Rheumatoid Arthritis - Free MCQ Practice Test with solutions, NEET PG
MCQ Practice Test & Solutions: Test: Rheumatoid Arthritis (30 Questions)
You can prepare effectively for NEET PG Topic Wise MCQs for NEET PG with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Rheumatoid Arthritis". These 30 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 30 minutes
- - Number of Questions: 30
Sign up on EduRev for free to attempt this test and track your preparation progress.

Which of the following drugs is not used in management of Rheumatoid arthritis? (AIIMS May 2018)
Detailed Solution: Question 1
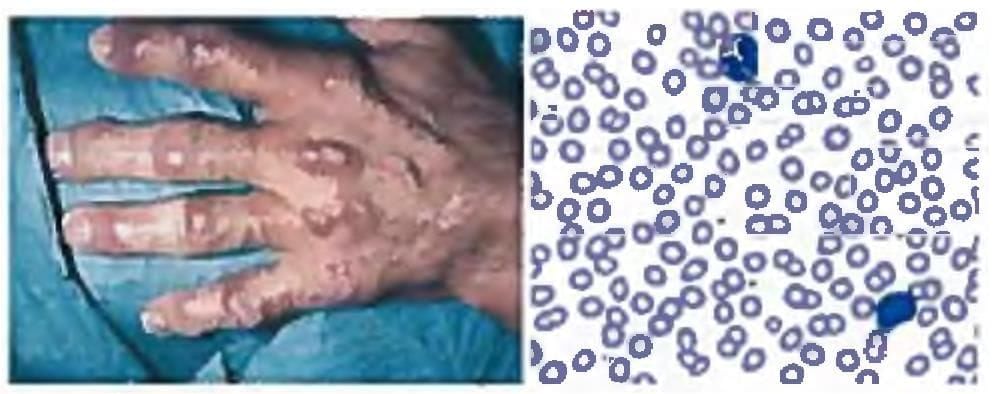
A woman presents with pain, swelling and redness of knee joint and hand. There were associated complaints of morning stiffness but the swelling spared the DIP joints. The image of the patient's hand is shown. What is the most likely diagnosis? (AIIMS May 2018)

Detailed Solution: Question 2

Which is not included in Polymyalgia rheumatic criteria (Healey criteria)? (JIPMER May 2018)
Detailed Solution: Question 3
A 55-year-old female on methotrexate presents with continuous pain and swelling of bilateral hand joints. What is the best treatment plan for this patient? (Recent Pattern Jan 2019)

Detailed Solution: Question 4
Which is the most common cause of death in rheumatoid arthritis? (Recent Question 2016-17)
Detailed Solution: Question 5
Which is the most common valvular lesion seen in rheumatoid arthritis? (Recent Question 2016-17)
Detailed Solution: Question 6
The most specific antibody for Rheumatoid arthritis is? (AP PG 2016)
Detailed Solution: Question 7
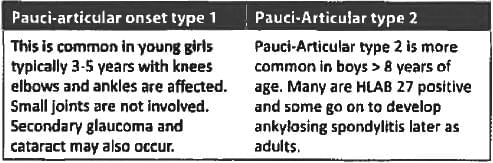
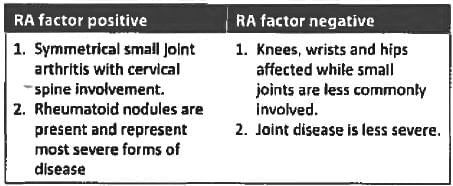
Consider the following statements about poly-articular juvenile rheumatoid arthritis?
a. It is more common in girls
b. Five or more joints are affected within the first six months of onset
c. Uveitis occurs in 95% patients
d. Rheumatoid factor may be negative
Which of the statements given above are true? (UPSC 2015)
a. It is more common in girls
b. Five or more joints are affected within the first six months of onset
c. Uveitis occurs in 95% patients
d. Rheumatoid factor may be negative
Which of the statements given above are true? (UPSC 2015)
Detailed Solution: Question 8
The most common type of juvenile rheumatoid arthritis is: (UPSC 2015)
Detailed Solution: Question 9
Which part of the spine is most commonly affected in Rheumatoid arthritis? (Bihar PG 2015)
Detailed Solution: Question 10
All are seen in Rheumatoid arthritis EXCEPT: (Recent Pattern 2015-16)
Detailed Solution: Question 11
In long standing rheumatoid arthritis which will be seen? (Recent Pattern 2015-16)
Detailed Solution: Question 12
Clinical manifestation of Felty’s syndrome are all except: (Recent Pattern 2014-15)
Detailed Solution: Question 13
Rheumatoid arthritis is seen with? (Recent Pattern 2015-16)
Detailed Solution: Question 14
Rheumatoid arthritis commonly affects the: (Recent Pattern 2014-15)
Detailed Solution: Question 15
Gold is used for management of? (Recent Pattern 2015-16)
Detailed Solution: Question 16
Caplan’s syndrome is seen with? (Recent Pattern 2014-15)
Detailed Solution: Question 17
Detailed Solution: Question 18
A patient of rheumatoid arthritis develops sudden onset Quadriparesis increased muscle tone of limbs with exaggerated tendon jerks and worsening of gait. The investigation to be done? (Recent Pattern 2014-15)
Detailed Solution: Question 19
Polyarticular onset JRA involves more than how many joints: (Recent Pattern 2014-15)
Detailed Solution: Question 20
Which is the most common site of subcutaneous nodules in rheumatoid arthritis? (Recent Pattern 2014-15)
Detailed Solution: Question 21
C V junction abnormalities are seen in all of the following except: (Recent Pattern 2014-15)
Detailed Solution: Question 22
Not seen in rheumatoid arthritis is: (Recent Pattern 2014-15)
Detailed Solution: Question 23
In rheumatoid arthritis the characteristic joint involvement is: (Recent Pattern 2014-15)
Detailed Solution: Question 24
All may be true about Rheumatoid Arthritis except: (Recent Pattern 2014-15)
Detailed Solution: Question 25
The most common cardiac involvement in rheumatoid arthritis: (Recent Pattern 2014-I5)
Detailed Solution: Question 26
Hemophilia with Rheumatoid arthritis, analgesic of choice is: (PGI Dec 98)
Detailed Solution: Question 27
Which of the following is the most specific test for rheumatoid arthritis? (Recent Pattern 2014-15)
Detailed Solution: Question 28
Detailed Solution: Question 29
Which type of anemia seen in Rheumatoid arthritis? (Recent Pattern 2014-15)
Detailed Solution: Question 30