Test: Miscellaneous - NEET PG MCQ
30 Questions MCQ Test - Test: Miscellaneous

In a patient with autonomic dysreflexia after a spinal cord injury, supine BP of the patient is 200/100 mm Hg with Heart rate of 58/min. Which of the following is required for initial management of these patients? (Recent Question 2019)

Which of the following indicates modified shock index? (AIIMS Nov 2017)

A 25-year-old patient with abdominal trauma presents with Hypovolemic shock, and is unresponsive to crystalloids. What is the next step? (Recent Question 2016-17)
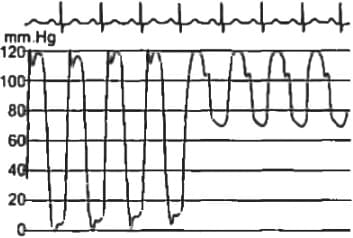
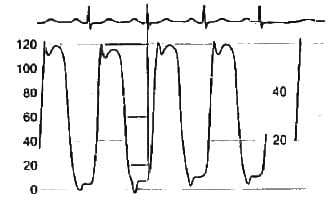
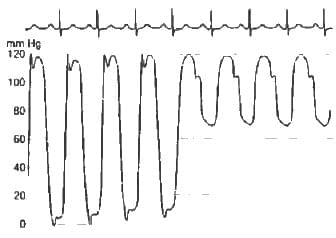
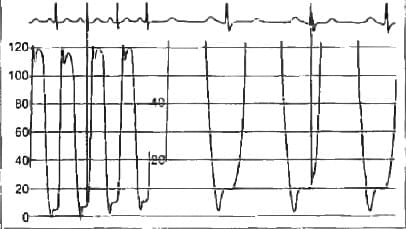
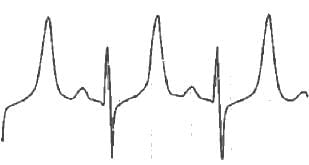
This picture depicts the pressure recordings from _____ (APPG 2016)
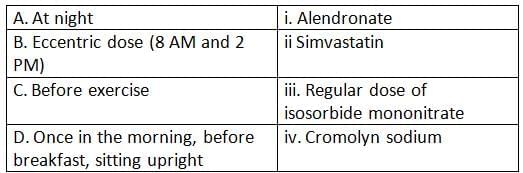
Match the following drugs with their timing of administration (APPG 2016)
Clinical markers in the revised Cardiac Risk Index (in preop evaluation) include the following EXCEPT. (APPG 2016)
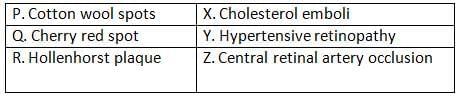
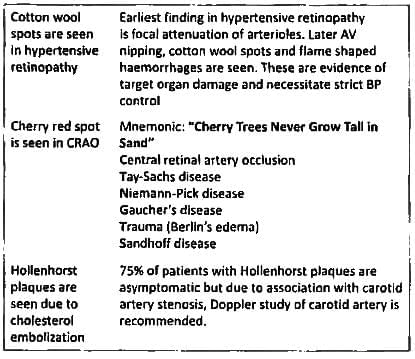
Match the following fundus findings and choose the best combination (APPG 2016)
Atrial Myxoma is associated with the following except? (UPSC 2015)
All of the following diseases affect the heart muscle except? (JIPMER May 2015)
A young woman present to the emergency departments with central cyanosis because her friends told her she looks bluish she is asymptomatic what could be the cause of bluish discolorations of tongue? (JIPMER Nov 2014)
Initial ECG change in Hyperkalemia is? (Recent Question 2015-16)
A Patient presented with deficiency of thiamine. What could be possible outcome: (Recent Question 2015-16)
A 1-year-old male child is having a Heart Rate 40/min, BP 90/60. His serum Potassium = 6.5. What is the next best management? (Recent Question 2015-16)
Patient with ICD collapses, which ICD imaging modality is best suited for this patient? (AIIMS Nov. 2012)
According to AHA 2010, drug not used in CPR is? (AIMS Nov. 2013)
Beyond which critical value Shock Index [Heart rate/BP] in pregnancy is considered abnormal? (AIIMS Nov. 2012)
Important Questions for Miscellaneous
Miscellaneous MCQs with Answers
Online Tests for Miscellaneous
|
© EduRev
|
Education Revolution
|



|









within 7 days!