NEET PG Exam > NEET PG Tests > Test: WPW and Brugada Syndrome & JVP - NEET PG MCQ
Test: WPW and Brugada Syndrome & JVP - NEET PG MCQ
Test Description
10 Questions MCQ Test - Test: WPW and Brugada Syndrome & JVP
Test: WPW and Brugada Syndrome & JVP for NEET PG 2025 is part of NEET PG preparation. The Test: WPW and Brugada Syndrome & JVP questions and answers have been prepared
according to the NEET PG exam syllabus.The Test: WPW and Brugada Syndrome & JVP MCQs are made for NEET PG 2025 Exam.
Find important definitions, questions, notes, meanings, examples, exercises, MCQs and online tests for Test: WPW and Brugada Syndrome & JVP below.
Solutions of Test: WPW and Brugada Syndrome & JVP questions in English are available as part of our course for NEET PG & Test: WPW and Brugada Syndrome & JVP solutions in
Hindi for NEET PG course.
Download more important topics, notes, lectures and mock test series for NEET PG Exam by signing up for free. Attempt Test: WPW and Brugada Syndrome & JVP | 10 questions in 10 minutes | Mock test for NEET PG preparation | Free important questions MCQ to study for NEET PG Exam | Download free PDF with solutions
Test: WPW and Brugada Syndrome & JVP - Question 1

Digoxin is not used in the management of? (Recent Question 2016-17)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 1
Test: WPW and Brugada Syndrome & JVP - Question 2
A 16-year old boy has history of recurrent episodes of fainting in-school assembly. ECG was done. What is incorrect about the condition?
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 2

Test: WPW and Brugada Syndrome & JVP - Question 3
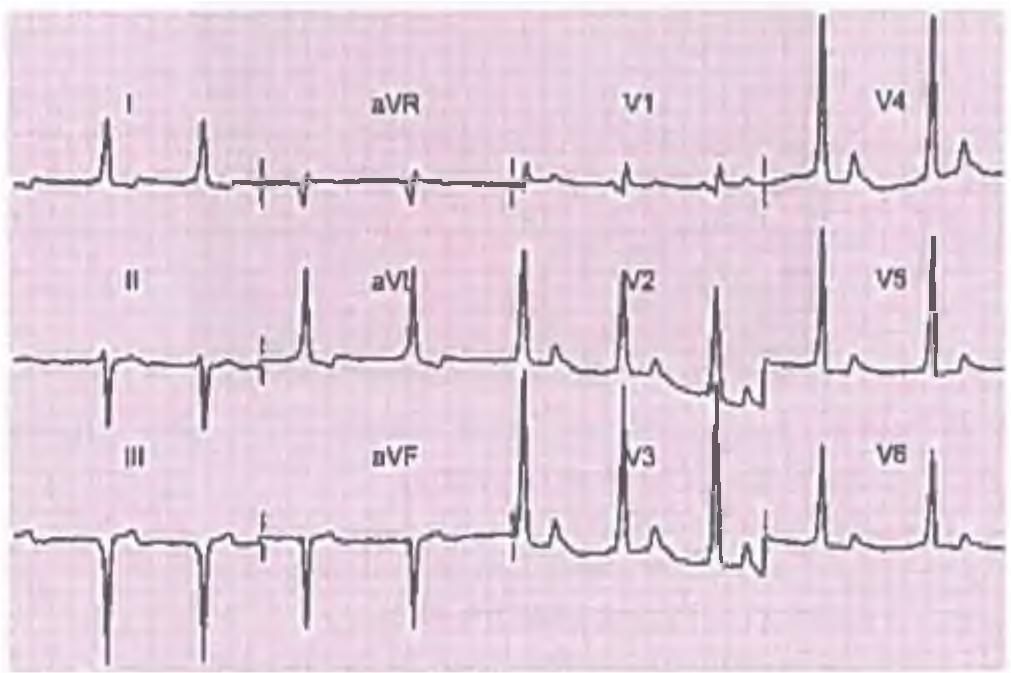
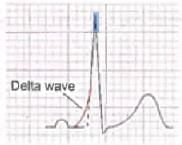
An 18-year-old boy is asymptomatic. On ECG he has a short PR interval with delta waves. Which of the following is not required for these patients? (AIIMS May 2013)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 3
Test: WPW and Brugada Syndrome & JVP - Question 4
What is incorrect about Brugada syndrome? (Recent Pattern 2014-15)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 4
Test: WPW and Brugada Syndrome & JVP - Question 5
Brugada Syndrome is associated with: (AIIMS 2013)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 5
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 6
Test: WPW and Brugada Syndrome & JVP - Question 7
In a patient of lung cancer with full neck veins and low BP, which of the following is incorrect? (Recent Pattern Questions)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 7
Test: WPW and Brugada Syndrome & JVP - Question 8
Internal jugular vein pressure determines pressure of: (Recent Question 2015-16)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 8
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 9
Test: WPW and Brugada Syndrome & JVP - Question 10
A wave in JVP is absent in: (Recent Question 2015-16)
Detailed Solution for Test: WPW and Brugada Syndrome & JVP - Question 10
Information about Test: WPW and Brugada Syndrome & JVP Page
In this test you can find the Exam questions for Test: WPW and Brugada Syndrome & JVP solved & explained in the simplest way possible.
Besides giving Questions and answers for Test: WPW and Brugada Syndrome & JVP, EduRev gives you an ample number of Online tests for practice
Download as PDF
Important Questions for WPW and Brugada Syndrome & JVP
Find all the important questions for WPW and Brugada Syndrome & JVP at EduRev.Get fully prepared for WPW and Brugada Syndrome & JVP with EduRev's comprehensive question bank and test resources.
Our platform offers a diverse range of question papers covering various topics within the WPW and Brugada Syndrome & JVP syllabus.
Whether you need to review specific subjects or assess your overall readiness, EduRev has you covered.
The questions are designed to challenge you and help you gain confidence in tackling the actual exam.
Maximize your chances of success by utilizing EduRev's extensive collection of WPW and Brugada Syndrome & JVP resources.
WPW and Brugada Syndrome & JVP MCQs with Answers
Prepare for the WPW and Brugada Syndrome & JVP within the NEET PG exam with comprehensive MCQs and answers at EduRev.
Our platform offers a wide range of practice papers, question papers, and mock tests to familiarize you with the exam pattern and syllabus.
Access the best books, study materials, and notes curated by toppers to enhance your preparation.
Stay updated with the exam date and receive expert preparation tips and paper analysis.
Visit EduRev's official website today and access a wealth of videos and coaching resources to excel in your exam.
Online Tests for WPW and Brugada Syndrome & JVP
Practice with a wide array of question papers that follow the exam pattern and syllabus.
Our platform offers a user-friendly interface, allowing you to track your progress and identify areas for improvement.
Access detailed solutions and explanations for each test to enhance your understanding of concepts.
With EduRev's Online Tests, you can build confidence, boost your performance, and ace WPW and Brugada Syndrome & JVP with ease.
Join thousands of successful students who have benefited from our trusted online resources.
|
© EduRev
|
Education Revolution
|



|









Signup on EduRev and stay on top of your study goals
10M+ students crushing their study goals daily