Spirometry, DLco, Alveolar-Arteriolar Gradient & Types of Respiratory Failure-
MCQ Practice Test & Solutions: Test: Spirometry, DLco, Alveolar-Arteriolar Gradient & Types of Respiratory Failure- 2 (15 Questions)
You can prepare effectively for NEET PG Medicine with this dedicated MCQ Practice Test (available with solutions) on the important topic of "Test: Spirometry, DLco, Alveolar-Arteriolar Gradient & Types of Respiratory Failure- 2". These 15 questions have been designed by the experts with the latest curriculum of NEET PG 2026, to help you master the concept.
Test Highlights:
- - Format: Multiple Choice Questions (MCQ)
- - Duration: 15 minutes
- - Number of Questions: 15
Sign up on EduRev for free to attempt this test and track your preparation progress.

A 17-year-old boy presents with complaints of difficulty in breathing. There was venous congestion of face and neck. A clinical diagnosis of SVC syndrome was made. The X-ray showed mediastinal widening. What is the next step?
Detailed Solution: Question 1
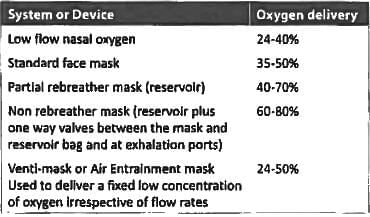
Maximum oxygen concentration can be delivered by? (AIIMS Nov 2017)
Detailed Solution: Question 2

Which of the following is not an etiology for peripheral cyanosis? (Recent Pattern Questions)
Detailed Solution: Question 3
Crescendo-decrescendo breathing pattern is seen in? (Recent Pattern Questions)
Detailed Solution: Question 4
A 55 year old female with morbid obesity presents to the ER with increased breathlessness, cough and orthopnea for 2 days. She has pulse rate of 96/minute, BP = 136/90 mmHg, RR = 30/min and spO₂ = 76%. ABG report shows pO₂ = 76 mm Hg, PCO₂ = 24 mmHg and pH = 7.28, The next step is? (AIIMS May 2016)
Detailed Solution: Question 5
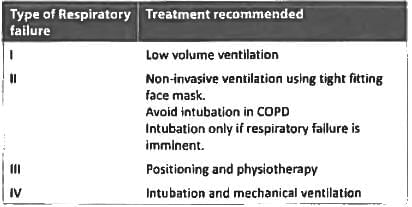
Which is the best treatment of type 4 Respiratory failure? (Recent Question 2016-17)
Detailed Solution: Question 6
Which of the following is the common cause of respiratory failure Type 2? (Recent Question 2015-16)
Detailed Solution: Question 7
Type II respiratory failure is seen in:
Detailed Solution: Question 8
Type 3 respiratory failure occurs due to: (Recent Pattern 2014-15)
Detailed Solution: Question 9
In type II respiratory failure there is: (Recent Pattern 2014-15)
Detailed Solution: Question 10
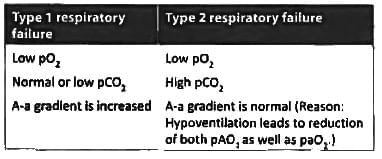
All of the following are true about type I respiratory failure except: (Recent Pattern 2014-15)
Detailed Solution: Question 11
Alveolar hypoventilation is observed in: (Recent Pattern 2014-15)
Detailed Solution: Question 12
Paradoxical breathing is characteristic of: (Recent Pattern 2014-15)
Detailed Solution: Question 13
Prolonged hyperventilation may lead to all except: (Recent Pattern 2014-15)
Detailed Solution: Question 14
Acute respiratory failure does not occur with: (Recent Pattern 2014-15)
Detailed Solution: Question 15
56 docs|64 tests |