Test: Malabsorption Syndrome, Pediatric Gastroenterology & MALT-oma - NEET PG MCQ
25 Questions MCQ Test - Test: Malabsorption Syndrome, Pediatric Gastroenterology & MALT-oma

Which test is recommended for this patient? (Recent Question 2019)
Which is the most important complication of celiac sprue? (Recent Question 2016-17)

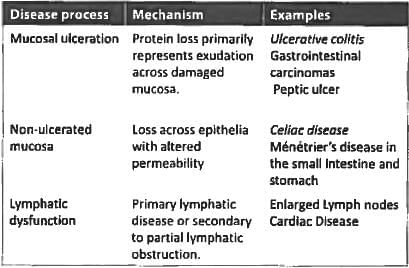
The following conditions can cause protein-losing enteropathy except? (UPSC 2015)
Malabsorption syndrome features include all, except: (Recent Pattern 2014-15)
Anti - T.T.G antibodies are seen in: (Recent Pattern 2014-15)
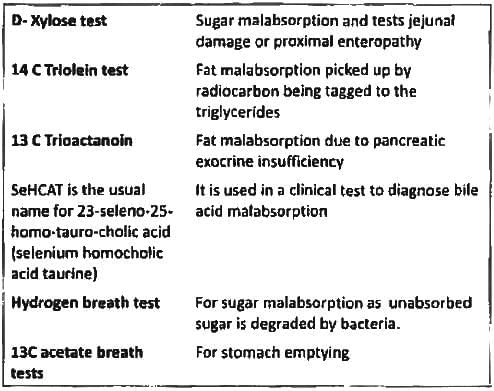
Xylose absorption test is used to assess: (Recent Pattern 2014-15)
Protein losing enteropathy is characterized by all except: (Recent Pattern 2014-15)
Alpha 1 anti-tryspin in stool is indicative of? (Recent Pattern 2014-15)
Jejunal biopsy is diagnostic in: (Recent Pattern 2014-15)
True about tropical sprue are A/E: (Recent Pattern 2014-15)
A 30-year-old lady presents with features of malabsorption and iron deficiency anaemia. Duodenal biopsy shows complete villous atrophy. Probable diagnosis is: (Recent Pattern 2014-15)
In celiac sprue there is a deficiency of all except: (Recent Pattern 2014-15)
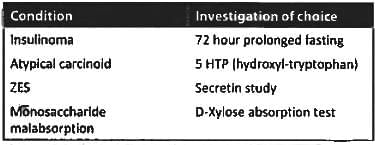
Not included in armamentarium of tests for malabsorption syndrome (AIIMS May 2013)
Malabsorption syndrome does not result from: (Recent Pattern 2014-15)
Non-tropical sprue is characterized by: (Recent Pattern 2014-15)
Consider the following:
a. Visible gastric peristalsis
b. Bilious vomiting
c. Palpable mass
d. Melena
Which of the above is/are the feature/features of infantile hypertrophic pyloric stenosis? (UPSC 2015)
A Term neonate with respiratory distress since birth. The CXR shows?

A neonate has been diagnosed with necrotizing enterocolitis with X ray abdomen showing gas in the portal vein. The correct staging of the patient is ? (Recent Pattern 2014-15)
Exposure to which of the following drugs is incriminated in IHPS (infantile hypertrophic pyloric stenosis): (Recent Pattern 2014-15)
All of the following are true regarding primary gastric lymphoma, except? (APPG 2016)
Which is the most common site of MALT? (AIMS Nov 2014)
Important Questions for Malabsorption Syndrome, Pediatric Gastroenterology & MALT-oma
Malabsorption Syndrome, Pediatric Gastroenterology & MALT-oma MCQs with Answers
Online Tests for Malabsorption Syndrome, Pediatric Gastroenterology & MALT-oma
|
© EduRev
|
Education Revolution
|



|








