Infanticide Foeticides and Child Abuse Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG PDF Download
| Table of contents |
|
| Introduction |
|
| Infanticide |
|
| Live Born, Stillborn and Dead Born Child |
|
| Feticide |
|
| Battered Baby Syndrome (Caffey Syndrome) |
|
| Sudden Infant Death Syndrome (SIDS) |
|
| Child Sexual Abuse |
|

Introduction
- During early life stages—such as intrauterine fetal development, infancy, and childhood—individuals are vulnerable to various adverse conditions, including diseases and trauma. These are broadly classified into three categories: (i) fetal death, which refers to the death of a fetus before birth; (ii) infant, newborn, or neonatal death, which involves the death of a child under one year of age due to natural or unnatural causes; and (iii) child abuse, encompassing maltreatment of a child for sexual or nonsexual purposes.
- The term "infanticide" originates from the Latin word infanticidium, meaning the killing of a child or infant (including newborns, babies, toddlers, etc.). Historically, infanticide has been practiced across all continents and by societies of varying cultural complexity, from hunter-gatherer communities to advanced civilizations, including our own ancestors. Far from being an exception, it has been a common practice. Historical records show that parents have often killed their children under various stressful circumstances. In 19th-century England, for instance, infanticide was widespread. Two primary reasons for infanticide stand out in history: poverty and population control. Charles Darwin noted that infanticide, particularly of female infants, was a significant factor in limiting population growth among early humans. While female infanticide was sometimes deemed necessary for the survival of the broader community, it was also frequently tied to societal biases against females, prevalent in many male-dominated cultures.
- The scale of female deaths is staggering. Estimates suggest that 30.5 million females are "missing" in China, 22.8 million in India, 3.1 million in Pakistan, 1.6 million in Bangladesh, 1.7 million in West Asia, 600,000 in Egypt, and 200,000 in Nepal. In India, the significant financial burden of raising a girl, including the costs of marriage and dowry, has historically been a key factor in the social acceptance of female infanticide. Girls were often viewed as mere consumers and a heavy economic load for impoverished families, leading to their frequent killing at birth.
Incidence
- In 1966, the United States reported a total of 10,920 murders, with a disturbing statistic showing that one in twenty-two victims was a child killed by a parent.
- Infanticide remains most common in regions experiencing extreme poverty.
- Historically, this crime has been associated primarily with mothers, and this pattern continues in contemporary society.
- Although men are generally more prone to commit murder, statistics reveal that mothers are usually the perpetrators in cases of infant killings.
- When mothers commit filicide, the victims are often newborns or infants under the age of one year.
- Research indicates that for children over one year old in the United States:
- White fathers are responsible for these murders 10% more often than white mothers.
- Black fathers commit these acts 50% more frequently than black mothers.
- The killing of female infants is predominantly observed in impoverished, rural communities.
- In India, the increase in the killing of female infants or fetuses is linked to:
- The low status of women
- Preference for male children
- Dowry practices prevalent across all caste groups
- Additional risk factors include:
- Young maternal age
- Low levels of education and employment
- Indicators of mental health issues, such as alcoholism or drug abuse
- Engagement in other criminal behaviors
- The most common methods of child killing involve:
- Head trauma
- Strangulation
- Drowning
- A significant number of contemporary murders are perpetrated by mothers, often through methods such as strangulation or physical punishment.
Infanticide
Definition
- Infanticide refers to the deliberate and illegal killing of a child who is under one year old, and this can occur either through direct action or failure to act.
- In the legal context of India, there is no differentiation in the treatment of crimes against children compared to those against adults.
- Consequently, infanticide is categorized as homicide under Indian law.
Investigation in a Case of Death of a Newborn and Infant
Examine the case through a detailed autopsy and provide answers to the following questions:
- Is the child viable ?
- Was the child live-born, stillborn, or dead-born?
- What was the time of survival if the child was live-born?
- What is the cause and manner of death?
Whether the Child is Viable or Not?
A viable child is one that is born alive and can exist independently after birth. Further questions, like live birth, survival duration, and cause of death, only come into play if the child is above the age of viability.
Medicolegal Significance
- When conducting an autopsy on a suspected case of infanticide, it is crucial to determine whether the child or newborn is viable. If the autopsy indicates non-viability, the charge of infanticide is dropped.
- Therefore, every doctor examining a suspected case must assess the viability of the child or fetus.
To establish viability, the infant should be examined using correct autopsy techniques, which include the following two methods:
- Assessing fetal developmental changes that indicate viability.
- Applying Haase's formula.
Fetal Developmental Changes:
- The fetus should be examined for developmental signs that suggest viability, including factors such as:
- Fetal Position:
- Muscle Tone:
- Organ Development:
- Skin Condition:
Haase's Rule:
- Haase's rule can be used to estimate the intrauterine age (IUA) of a fetus based on its crown-heel length.
Principles of Estimating Intrauterine Age (IUA)
- The age of a fetus can be estimated by taking the square root of its length in months.
- For lengths greater than 5 months, the length of the fetus in centimeters can be calculated by dividing the length by 5.
Up to 25 cm of crown-heel length
- Intrauterine age (IUA) in months is calculated by taking the square root of the length.
- For example, if the crown-heel length is 9 cm:
- IU Age = √9 = 3 months.
For crown-heel lengths exceeding 25 cm
- Intrauterine age (IUA) is calculated by dividing the length by five.
- For example, if the crown-heel length is 40 cm:
- IU Age = 40 × 1/5 = 40 ÷ 5 = 8 months.
Foetal autopsy: External and internal developmental changes of viability
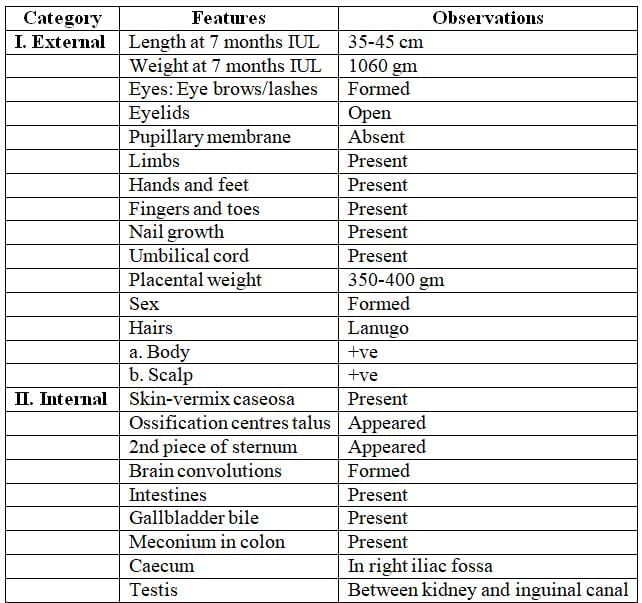
Measuring Crown-heel Length
- To measure the length of the fetus from the crown to the heel, the fetus is laid on a flat surface.
- A metallic scale or a flexible measuring tape can be used for this measurement.
- Alternatively, an osteometric board, which is designed for measuring long bones, can also be used.
Live Born, Stillborn and Dead Born Child
Live Born Child
- A child is classified as live born if any part of its body emerges from the mother's reproductive tract.
- This classification holds true even if the child has not taken a breath or is not fully delivered.
Stillborn Child
A stillborn child is one who is born after 28 weeks of pregnancy but shows no signs of life at any point during or after birth.
Changes in Fetal Length and Weight at Birth and After Birth

A Rough Method of Calculating the Age of the Fetus
Haase's Rule:
- Up to 5 months. Age of the fetus = Square root of length of fetus (in months)
- Over 5 months. Length of the fetus (in cm) / 5. (months)
For Confirmation of Age:
- Between 6 and 12 years: Dental examination is the best method.
- Between 14 and 25 years:
14 years: Patella completely ossifies.
14-25 years: Sternum fusion occurs from below upwards.
15-16 years: Elbow joint fusion.
16-17 years: Ankle joint fusion.
17-18 years: Hip joint fusion.
18-19 years: Knee, shoulder, and inner end of clavicle centres appear.
18-20 years: Iliac crest fuses.
21 years: Fusion of ischial tuberosity and inner end of clavicle.
22 years: Epiphyseal union of sternal end of clavicle.
Bertillon's System: For age over 21 years.
A stillborn child is one that has died in the uterus before the birth process begins. At birth, it may show signs of rigor mortis, maceration, or mummification.
 Foetus of different intrauterine age and developments
Foetus of different intrauterine age and developments
Establishing Whether Live Born?
In civil cases, the following signs indicate a live birth:
- The baby’s cry, known as vagitus, during vaginal delivery or in the uterus.
- Muscle twitching or movements of limbs.
In criminal cases, the presumption of death at birth is often confirmed by autopsy. Many jurisdictions presume that a newborn found dead was stillborn unless proven otherwise.
External Autopsy Observations
Overall Observations:
- The absence of vernix caseosa and the presence of clothing on the body indicate that the infant was born alive.
Ear Characteristics:
- The absence of embryonic connective tissue or the presence of air in the middle ear also suggest that the infant was born alive.
Chest Changes:
- Changes in the chest are crucial for determining whether the infant had respired, which helps to establish if the birth was live or stillborn.
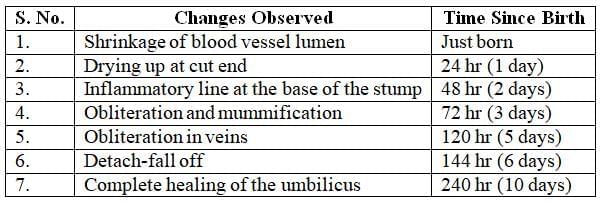
Umbilical Cord Changes:
- The presence of ligature marks or signs of crushing from artery forceps on the umbilical cord indicates live birth.
- Changes in the stump attached to the child provide additional evidence of live birth and help assess the time since birth.
Changes in the chest

Time since birth by changes in the umbilical cord
Internal Autopsy Observations
Indicators of live birth observed in the viscera, including the lungs, heart, and gastrointestinal tract, are as follows.
Changes in the Lungs
Alterations primarily result from respiration and are evidenced as follows.
Tests to Confirm Respiratory Changes in Lungs
- Pawlik's test
- Hydrostatic test (floatation test)
- Histological examination of lung
Pawlik's Test
This test assesses the weight of the lung in relation to the body weight. Normally, the lung-to-body weight ratio is approximately 1:30. If the lung has not undergone respiration, this ratio cannot be maintained.
Hydrostatic Test (Floatation Test)
In the second edition of his book "Forensic Pathology," Bernard Knight discusses the hydrostatic test, suggesting that it is an area lacking thorough research and practical application. However, I argue that salmon-pink, spongy lungs that float in water are indicative of an infant having breathed, provided there is no evidence of resuscitation or decomposition. Knight presents an example of aerated lungs floating in water in a case of suspected stillbirth without resuscitation, implying a live birth.
Principle: When air enters lung tissue during breathing, it decreases the tissue's density, allowing it to float in water. Normally, the specific gravity of lung tissue is around 1.0 before breathing, but after breathing, it changes to between 0.940 and 0.950, enabling the lungs to float.
Procedure
Dissect the fetal lungs.
Submerge both lungs in a trough of water and observe.
Lung changes due to respiration
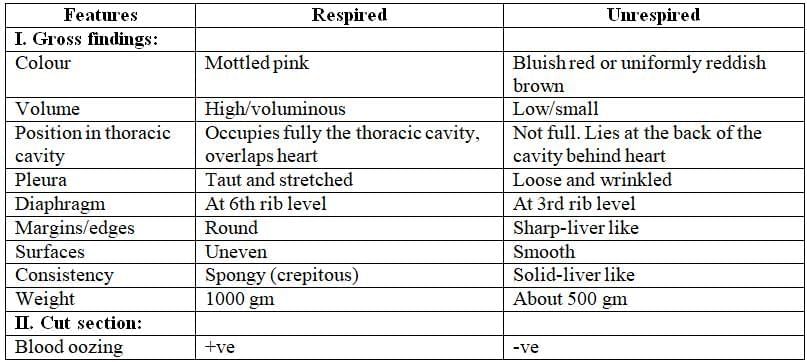
Inference
- If the lung pieces sink, it indicates an unrespired lung.
- If they float, remove them from the water, cut them into small pieces, and then place them back into the water column.
- If they float after being cut, it indicates a respired lung.
Explanation
The flotation observed in the test for the second time is primarily due to the residual air present in the lungs. This air cannot be expelled by pressing if the child has breathed after birth.
Fallacies
False-Positive Flotation: Flotation of lung pieces may falsely occur in conditions such as:
- Accumulation of putrefying gases in the lungs.
- Air being pushed into the lungs through artificial respiration.
False-Negative Sinking: Sinking of lung pieces may falsely occur in conditions such as:
- Atelectasis (lung collapse).
- Pneumonic consolidation.
Histology of Lung
- Unrespired Lung: The unrespired lung looks similar to a section of the parotid gland because its alveoli are lined with cuboidal epithelium.
- Foetal Lung Microscopy:
- (A) Before Respiration (Unrespired Lung): The immature alveoli in the foetal lung have not yet filled with air, giving the lung a glandular appearance.
- (B) After Respiration (Respired Lung): After respiration begins, the epithelium in the alveoli appears flattened, and the alveoli are expanded and filled with air.
- As air enters the lungs during respiration, the cells lining the alveoli flatten out, leading to a dilated pavement epithelium.
Heart Changes
Foramen Ovale. Ductus Arteriosus
- Foramen Ovale: This is a small hole between the two upper chambers of the heart (the right and left atria). In the fetus, oxygen-rich blood from the right atrium passes through this hole into the left atrium, and then into the left ventricle, which pumps it around the body.
- Ductus Arteriosus: This is a connection between the pulmonary artery (which carries blood to the lungs) and the aorta (the main artery that carries blood to the body). In the fetus, most blood from the right ventricle flows into the pulmonary artery, but instead of going to the lungs, it mostly passes through the ductus arteriosus into the aorta and then around the body, bypassing the lungs.
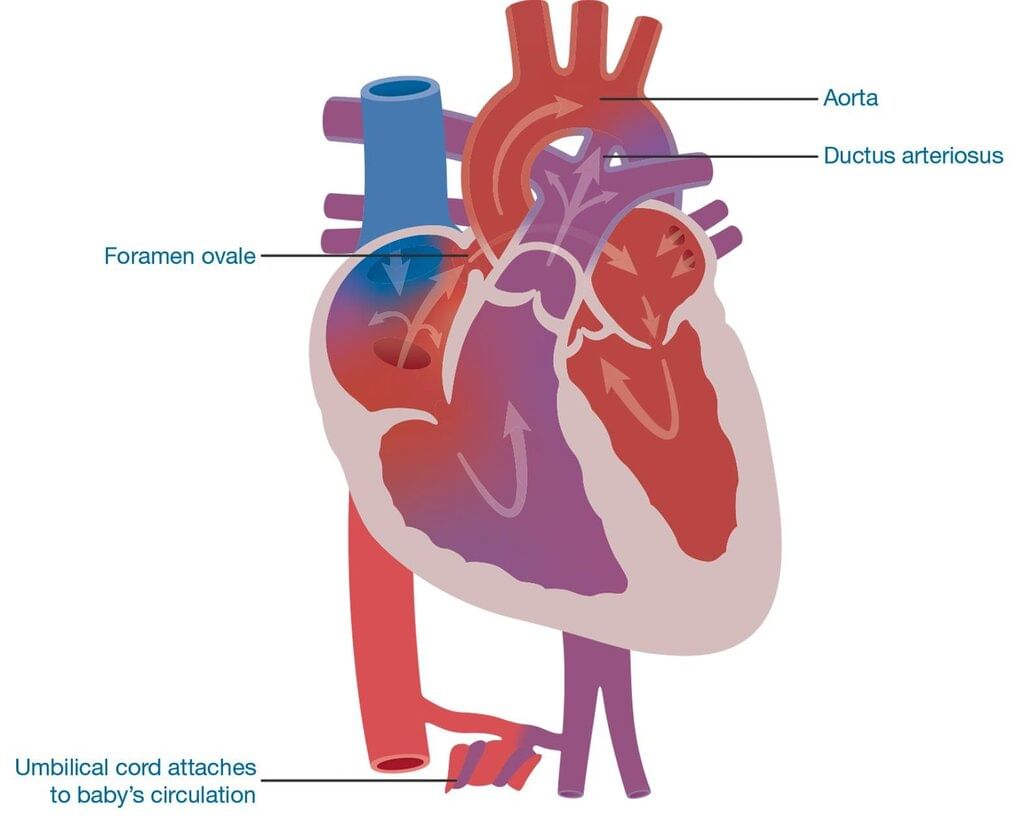 Showing foetal heart and blood flow in it
Showing foetal heart and blood flow in it
Bypass Function: The foramen ovale and ductus arteriosus act as bypass systems in fetal circulation, allowing blood to avoid the lungs, which are not yet in use.
Changes at Birth: When the baby is born and starts breathing on its own, these bypass systems are no longer needed. Gradually, in the first few days or weeks after birth, the ductus arteriosus closes, and the foramen ovale seals off. This changes the baby’s circulation to the normal pattern seen in adults.
Heart Changes Indicating Live Birth
- Ductus Arteriosus Closure: This usually happens on the fourth day after birth.
- Foramen Ovale Closure: This occurs by the second month after birth.
GIT Changes Indicating Live Birth
- Presence of Food and Saliva: Indicates that the stomach is functioning normally.
- Presence of Air in the Stomach: Shows that the stomach is not decomposing and is functioning properly.
- Presence of Meconium in the Intestine: Meconium is made up of intestinal secretions, cells, and bile. It is usually passed within 24 to 28 hours after birth. If meconium is present in the intestine, it suggests that the baby was born alive. However, if meconium is absent, it does not necessarily mean the baby was not born alive, as it can be voided in cases of breech delivery.
Establishing Whether Dead Born
A stillborn fetus may undergo a specific change called maceration.
Maceration refers to a condition of aseptic autolysis that occurs after the fetus has died in the womb. When examining a macerated fetus, the following characteristics are typically observed:
- Odour: Emits a rancid smell.
- Body: Soft and pliable; flattens when placed on a table.
- Skin: Sodden and coppery red or purplish (never greenish, as seen in putrefaction), with blisters and peeling cuticle.
- Abdomen: Distended.
- Umbilical cord: Thick, red, smooth, and soft.
- Joints: Abnormally mobile or flexible.
- Body cavity: Contains reddish serum.
- Organs/viscera: Soft and swollen, losing their shape, but lungs and uterus remain unaffected for a long time.
- Skull bones: Loss of alignment and overlapping of cranial bones (observed on radiograph, known as Spalding's sign. due to shrinkage of the brain shortly after death, which is visible within a few days.
Timeframe: Maceration begins 5 to 7 days before expulsion, so it takes approximately 5 to 7 days to develop.
Grades of Maceration
Maceration grades are determined by the outer features of the stillborn. The severity of maceration is classified into five grades:
- None
- Slight: Characterized by skin slippage, occasional blisters, minimal denudation (such as only the scrotum or a few spots of skin loss).
- Mild: Bultiple areas with focal denudation but no other significant changes.
- Moderate: Widespread skin maceration or denudation without major compressive alterations.
- Advanced: Involving compression, mummification, or internal liquefaction.
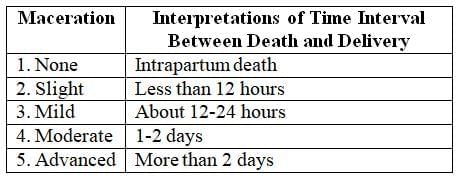
Understanding these grades helps in estimating the relationship between maceration severity and the time interval between death and delivery.
Showing six of the measures applicable scale used in grading maceration
Time of Survival If Live Born
- Caput succedaneum changes: This condition involves swelling (haematoma) in the skin of the baby's head due to the pressure during delivery. It typically begins to subside within 24 hours after birth and is completely resolved by day 7. If a baby exhibits this condition, their estimated survival time after birth is approximately 7 days.
- Umbilical cord changes: These changes are indicative of the baby's condition and can influence survival estimates.
- Spalding’s sign: This sign is observed in X-rays and ultrasounds of the fetal skull, where the skull bones and ribs appear overlapped, suggesting intrauterine death (IUD) of the fetus.
- Gastrointestinal changes: These changes are relevant in assessing the baby's condition and potential survival.
- Cardiovascular changes: Similar to gastrointestinal changes, cardiovascular alterations are important in evaluating the baby's health and survival chances.
- Changes in blood:
- Normoblasts are usually present for a few hours after birth.
- Fetal haemoglobin can be detected during the first six months after birth.
Causes of Death in Newborns
The death of a newborn can result from various factors. Perinatal autopsies in developed countries have identified a wide range of causes, with natural causes such as prematurity, debility, diseases, and congenital anomalies discussed elsewhere.
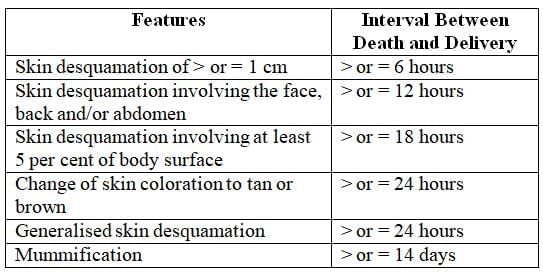
Time interval between death and delivery by maceration scale
Acts of Omission
These involve neglecting essential actions for an infant’s survival, including:
Failing to ligate the umbilical cord before cutting.
Not providing nourishment to the infant.
Under Section 317 of the Indian Penal Code (IPC), exposure and abandonment of a child under twelve years by a parent or caregiver is punishable by imprisonment of up to seven years, a fine, or both.
Acts of Commission
These involve deliberate actions leading to the infant’s death, such as:
Smothering the infant.
Strangulation.
Inflicting head injuries.
Prolonged Labour
In cases of prolonged labour, the fetus may die in utero due to maternal factors, including:
Contracted pelvis.
Cephalopelvic disproportion.
Precipitate Labour
In precipitate labour, the fetus dies during delivery, often in settings like a toilet or bathroom. This typically occurs in grand-multiparous women, where the three stages of labour merge into one, resulting in rapid delivery. The primary cause of infant death in such cases is usually head injury.
Cord Around the Neck
During delivery, the umbilical cord may accidentally wrap around the fetus’s neck, causing death by asphyxia. The cord acts as a ligature, similar to hanging or strangulation.
Feticide
Foeticide refers to the deliberate termination of a fetus, particularly female fetuses, before birth. This practice, a severe form of violence against females, is often facilitated by sex determination clinics and has become increasingly prevalent in India. In northern India, female fetuses are frequently aborted due to the availability of prenatal sex-determination technologies like ultrasound. In contrast, in southern India, where such tests and abortions are considered costly, female infanticide—killing the newborn girl after birth—is more common. Economic factors drive these practices, as daughters are often seen as financial burdens due to high wedding and dowry costs, while sons are viewed as sources of income and security.
Advancements in prenatal sex-determination techniques, such as ultrasound, have shifted the preference from female infanticide to abortion of female fetuses. This trend is exacerbated by the growing preference for smaller families. India’s sex ratio reflects this crisis, with 93 women for every 100 men nationally, and some regions reporting ratios below 85:100. A 1995 study in Mumbai hospitals highlighted the disparity, showing 1,000 female fetuses aborted for every male fetus aborted. The sex ratio has steadily declined, from 972 females per 1,000 males in 1901 to 933 per 1,000 in 2001.
To address this issue, the Pre-natal Diagnostic Techniques (PNDT) Act of 1994 was enacted, later amended in 2002 as the Preconception and Prenatal Diagnostic Techniques (Prohibition of Sex Selection) Act, 1994. The amendment accounted for technologies allowing sex selection before conception, such as sperm processing to separate X and Y chromosomes. Key provisions of the Act include:
- Regulation of Facilities: Genetic Counseling Centers, Laboratories, and Clinics must be registered to conduct prenatal diagnostic procedures and cannot employ unqualified personnel.
- Restrictions on Procedures: Prenatal diagnostic tests are permitted only under specific conditions, such as when the pregnant woman is over 35, has a history of multiple miscarriages, has been exposed to teratogenic agents, or has a family history of genetic disorders. Written consent in a language the woman understands is mandatory, and disclosing the fetus’s sex is strictly prohibited.
- Prohibition of Sex Selection: No facility or individual may use prenatal diagnostic techniques, including ultrasonography, to determine the fetus’s sex or facilitate sex selection before or after conception.
Offenses and Penalties under the Act include:
- Ban on Advertisements: Advertising services for sex determination or selection is illegal, punishable by up to three years imprisonment and a fine of up to ₹10,000.
- Violations by Medical Professionals: Medical geneticists, gynecologists, or other practitioners who violate the Act face up to three years imprisonment and a ₹10,000 fine for the first offense, with harsher penalties (up to five years imprisonment and a ₹10,000 fine) for subsequent offenses. Offending practitioners are reported to the State Medical Council for further action.
- Penalties for Individuals: Anyone seeking sex selection or prenatal diagnostic tests for sex determination faces up to three years imprisonment and a ₹50,000 fine for the first offense, with penalties increasing to five years imprisonment and a ₹100,000 fine for subsequent offenses.
Despite these legal measures, female foeticide remains a significant challenge in India, with the sex ratio continuing to decline, underscoring the need for stronger enforcement and societal change.
Statutes and Case Laws in Relation to Foetus in India
The legal perspective on the death of a child in the mother’s womb varies significantly. While it is not classified as homicide, it can be considered culpable homicide under certain circumstances. This is because foeticide involves the death of a living child within the womb, as outlined in Section 299 of the Indian Penal Code (IPC).
- Section 299 IPC clarifies that a human fetus is not regarded as a human being in legal terms.
- Infanticide is determined by the development of the fetus to a stage where it is recognized as human and has been born.
In a recent ruling by the Maharashtra State Commission in the case of Kanta Mohan Lal Kotehca Vs United India Insurance Co. Ltd, it was determined that a claim for an unborn child is legally valid.
In 2003, The Tribune covered a case involving a doctor couple facing legal action after a patient died during an abortion at their nursing home. The couple was accused of violating the PNDT Act as their nursing home’s registration had been suspended. Despite this, they performed a sonography on the patient without proper registration under the MTP Act (1971).
Initially charged under Section 304A of the IPC, the couple’s charges were later upgraded to Section 304 and Section 201, with additional sub-sections from the PNDT Act. During bail proceedings, the couple's lawyer argued that the doctors could perform an abortion to save the patient’s life, even without registration under the MTP Act. The lawyer contended that Section 304 IPC was not applicable due to lack of intent to kill.
The prosecution claimed the couple failed to keep necessary documents as per the Act. The State challenged the bail granted by the Magistrate in the Sessions Court, arguing the lower court exceeded its authority. The Sessions Court cancelled the bail, stating an offence under Section 304 IPC was applicable and ordered a re-evaluation of the bail application by the Chief Judicial Magistrate.
Battered Baby Syndrome (Caffey Syndrome)
Definition
Battered baby syndrome refers to a clinical condition typically seen in children under three years old who have experienced repeated, nonaccidental violence or injury inflicted by an adult, such as a parent, guardian, or foster caregiver. Alongside physical harm, these children may also suffer from intentional neglect, including lack of proper nutrition, care, or affection.
Causes
Victims are often unwanted children, born out of wedlock, or those whose paternity is questioned. Triggers for such abuse commonly include a child's crying that disrupts a parent's sleep, social plans, or activities like watching television. The act of battering often stems from a sudden loss of temper in such situations. Perpetrators frequently have low intelligence, a history of family conflict, chronic emotional issues, financial difficulties, or a criminal background. Many such adults were themselves victims of similar abuse during their childhood.
Injuries Sustained
Injuries are typically multiple, varying in severity, and follow a recognizable pattern. Common signs include severe localized bruises on the head that do not align with minor falls, as well as bruises on the face, trunk, or limbs resembling grip marks. Injuries like torn frenum of the upper lip or damaged gums, often caused to silence cries, are also frequent. Fatal injuries may include head trauma, such as skull fractures or subdural hematoma, or abdominal injuries, like a ruptured liver or mesenteric hemorrhage. Evidence from clinical exams and X-rays may show injuries occurring at different times, indicating repeated abuse.
Diagnosis of the Syndrome
Battered baby syndrome should be suspected in cases where:
The type or severity of injuries does not match the provided explanation.
Injuries show varying stages of healing, suggesting multiple incidents.
There is a delay in seeking medical care despite serious injuries.
The child exhibits signs such as bone fractures, subdural hematoma, failure to thrive, soft tissue swelling, or skin bruising.
The child experiences sudden, unexplained death.
Medicolegal Importance
The history provided by caregivers may be deceptive regarding the circumstances of the injury or death.
A thorough external and internal examination is critical, supported by photographs, radiographs, microscopic analysis of relevant lesions, and toxicological studies.
In India, cultural reverence for children as divine gifts makes battered baby syndrome rare. However, mistreatment of young children working as domestic servants is more common.
Such cases may lead to charges of infanticide.
Sudden Infant Death Syndrome (SIDS)
Definition
Sudden Infant Death Syndrome (SIDS) refers to the unexpected death of an apparently healthy infant, typically without any prior signs or symptoms that could predict such an event. Postmortem examinations reveal insufficient pathological findings to adequately explain the cause of death.
Incidence
SIDS occurs at a rate of 2–3 deaths per 1,000 live births. It most commonly affects infants aged between two weeks and six months, with a slightly higher prevalence in boys than girls. The condition is more frequent among low birth weight infants, those from lower-income families, and infants whose mothers smoke or use drugs. SIDS is often linked to seasonal upper respiratory infections, with approximately half of the cases showing cold-like symptoms in the week before death.
Causes
The exact cause of SIDS remains unclear, but several potential factors are suspected:
- Viral Infections: May contribute to the condition.
- Milk Allergy: Hypothesized as a possible trigger.
- Autobeverage Syndrome: Enzymatic activity in the stomach may convert milk into alcohol, leading to alcohol poisoning.
- Respiratory Infections: Often associated with SIDS cases.
- Overlaying: Occurs when a mother, while feeding the infant in a lying position, accidentally smothers the baby by pressing her breast against the infant’s face, causing suffocation.
- Sleep Apnea: A widely accepted theory suggests that pauses in breathing during sleep may lead to death.
- Shaken Infant Syndrome: Violent shaking during play can cause intracranial hemorrhage due to extreme neck movements, potentially resulting in death.
Autopsy Findings
Autopsies often reveal minimal fluid in the trachea, sometimes mixed with blood, and small petechial hemorrhages on the surfaces of the pleura, pericardium, and thymus. Microscopic evidence of respiratory inflammation is common. Other findings include signs of brief, intense muscle activity before death, empty bladder and bowels, and occasionally, blanket fibers under the infant’s fingernails.
Medicolegal Importance
SIDS cases may lead to investigations for infanticide, as the sudden and unexplained nature of the death can raise suspicions of foul play.
Child Sexual Abuse
Child Sexual Abuse (CSA) involves engaging dependent and developmentally immature children and adolescents in sexual activities that they do not fully comprehend, cannot consent to, or that breach social norms or family roles. It is a pervasive issue that necessitates a multidisciplinary approach for diagnosis and management, involving not only medical professionals but also social services and law enforcement agencies.
Rape of a child is a form of Child Sexual Abuse (CSA). When a parent or close relative, such as a grandparent, aunt, or uncle, commits this act, it is referred to as incest. If another child, usually older or stronger, is the perpetrator, it is called child-on-child sexual abuse.
When a child is sexually abused by a family member, particularly a parent, it can cause severe and lasting psychological trauma. Similarly, if an adult caregiver or authority figure, who is not a family member, commits the act, the impact can be comparable to that of incest.
Psychologists estimate that 40 million adults in the United States were sexually abused as children, including 15 million men (Adams 1991). Many of these abuses were perpetrated by parents, relatives, or trusted adults. The National Centre for Victims of Crime reports that 46 per cent of rapes in the United States are committed by a family member.
The effects of child rape can include: Effects of Child Rape
- Depression
- Post-traumatic stress disorder (PTSD)
- Anxiety
- Increased risk of re-victimization in adulthood
- Physical injury
Children, particularly adolescents, who are raped by parents or close relatives are often referred to as 'secret survivors'. They may remain silent about the abuse due to:
- Threats from the abuser
- Fear of abandonment
- Feelings of shame
Signs of such abuse are often not apparent except to trained professionals, leading to prolonged suffering in silence until the child can escape the abuser. By that time, the statute of limitations may have lapsed, and repressed memories might not be admissible as evidence, allowing the abuser to evade punishment.
In South Africa, over 67,000 cases of rape and sexual assault against children were reported in 2000. Child welfare organizations believe that the actual number of unreported cases could be up to ten times higher. A widespread belief in South Africa is that sexual intercourse with a virgin can cure a man of HIV or AIDS. The country has one of the highest rates of HIV-positive individuals globally, with one in eight South Africans infected.
Edith Kriel, a social worker in the Eastern Cape, remarked: "Child abusers are often relatives of their victims—even their fathers and providers."
Suzanne Leclerc-Madlala, an anthropology lecturer, observes that the myth of sex with a virgin as a cure for AIDS extends beyond South Africa, affecting countries like Zambia, Zimbabwe, and Nigeria, and contributing to high rates of sexual abuse against children.
Incest between fathers and daughters is more prevalent than reported globally. However, there has been a significant rise in claims of sexual abuse in recent years. In lower social classes, the erroneous belief that venereal diseases can be cured through sex with a virgin persists, making female children frequent victims.
Examination of the CSA Case
- Forming opinions on serious issues can be difficult for an examining doctor unless they have significant experience.
- It is important to recognise the wide variety of normal appearances of the genitalia and anus in order to provide a trustworthy opinion.
- A digital examination of a prepubertal child is rarely necessary and may require general anaesthesia if deemed essential.
Reflex Anal Dilation Test
- The Reflex Anal Dilation Test is controversial and should be used as part of the overall examination, rather than being solely relied upon.
- During the procedure, the child is positioned in the left lateral position, with the buttocks gently separated, rather than in the knee-elbow position.
- A positive result is indicated by the relaxation of the external sphincters within 30 seconds, allowing visibility of the anal canal's interior.
- It is important that this dilatation lasts for several seconds, as quick reflex puckering is not diagnostic.
- Additionally, it is crucial to consider the possibility of sexually transmitted diseases, which has both diagnostic and therapeutic implications for the examining doctor.
|
135 docs|3 tests
|
FAQs on Infanticide Foeticides and Child Abuse Chapter Notes - Forensic Medicine and Toxicology (FMT) - NEET PG
| 1. What is the definition of incidence in the context of newborn and infant deaths? |  |
| 2. How can one investigate a case of death in a newborn or infant? | |
| 3. What factors determine whether a child is considered viable or not? | |
| 4. What is the medicolegal importance of determining whether a child is live-born or stillborn? | |
| 5. How is crown-heel length measured, and why is it significant in assessing newborns? | |


MCQs
,Extra Questions
,ppt
,Objective type Questions
,Exam
,shortcuts and tricks
,Semester Notes
,past year papers
,mock tests for examination
,Previous Year Questions with Solutions
,practice quizzes
,Important questions
,Free
,Sample Paper
,Infanticide Foeticides and Child Abuse Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,Infanticide Foeticides and Child Abuse Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,Viva Questions
,video lectures
,study material
,Infanticide Foeticides and Child Abuse Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,Summary
;






Chapter Notes: Infanticide Foeticides and Child Abuse Free PDF Download
Importance of Chapter Notes: Infanticide Foeticides and Child Abuse
Chapter Notes: Infanticide Foeticides and Child Abuse
Chapter Notes: Infanticide Foeticides and Child Abuse NEET PG Questions
Study Chapter Notes: Infanticide Foeticides and Child Abuse on the App
|
© EduRev
|
Education Revolution
|



|





