Test: Raised ICP- 1 - NEET PG MCQ
30 Questions MCQ Test - Test: Raised ICP- 1

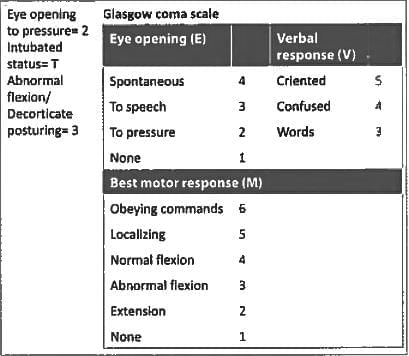
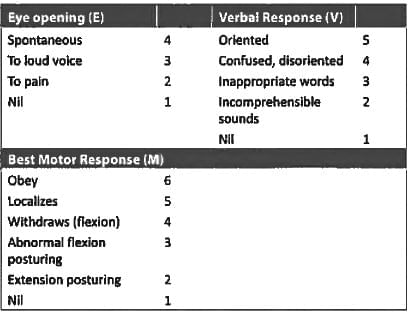
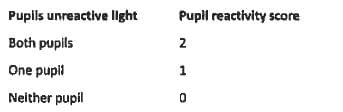
An intubated patient exhibits eye opening to pressure and abnormal flexion. What is the GCS score? (AIIMS May 2018)
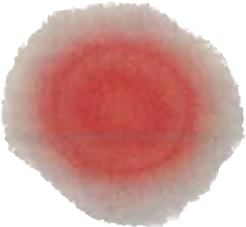
In a patient of head injury, the following sign is noted on his handkerchief. Which is the next test to confirm the diagnosis? (Recent Question 2019)

Patient had a RTA and was put on mechanical ventilation. He is opening his eyes on verbal command. He moves all his limbs spontaneously. What will be his GCS score? (AIIMS Nov 2018)
Calculate the GCS of a patient with spontaneous eye opening, who moves away his limb on painful stimulus and speaks inappropriate words? (AIIMS Nov 2017)
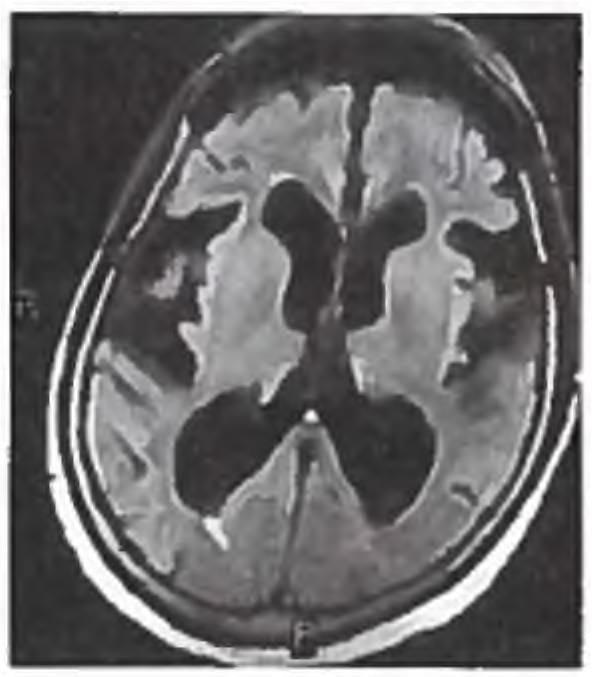
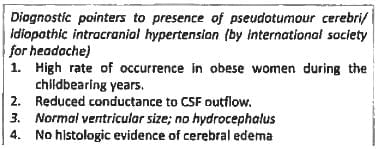
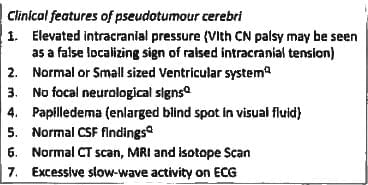
A lady had a normal vaginal delivery and was discharged. On 3rd day she came back with fever, tachycardia and seizures. Fundus examination shows papilledema with no focal deficits. What is the diagnosis? (AIMS May 2017)
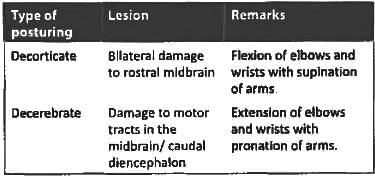
A 30 year old female was admitted to casualty with a history of head trauma. On examination she is lying with both legs in extended posture. She opens her eyes to pain, moans and localises pain on left hand. Calculate her GCS? (AIIMS May 2017)
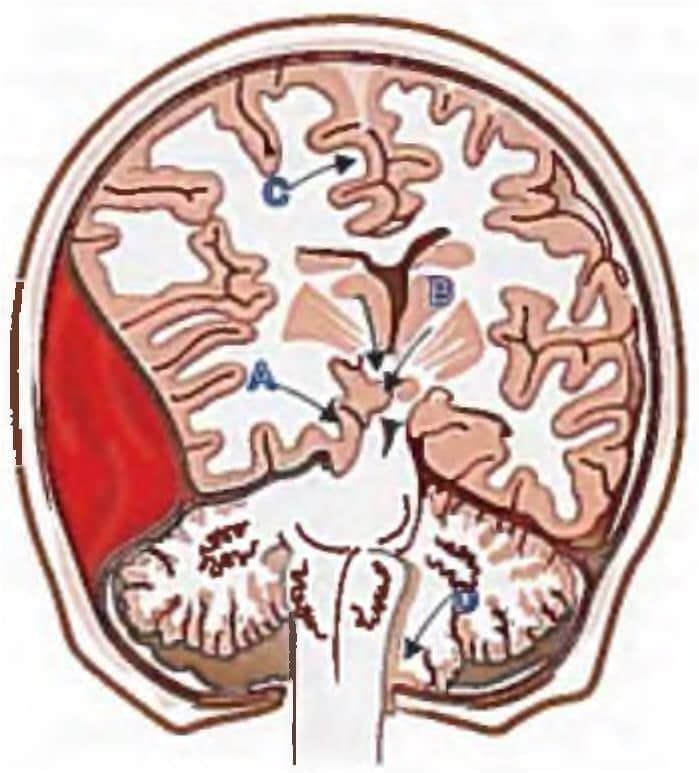
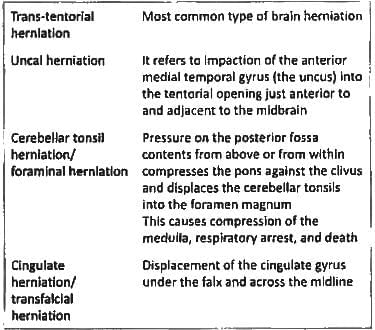
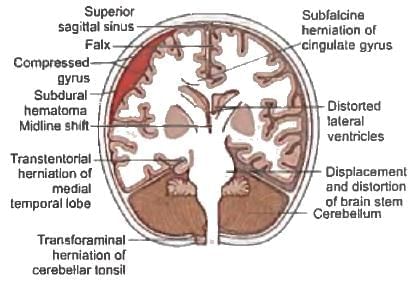
Foraminal brain herniation leads to? (Recent Pattern Questions)
Horizontal displacement of pineal calcification > ___ mm is associated with coma. (Recent Question 2016-17)
All are used for management in head injury patient except? (Recent Question 2016-17)
Most common form of brain herniation is? (Recent Question 2016-17)
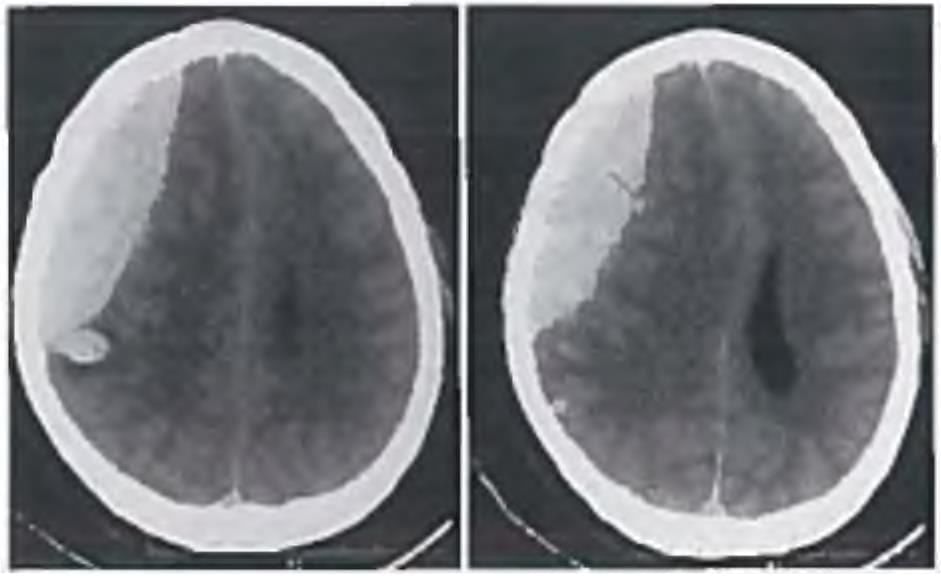
This is the plain CT scan of a male who sustained an injury with a baseball bat. Which of the following statements are TRUE regarding this condition? (AP PG 2016)
P. Middle meningeal artery is the vessel commonly injured
Q. Usually occurs several weeks after a trivial injury, often forgotten
R. Lucid interval is classical but seen only in 1/5th to 1/3rd patients
S. May be associated with a Hutchinson pupil
All are seen in Benign Intracranial Hypertension except? (AIIMS Nov 2015)
In Glasgow coma scale maximum and minimum scores are? (AIMS Nov 2015)

Commonly used shunt in hydrocephalus management? (AIIMS May 2015)
A 10 year old child 'blanks out' in class (e.g. stops talking midsentence and then continues as if nothing had happened). During spells there is slight quivering of lips. What is the most probable diagnosis? (UPSC 2015)
Patient has space occupying lesion in temporal and occipital lobe. What will occur? (JIPMER Nov 2015)
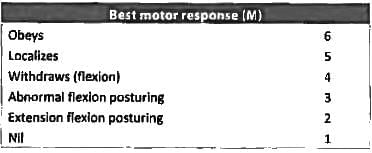
Glasgow coma scale motor 4 represents? (Recent Question 2015-16)
Important Questions for Raised ICP- 1
Raised ICP- 1 MCQs with Answers
Online Tests for Raised ICP- 1
|
© EduRev
|
Education Revolution
|



|








