Test: Disorders of Adrenal Cortex - NEET PG MCQ
30 Questions MCQ Test - Test: Disorders of Adrenal Cortex

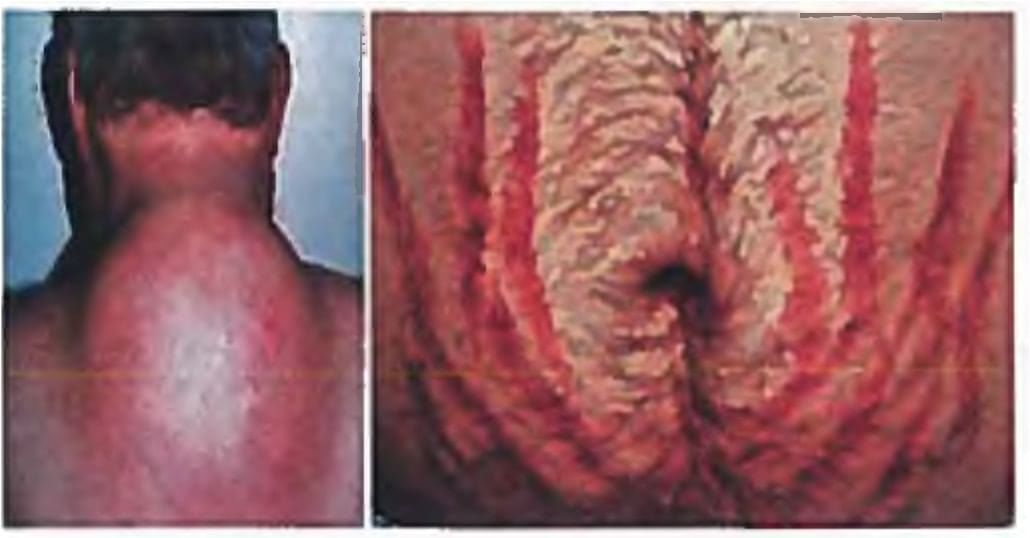
All are true about the condition shown except? (Recent Pattern Questions)
All of the following investigations are needed for the following case except? (Recent Questions 2016-17)



All are features of glucocorticoid deficiency except? (AIIMS Nov 2015)
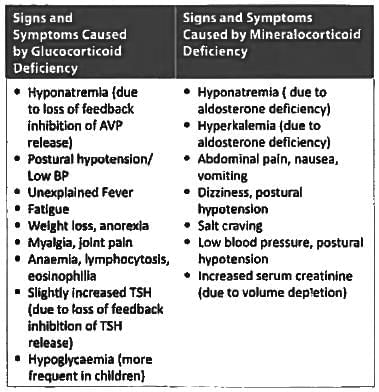
All are seen in Addison's disease EXCEPT? (Recent Questions 2015-16)
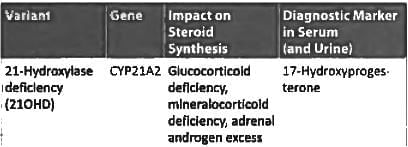
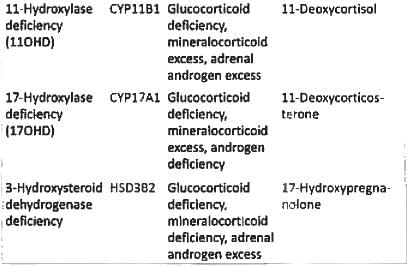
Congenital adrenal hyperplasia due to 11 beta hydroxylase deficiency presents with all EXCEPT? (Recent Questions 2015-16)
40 year Male presents with primary infertility. Testis is present with azoospermia and absent vas deferens (AIIMS Nov 14)
Obesity is seen in all except: (Recent Pattern 2014-15)
Primary hyperaldosteronism can be diagnosed by all of the following criteria except: (Recent Pattern 2014-15)
Cushing syndrome is commonly caused by: (Recent Pattern 2014-15)
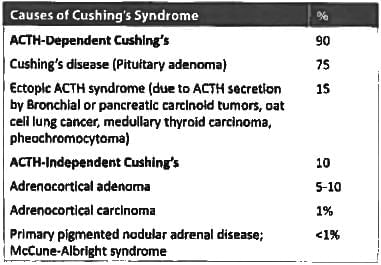
Most common cause of Cushing's syndrome is: (Recent Pattern 2014-15)
Not seen in Cushing's syndrome: (Recent Pattern 2014-15)
A 28-year-old lady has put on weight (10 kg over a period of 3 years) and has oligomenorrhoea followed by amenorrhoea for 8 months. The blood pressure is 160/100 mm of Hg. Which of the following is the most appropriate investigation? (AIPG 2011)

A patient presents with hemoptysis and cushingoid features with a lack of dexamethasone suppression, the likely reason could be: (Recent Pattern 2014-15)
Conn's syndrome is characterized by all except:
Best for management of hypoglycemia in a girl child with Congenital adrenal hyperplasia ? (Recent Pattern 2014-15)
Congenital 17-hydroxylase deficiency leads to hypertension due to accumulation of? (Recent Pattern 2014-15)
Decreased plasma renin activity is seen in: (Recent Pattern 2014-15)
Incorrect about Addison's disease is? (Recent Pattern 2014-15)
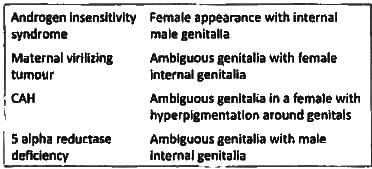
A child presents with ambiguous genitalia without hyperpigmentation and normal blood pressure, 2.5 cm phallus with no opening at its tip, labia developed. Gonads are not seen in inguinal region and Mullerian structures are present on USG. The most probable diagnosis is: (Recent Pattern 2014-15)
In Conn's syndrome, all the following are seen, except: (Recent Pattern 2014-15)
Hypertension with hypokalemia is seen in following except: (Recent Pattern 2014-15)
Important Questions for Disorders of Adrenal Cortex
Disorders of Adrenal Cortex MCQs with Answers
Online Tests for Disorders of Adrenal Cortex
|
© EduRev
|
Education Revolution
|



|








