Congenital Heart Disease - Free MCQ Practice Test with solutions, NEET
MCQ Practice Test & Solutions: Test: Congenital Heart Disease (25 Questions)
You can prepare effectively for NEET PG Medicine with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Congenital Heart Disease". These 25 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 25 minutes
- - Number of Questions: 25
Sign up on EduRev for free to attempt this test and track your preparation progress.

In coarctation of aorta, site of rib notching is? (Recent Question 2015-16)
Detailed Solution: Question 1
A neonate presents with anoxic spells and single S2. CXR shows all except:

Detailed Solution: Question 2

Lithium use in pregnancy leads to which effect on the baby? (AIMS Nov 2018)
Detailed Solution: Question 3
Epstein syndrome is characterised by presence of? (Recent Question 2019)
Detailed Solution: Question 4
Which of the following is compatible with tet spells in a 4 month old child with TOF? (AIIMS May 2016)
Detailed Solution: Question 5
Congenital heart disease associated with pre-excitation is? (UPSC 2015)
Detailed Solution: Question 6
When should a very large ventricular septal defect be operated? (UPSC 2015)
Detailed Solution: Question 7
Pulmonary blood flow increases in all except? (PGI Chandigarh May 2015)
Detailed Solution: Question 8
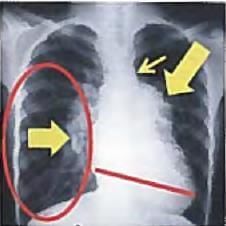
A 5-year old child with episodes of recurrent pneumonia was found to have a mid-diastolic murmur. CXR was performed. All are correct about the image shown except?

Detailed Solution: Question 9
Turner's syndrome is associated with? (Recent Pattern 2015-16)
Detailed Solution: Question 10
Most common cause of heart block in infants is? (Recent Pattern 2015-16)
Detailed Solution: Question 11
A Preterm baby with PDA will have all except: (AIMS Nov. 2012)
Detailed Solution: Question 12
All are causes of sudden death in infant except: (Recent Pattern 2014-15)
Detailed Solution: Question 13
Neonate with cyanosis, heart failure and systolic murmur is suffering from: (Recent Pattern 2014-15)
Detailed Solution: Question 14
Which of the following is not given it of cyanotic spell? (IS Nov. 2013)
Detailed Solution: Question 15
Ductus arteriosus complete closure occurs at how many weeks in a term baby? (Recent Pattern 2014-15)
Detailed Solution: Question 16
Alprostadil is contraindicated In: (Recent Pattern 2014-15)
Detailed Solution: Question 17
Partial anomalous pulmonary venous connection is associated with which of the following defects? (Recent Pattern 2014-15)
Detailed Solution: Question 18
Which of the following conditions causes both superior as well as inferior notching of the ribs? (Recent Pattern 2014 15)
Detailed Solution: Question 19
Reversal of shunt is not possible in natural history of: (AIIMS Nov. 2012)
Detailed Solution: Question 20
A preterm baby with Patent Ductus Arteriosus. All are true except: (AIIMS May 2013)
Detailed Solution: Question 21
Extremely bad prognosis is seen in which heart disease in pregnancy? (Recent Pattern 2014-15)
Detailed Solution: Question 22
A 6-hour old child with cyanosis. On examination, S2 is loud and single. CXR was done. All arc true about this condition except?


Detailed Solution: Question 23
All of the following are true about ASD except: (AI 2001)
Detailed Solution: Question 24
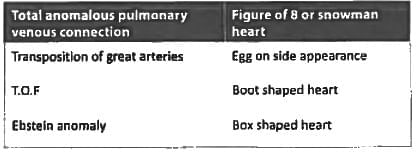
Snow man appearance or figure of 8 appearance is seen in? (Recent Question 2015-16)
Detailed Solution: Question 25
52 docs|64 tests |