NEET PG Exam > NEET PG Notes > Microbiology > Chapter Notes: Plasmodium Species and Babesia
Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG PDF Download

Plasmodium
Plasmodium species responsible for malaria include the following:
- Species: Plasmodium vivax, Disease: Benign tertian, Periodicity (Hours): 48
- Species: Plasmodium falciparum, Disease: Malignant tertian, Periodicity (Hours): 48
- Species: Plasmodium ovale, Disease: Ovale tertian, Periodicity (Hours): 48
- Species: Plasmodium malariae, Disease: Quartan, Periodicity (Hours): 72
- Species: Plasmodium knowlesi, Disease: Quotidian, Periodicity (Hours): 24
Life Cycle
- Definitive host involves female Anopheles mosquitoes.
- Intermediate host is humans.
- Infective form to humans consists of sporozoites located in the mosquito's salivary gland.
- Infective form to humans via blood transfusion or vertical transmission is the trophozoite.
- Differences in life cycle when transmitted by blood transfusion or vertical mode include:
- Absence of liver stage, with infective form being trophozoite leading to merozoite.
- No production of hypnozoites.
- Therefore, no relapse occurs.
- Hence, primaquine is not required.
- Infective form to mosquito is the gametocyte.
- For mosquitoes to be infected, gametocytes must be mature, viable, and present in counts greater than 12 per cubic mm of blood.
- Asexual cycle in humans:
- Following mosquito bite, sporozoites enter blood and are transported to liver.
- Liver cycle (pre or exoerythrocytic cycle): Sporozoites change into trophozoites, then pre-erythrocytic schizont performs schizogony to yield pre-erythrocytic (PE) merozoites.
- RBC cycle: PE merozoites enter RBCs, become early trophozoites (ring form), progress to late trophozoites, then erythrocytic schizont, which undergoes schizogony to form merozoites.
- Merozoite release causes clinical symptoms to appear.
- Merozoites can either invade more RBCs to continue the cycle or develop into gametocytes that can infect mosquitoes.
- Sexual cycle (Sporogony): Starts with gametocytes entering female Anopheles mosquito, transforming into gametes, then zygote, ookinete, oocyst, and finally sporozoites.
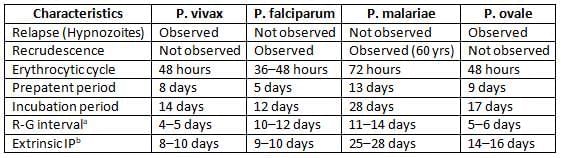
Recrudescence
Observed in infections by P. falciparum and P. malariae.- In P. falciparum malaria: Caused by survival of drug-resistant parasites, with fever returning after 2–3 weeks post-treatment.
- In P. malariae infection: Long-term recrudescences can occur up to 60 years, due to prolonged survival of erythrocytic stages at low, undetectable levels in blood.
Relapse
- Caused by hypnozoites (dormant stage) that can reactivate after 2-3 years of malaria infection.
- Occurs in P. vivax and P. ovale.
- Treatment for relapse involves primaquine.
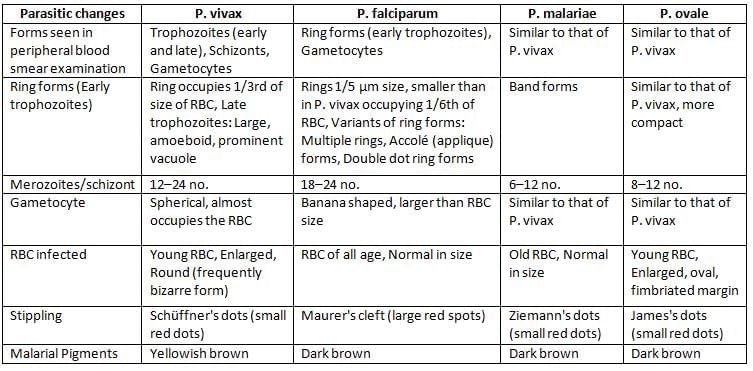
Differences between the four malaria parasites
Pathogenesis of P. falciparum
- Sequestration refers to parasites being retained in blood vessels of deep organs like brain and kidney, causing vascular blockage.
- Cytoadherence involves binding of RBC to endothelium via Pf EMP.
- Rosetting occurs when unparasitized RBCs cluster with parasitized RBCs.
- Cytokines are released due to GPI (glucosylphosphatidyl Inositol).
- Antigenic diversity exists in Pf EMP.
Immunity
- Nature of Hemoglobin:
- Sickle cell anemia trait provides protection from P. falciparum.
- Thalassemia trait offers protection from P. falciparum.
- Fetal Hb gives protection from P. falciparum.
- Nature of RBC:
- P. falciparum infects RBCs of all ages.
- P. malariae infects old RBCs.
- P. ovale and P. vivax infect young RBCs.
- Nature of Enzyme: G6PD deficiency protects from P. falciparum.
- Ovalocytosis makes RBC rigid, protecting from P. falciparum.
- Duffy negative RBC protects from P. vivax.
- HLA-BW53 and haplotypes with DRW13.02 antigen and R111 gene contribute to immunity.
- Nutritional status has a paradoxical effect.
- Predisposing factors:
- Density of the vector.
- Number of human bites per day per mosquito.
- Time of mosquito bite (more after dusk).
- Optimum temperature (20–30 °C).
- Optimum humidity (60%).
- Rainfall (July to November).
- Altitude below 2000 meters.
- Mosquito longevity (as sporogony lasts for 7–30 days, thus, to transmit malaria, the mosquito must live > 7 days).
Epidemiology
Situation in World
- Most affected area is Sub-Saharan Africa (85%), followed by South East Asia Region (SEAR) (10%) and Mediterranean (4%).
- P. vivax is the predominant species.
- Age: Children are most affected.
Situation in India
- P. falciparum accounts for 51% and P. vivax for 49%, with few mixed infections reported.
- 22% of people live in high transmission areas (≥ 1 case per 1000).
- 67% in low transmission areas (0–1 case per 1000).
- 11% in malaria-free areas.
- Odisha is most affected (24%), with 92% cases due to P. falciparum.
- P. malariae is less than 1% in India, mainly in Tumkur and Hassan districts of Karnataka.
- P. ovale is confined to tropical Africa, with only few cases from India (Odisha, Delhi, Assam, Gujarat, and Kolkata).
- Roll back malaria: Launched in 2000, aims to reduce malaria cases by 50% by end of 2010 and 75% by end of 2015.
- World malaria day: Observed every year on 25th April.
Clinical Features of Malaria
- Fever.
- Sweating.
- Anemia.
- Splenomegaly (enlarged spleen).
- Irritability.
- Coma.
- Retinal Hemorrhages.
- Algid Malaria (a shock-like syndrome).
- Respiratory distress syndrome.
Complications
- Cerebral malaria.
- Black water fever.
- Tropical splenomegaly syndrome.
- Malarial hyperpyrexia.
- Gastrointestinal disorders.
- Algid malaria.
- Nephrotic syndrome: Associated with P. malariae infection.
- Promotes Burkitt’s Lymphoma.
Plasmodium Knowlesi
- It is a malaria parasite primarily of monkeys but can infect humans, recently reported from Asia.
- Not reported from India yet, although the vector Anopheles leucosphyrus is present in southwest coastal region.
- Large focus of P. knowlesi in humans: Recently identified in Malaysia, Singapore, and Thailand.
- Blood smear examination: Early trophozoite resembles P. falciparum, and late trophozoite resembles P. malariae.
- Produces acute illness and relatively high parasitaemia compared to P. malariae.
- Paroxysms of fever occur daily (quotidian malaria) due to short RBC cycle.
Laboratory Diagnosis
Microscopic Tests
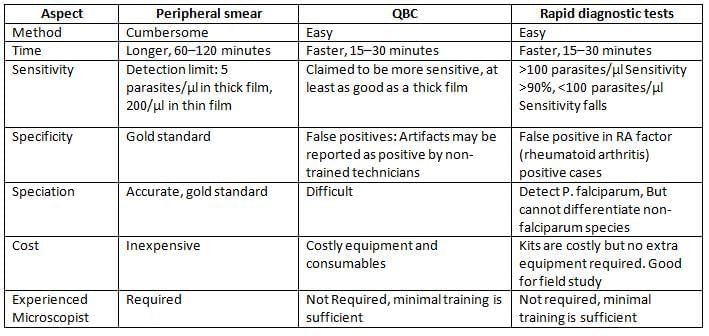
- Examination of peripheral blood smears (thin and thick blood films): Considered the gold standard method.
- Thick smear: More sensitive (40 times), used for quantification and detection of malaria pigment.
- Thin smears: Used for species identification.
- Feathery tail end of the smear should be examined.
- At least 200–300 oil immersion fields should be examined before declaring negative.
- Stains used:
- JSB (Jaswant Singh and Bhattacharya) stain – Used in malaria control programme in India.
- Leishman’s, Giemsa, and Field’s, Wright’s.
- Fluorescence microscopy (Kawamoto technique) - by Acridine orange stain.
- Quantitative Buffy coat examination (QBC): Rapid method for parasite detection.
- Blood is collected in a capillary tube coated with acridine orange, then centrifuged, and buffy coat region (junction of RBC & WBC) examined under UV.
Non-microscopic Tests
- Antigen detection tests: Rapid diagnostic tests (RDTs) or Immunochromatographic tests (ICTs).
- Rapid and simple but less sensitive, costly, and may give false positives in RA factor positive cases.
- pLDH and Aldolase: Common to all Plasmodium species.
- HRP-2 Ag detection: Specific for P. falciparum.
- Antibody detection methods:
- Used for epidemiological surveys in malaria.
- Screening of blood banks: To identify infected donors.
- Culture of malarial parasites: Tragger and Jensen method using RPMI 1640 medium is used for research purposes.
- Molecular methods - PCR using PBRK1 primer.
- It is 100 times more sensitive than thick blood smear.
- Speciation can be performed.
- Drug resistance genes can be detected.
Comparison of Peripheral Smear, QBC and Rapid Diagnostic Tests
Treatment
Uncomplicated Benign Malaria in India
- Chloroquine remains the drug of choice for uncomplicated benign malaria in India, administered as 25 mg/kg divided over three days.
- Relapse rate of vivax malaria is around 30% in India. Primaquine is administered as 0.25 mg/kg daily for 14 days to prevent relapse.
Complicated or Falciparum Malaria in India
Treatment of falciparum malaria in India depends on whether the area is resistant or sensitive to chloroquine.
- Artemisinin combination therapy (ACT) is recommended in chloroquine resistant areas, whereas chloroquine can be used in sensitive areas.
- Artemisinin combination therapy (ACT) includes a combination of artemisinin derivative (Artemisinin or artemether or arte-ether) and long-acting antimalarial drugs like sulfadoxine-pyrimethamine, mefloquine, or lumefantrine.
- For treatment failure of P. falciparum cases: Quinine combined with doxycycline or tetracycline is recommended.
- Chloroquine resistant areas where Artemisinin combination therapy (ACT) is recommended: Odisha, Jharkhand, Madhya Pradesh, Chhattisgarh, and Andhra Pradesh.
- In pregnancy: Quinine is recommended in first trimester, whereas Artemisinin combination therapy (ACT) is given in second and third trimester.
- Treatment of unconfirmed cases or mixed infection with P. falciparum should be treated as falciparum malaria, plus primaquine is given for radical cure.
Babesia
- Intraerythrocytic protozoa.
- Causes malaria-like illness in animals and zoonotic opportunistic infections in humans.
- Not found in India.
- Vector: Tick borne.
- Treatment: Clindamycin with oral quinine and atovaquone and azithromycin.
- Differences from Plasmodium:
- Hemozoin absent.
- Gametocyte not distinguished from asexual forms.
- Maltese cross form seen: Ring forms arranged in tetrad.

The document Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG is a part of the NEET PG Course Microbiology.
All you need of NEET PG at this link: NEET PG
|
75 docs|5 tests
|
FAQs on Plasmodium Species and Babesia Chapter Notes - Microbiology - NEET PG
| 1. What is the life cycle of Plasmodium species that cause malaria? |  |
Ans. The life cycle of Plasmodium species involves two hosts: the female Anopheles mosquito and humans. In the mosquito, the sexual phase occurs. When a mosquito bites an infected human, it ingests gametocytes, which develop into sporozoites in the mosquito's gut. These sporozoites migrate to the salivary glands and are transmitted to humans during subsequent bites. In humans, the sporozoites enter the bloodstream and infect liver cells, where they multiply and release merozoites into the bloodstream. Merozoites then invade red blood cells, leading to the characteristic symptoms of malaria. Some merozoites develop into gametocytes, which can be taken up by another mosquito, continuing the cycle.
| 2. What are the clinical features of malaria caused by Plasmodium falciparum? | |
Ans. Clinical features of malaria caused by Plasmodium falciparum include high fever, chills, sweats, headache, nausea, vomiting, and fatigue. Symptoms typically occur in cyclical patterns, often every 48 hours. Severe cases may lead to complications such as cerebral malaria, anemia, respiratory distress, and multi-organ failure. The rapid progression of the disease can result in significant morbidity and mortality if not treated promptly.
| 3. How does the epidemiology of malaria in India reflect the findings of the WHO Malaria Report? | |
Ans. According to the WHO Malaria Report, India has made significant strides in reducing malaria cases and mortality rates through various public health interventions. However, certain regions, particularly in the northeastern states, continue to report high transmission rates. The report highlights the importance of continued surveillance, vector control measures, and access to effective antimalarial treatments to combat malaria in India. Variability in incidence is influenced by factors such as climate, urbanization, and socio-economic conditions.
| 4. What are the complications associated with malaria? | |
Ans. Complications of malaria can be severe and include cerebral malaria, characterized by altered consciousness and seizures; severe anemia due to hemolysis of red blood cells; acute respiratory distress syndrome (ARDS); and multi-organ failure affecting the liver, kidneys, and spleen. Pregnant women and young children are particularly at risk for these complications, which can lead to increased morbidity and mortality. Prompt diagnosis and treatment are crucial to prevent these severe outcomes.
| 5. How is Plasmodium knowlesi different from other Plasmodium species? | |
Ans. Plasmodium knowlesi is primarily a zoonotic malaria parasite that is transmitted from macaques to humans, unlike other Plasmodium species, which are primarily transmitted between humans. It is endemic in certain Southeast Asian regions and can cause malaria with symptoms similar to those of Plasmodium falciparum. However, it often presents with a different clinical profile and can lead to severe disease if not diagnosed and treated promptly. The recognition of P. knowlesi has implications for malaria control and elimination strategies in affected regions.
About this Document

Oct 10, 2025
Last updated
Document Description: Chapter Notes: Plasmodium Species and Babesia for NEET PG 2025 is part of Microbiology preparation.
The notes and questions for Chapter Notes: Plasmodium Species and Babesia have been prepared according to the NEET PG exam syllabus. Information about Chapter Notes: Plasmodium Species and Babesia covers topics
like Plasmodium, Babesia and Chapter Notes: Plasmodium Species and Babesia Example, for NEET PG 2025 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Chapter Notes: Plasmodium Species and Babesia.
Introduction of Chapter Notes: Plasmodium Species and Babesia in English is available as part of our Microbiology
for NEET PG & Chapter Notes: Plasmodium Species and Babesia in Hindi for Microbiology course.
Download more important topics related with notes, lectures and mock test series for NEET PG
Exam by signing up for free. NEET PG: Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG
Description
Full syllabus notes, lecture & questions for Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG - NEET PG | Plus excerises question with solution to help you revise complete syllabus for Microbiology | Best notes, free PDF download
Information about Chapter Notes: Plasmodium Species and Babesia
In this doc you can find the meaning of Chapter Notes: Plasmodium Species and Babesia defined & explained in the simplest way possible. Besides explaining types of
Chapter Notes: Plasmodium Species and Babesia theory, EduRev gives you an ample number of questions to practice Chapter Notes: Plasmodium Species and Babesia tests, examples and also practice NEET PG
tests

Related Searches
shortcuts and tricks
,Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG
,Sample Paper
,Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG
,Semester Notes
,past year papers
,practice quizzes
,Plasmodium Species and Babesia Chapter Notes | Microbiology - NEET PG
,mock tests for examination
,Extra Questions
,Summary
,Important questions
,Previous Year Questions with Solutions
,Viva Questions
,Free
,ppt
,study material
,MCQs
,Objective type Questions
,video lectures
,Exam
;






Additional Information about Chapter Notes: Plasmodium Species and Babesia for NEET PG Preparation
Chapter Notes: Plasmodium Species and Babesia Free PDF Download
The Chapter Notes: Plasmodium Species and Babesia is an invaluable resource that delves deep into the core of the NEET PG exam.
These study notes are curated by experts and cover all the essential topics and concepts, making your preparation more efficient and effective.
With the help of these notes, you can grasp complex subjects quickly, revise important points easily,
and reinforce your understanding of key concepts. The study notes are presented in a concise and easy-to-understand manner,
allowing you to optimize your learning process. Whether you're looking for best-recommended books, sample papers, study material,
or toppers' notes, this PDF has got you covered. Download the Chapter Notes: Plasmodium Species and Babesia now and kickstart your journey towards success in the NEET PG exam.
Importance of Chapter Notes: Plasmodium Species and Babesia
The importance of Chapter Notes: Plasmodium Species and Babesia cannot be overstated, especially for NEET PG aspirants.
This document holds the key to success in the NEET PG exam.
It offers a detailed understanding of the concept, providing invaluable insights into the topic.
By knowing the concepts well in advance, students can plan their preparation effectively.
Utilize this indispensable guide for a well-rounded preparation and achieve your desired results.
Chapter Notes: Plasmodium Species and Babesia
Chapter Notes: Plasmodium Species and Babesia Notes offer in-depth insights into the specific topic to help you master it with ease.
This comprehensive document covers all aspects related to Chapter Notes: Plasmodium Species and Babesia.
It includes detailed information about the exam syllabus, recommended books, and study materials for a well-rounded preparation.
Practice papers and question papers enable you to assess your progress effectively.
Additionally, the paper analysis provides valuable tips for tackling the exam strategically.
Access to Toppers' notes gives you an edge in understanding complex concepts.
Whether you're a beginner or aiming for advanced proficiency, Chapter Notes: Plasmodium Species and Babesia Notes on EduRev are your ultimate resource for success.
Chapter Notes: Plasmodium Species and Babesia NEET PG Questions
The "Chapter Notes: Plasmodium Species and Babesia NEET PG Questions" guide is a valuable resource for all aspiring students preparing for the
NEET PG exam. It focuses on providing a wide range of practice questions to help students gauge
their understanding of the exam topics. These questions cover the entire syllabus, ensuring comprehensive preparation.
The guide includes previous years' question papers for students to familiarize themselves with the exam's format and difficulty level.
Additionally, it offers subject-specific question banks, allowing students to focus on weak areas and improve their performance.
Study Chapter Notes: Plasmodium Species and Babesia on the App
Students of NEET PG can study Chapter Notes: Plasmodium Species and Babesia alongwith tests & analysis from the EduRev app,
which will help them while preparing for their exam. Apart from the Chapter Notes: Plasmodium Species and Babesia,
students can also utilize the EduRev App for other study materials such as previous year question papers, syllabus, important questions, etc.
The EduRev App will make your learning easier as you can access it from anywhere you want.
The content of Chapter Notes: Plasmodium Species and Babesia is prepared as per the latest NEET PG syllabus.
|
© EduRev
|
Education Revolution
|



|






Signup to see your scores
go up within 7 days!
Access 1000+ FREE Docs, Videos and Tests
Takes less than 10 seconds to signup