Firearms and Explosive Injuries - 3 Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG PDF Download
| Table of contents |
|
| Gunshot Wounds Caused by Rifled Firearms |
|
| Peculiar Effects of Rifled Firearms/ Gunshot Wounds |
|
| Gutter Fracture |
|
| Shotgun Wounds |
|

Gunshot Wounds Caused by Rifled Firearms
Gunshot wounds are injuries inflicted by rifled firearms, which are commonly referred to as guns. When a gun is discharged, various elements are released, each playing a distinct role in impacting the wound. These elements include:
- The bullet or projectile
- Smoke containing soot particles
- Unburnt gunpowder particles
- Hot combustion gases
- Gun flame
While the bullet is the primary cause of injury, the other elements can also affect the wound's characteristics, especially depending on the distance from which the gun was fired.
- Heat Combustion Effect
- Soiling of the Wound
- Smudging
- Blackening
- Tattooing
- Blast Effects
- Facial Distortion Effects
- Cherry Red Discoloration
- Abrasion and Grease Collar
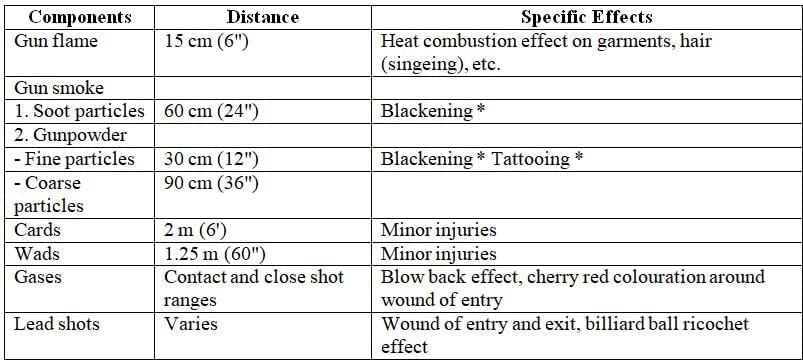
Distance travelled by the components of rifle firearm discharge and the special effects produced by them
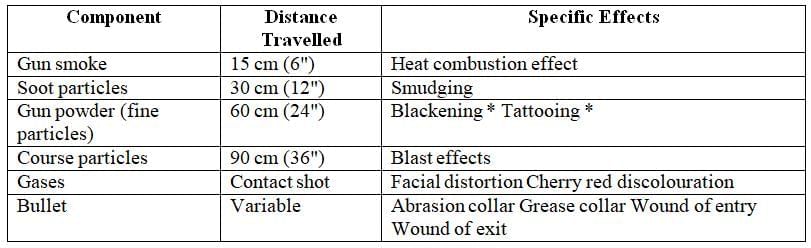
* Collectively called soiling of the wound
Heat Combustion Effects
When a gun is fired, the flame that shoots out from the muzzle creates a combustion effect due to its high temperature. This intense heat can impact the clothing and hair surrounding the entry wound.
Effects on Garments: There are three primary changes observed in garments:
- Ironing Effect: The cloth looks as if it has been freshly pressed with a hot iron.
- Melting Effect: This is particularly noticeable in synthetic fabrics.
- Burning Effect: This effect is especially evident in non-synthetic natural fibres.
Effects on Hair: The changes in hair are referred to as singeing, which is commonly observed with contact shots:
- Singed hair appears grossly swollen, curly, and fragile, to the point where touching it can cause it to fall out.
- For blondes, the singed hair may appear blackish and emit a peculiar odour due to the burning of keratin.
- The tips of the hairs are swollen and resemble the bulb or root of the hair.
Microscopy: Microscopic examination reveals an increase in hair width and the presence of vacuoles within the hair shaft.
Medicolegal Importance: The combustion effects hold significance in medicolegal investigations as they can assist in:
- Distinguishing between entry and exit wounds.
- Assessing the firing range, including contact, near contact, and close shots.
Soiling of the Wound
- Gunsmoke from burnt powder causes the soiling effect, usually visible around the entry wound on the skin or clothing.
- Smudging or blackening occurs due to smoke particles, lead, or metal from the bullet.
- Tattooing or peppering happens when fine or coarse gunpowder particles embed into the skin, leaving marks that cannot be washed off.
- Medicolegal importance—Smudging and tattooing help determine the firing range:
- Close Range: If both smudging and tattooing are present, it indicates the shot was close or near.
- Distant Range: If both smudging and tattooing are absent, the shot was from a distance.
- Contact Shot: If tattooing is deeper, such as on the inner part of the wound, it suggests a contact shot.
- Near Range: If only tattooing is present, the shot was near.
- Fading of Marks: As the range increases, blackening fades first, followed by tattooing, because their sources cannot travel far.
Blast Effect
- Blast effects are caused by the hot gases produced during the combustion of gunpowder, and they are observed around the entry wound of a bullet. These effects are linked to the high pressure of the gases, which disrupt tissues at the point of entry.
- When a gun is fired at close range, with the muzzle pressed against the target (a contact shot), gases such as carbon monoxide (CO) and carbon dioxide (CO2) are released due to the burning of gunpowder, creating intense pressure. This pressure causes the gases to accumulate between the skin and the underlying tissues, particularly over bony areas like the skull, leading to a blast effect.
- Tearing of skin: The gases forcefully push to escape the wound, causing the skin to tear.
- Eversion of wound edges: The edges of the wound turn outward as the gases attempt to escape.
- Muzzle end imprint abrasion: The skin is pushed forward by the force of the gases and comes into contact with the muzzle end of the weapon.
- Formation of blood and gunpowder pocket: If the wound is small, blood and gunpowder can accumulate beneath the skin.
- Pressure extrusion: Fibers from fabric, soft tissues, blood, and fat can be pushed out of the wound along with the escaping gases.
- Contamination of bones (periosteum) and clothing: Soot particles can enter the wound at contact shot range, contaminating the bones and clothing.
Effects of Facial Distortion
- When a bullet strikes the head, gases from the gunshot can enter the skull.
- This causes a rapid increase in pressure inside the skull, which is rigid and cannot expand easily.
- As a result, pressure builds up, leading to fractures and the displacement of bone fragments.
- These sharp bone fragments can create tears (lacerations) in the skin of the face, resulting in noticeable facial distortion effects.
- Swelling or over-expansion of facial tissues can occur.
- Tears may happen in front of the ears and along the creases by the mouth and nose, as well as near the inner corners of the eyes.
- Fractures can occur in both the skull and the facial skeleton.
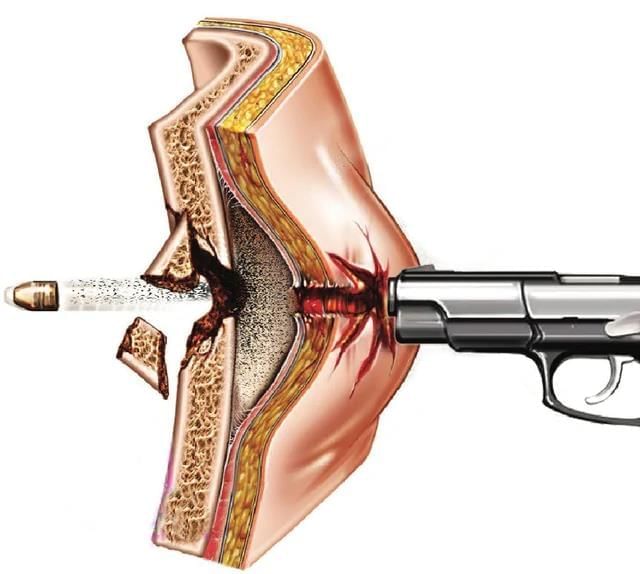 Mechanisms of blast effect
Mechanisms of blast effect
Medicolegal Significance
- Changes in the body can help pinpoint the wound of entry.
- However, the resulting disfigurement might make it harder to identify the deceased.
Cherry Red Discoloration
- When gunpowder burns, it produces carbon monoxide gas, which is typically observed in the tissues around and beneath the wound of entry.
- Carbon monoxide can attach to hemoglobin and myoglobin in blood and muscle tissues, forming carboxyhemoglobin and carboxymyoglobin, which have a cherry red color.
- This reaction causes a cherry red appearance in the muscles surrounding the wound of entry.
- This change can be helpful in identifying the wound of entry and determining the range of firing.
Abrasion and Grease Collar
- Abrasion and grease collars are caused by the gyroscopic movement of the bullet, the skin's elasticity, and the presence of grease and dirt particles on the bullet's surface. These collars can be seen on the skin surrounding the entry wound at different ranges.
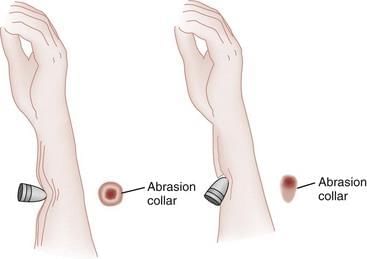 Abrasion collar in a bullet entry wound
Abrasion collar in a bullet entry wound
- Mechanism: When a bullet strikes and penetrates the skin, its spinning action creates friction, leading to the formation of an abrasion collar around the entry point. As the garment or skin flexes with the bullet's movement, it gets perforated. The bullet also removes dirt or grease particles from its surface, which are then deposited around the entry wound, creating the grease collar. These warm particles are readily absorbed by the skin.
- Appearance:
- Abrasion collar: This appears as a marginal abrasion around the entry wound. Its shape depends on the bullet's entry angle:
- Perpendicular entry results in a rounded abrasion collar.
- Acute angular entry leads to an oblique or oval abrasion collar.
- Grease collar: Often found on clothing, it appears as a sharply defined black mark, similar to a print. This is more noticeable on light-coloured fabrics and fair-skinned individuals.
- Abrasion collar: This appears as a marginal abrasion around the entry wound. Its shape depends on the bullet's entry angle:
- Medicolegal importance: The presence of abrasion and grease collars is valuable for determining the wound's entry and the direction of firing.
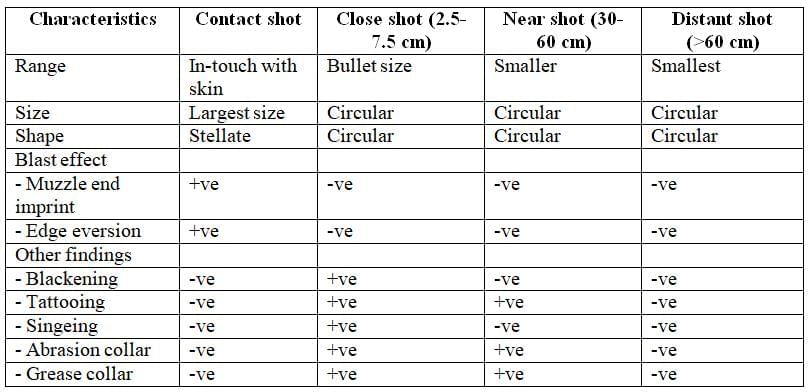
Wound of Entry
The wound of entry varies depending on the range of firing. For rifle firearms, four ranges are observed:
- Contact shot range
- Close shot range
- Near shot range
- Distant shot range
Contact Shot Range
- In the contact shot range, the muzzle of the firearm is in direct contact with the skin.
- Size: The wound is the largest among the four ranges.
- Shape: The wound can be crater-shaped or stellate (star-like).
- Blast Effects: Two main effects are observed:
- Muzzle end imprint abrasion, where the muzzle leaves an imprint on the skin.
- Eversion of wound edges, where the edges of the wound are turned outward.
- Blackening: Blackening is usually absent on the outer surface of the wound but may occur in deeper layers.
- Tattooing: Tattooing is generally not seen on the outside of the wound but may be present in deeper tissues.
- Cooking and Cherry Red Discoloration: The tissue inside the wound shows signs of cooking and/or cherry red discoloration.
- Singeing and Scorching: These effects are absent in the contact shot range.
- Abrasion Collar: An abrasion collar is not present.
- Grease Collar: Grease collar is also absent.
Close Shot Range
- The muzzle of the gun is positioned about 1 inch to 3 inches (approximately 2.5 to 7.5 cm. away from the target.
- The characteristics of the wound are depicted.
- Size: The wound is smaller than that of a contact shot.
- Shape: The wound is circular or oval in shape.
- Blackening: Blackening is usually observed around the wound with limited spread.
- Tattooing: Tattooing is typically seen around the wound but covers a smaller area.
- Singeing and/or Scorching: These are present around the wound.
- Abrasion Collar: An abrasion collar is present.
- Grease Collar: Grease collar is also present.
Near Shot Range
- The muzzle of the gun was positioned approximately 12" to 24" (30-60 cm) away from the target.
- The wound appearance is characterized by the features outlined below.
- Size: Smaller than a bullet.
- Shape: Circular or oval.
- Blackening: Typically observed around the wound with a large spread area, reaching a maximum of 30 cm.
- Tattooing: Usually present around the wound with a significant spread area, up to a maximum of 60 cm.
- Singeing: Absent.
- Abrasion Collar: Present.
- Edges: Generally inverted, although they can also be everted. In cases where the injury site contains a lot of adipose tissue, the edges of the wound may become everted.
Distant Shot Range
- In this scenario, the muzzle end of the gun is positioned more than 24 inches (60 centimeters) away from the target. The resulting wound appears similar to that of a near shot wound.
- Size: The wound is smaller than a near shot wound.
- Shape: The wound is circular in shape.
- Blackening: There is no blackening present on either the outer or inner sides of the wound.
- Tattooing: Tattooing is absent on both the outer and inner sides of the wound. However, it may appear around the entry wound at varying distances.
- Edges: The edges of the wound are inverted.
Exit Wound
- Exit wounds are analyzed based on their site, size, shape, and other characteristics.
- Site: The exit wound is located directly opposite the entry wound on the body.
- Size: The size of the exit wound can vary based on several factors:
- Close Range: Exit wounds are typically smaller than entry wounds at close range.
- Increased Range: As the distance increases, exit wounds tend to become larger.
- High Velocity Bullets: The size of exit wounds can vary significantly with high-velocity bullets, depending on how the bullet deforms upon impact.
- Deformed Bullets: If a bullet is deformed, it is likely to cause a larger exit wound.
- Shape: Exit wounds are usually irregular in shape but are roughly circular.
Other Findings
- Edges: The edges of the wound may appear puckered, torn, or everted.
- Some fat and other soft tissue might be present around the wound.
Peculiar Effects of Rifled Firearms/ Gunshot Wounds
Gunshot wounds caused by rifled firearms are typically straightforward. However, there are instances where they exhibit unusual characteristics. Below are some examples of atypical entrance wounds and their explanations.
Examples of Atypical Entrance Wounds
- Large Atypical Entrance Wound: An entrance wound that is unusually large for a gunshot injury.
- Bullet Bruise: Bruise caused by a bullet impacting the skin without penetrating it.
- Bullet Graze/Slap: Wound caused by a bullet grazing or slapping against the skin, creating a superficial injury.
- Ricochet Bullet: Bullet that strikes a surface and bounces off, causing an atypical wound pattern.
- Single Entry Wound with Multiple Exit Wounds: Scenario where one bullet enters the body but creates multiple exit wounds.
- Multiple Entry and Exit Wounds with a Single Bullet Recovered: Cases where multiple wounds are present, but only one bullet is recovered.
- Entry Wound Present, but No Bullet or Exit Wound: Situation where an entry wound is visible, but no bullet or exit wound can be found.
- Gutter Fracture of the Skull: Specific type of skull fracture caused by a bullet, resembling a gutter.
- Tandem/Piggy Back Bullet Effect: When two bullets hit in close succession, creating a unique wound pattern.
- Frangible Bullet Effect: Wounds caused by bullets designed to fragment upon impact, creating multiple wound channels.
- 'Dumdum' Bullet Effect: Refers to expanding bullets that cause larger wounds, though their use can be controversial in legal contexts.
- Artifacts: Unusual findings at a crime scene that may mislead investigations.
- Rayalaseema Phenomena: Specific phenomenon observed in certain gunshot cases in the Rayalaseema region.
- Souvenir Bullet: Bullet that is kept as a memento, often with an interesting backstory.
- Magic Bullet: Bullet that appears to have caused multiple wounds or injuries in a way that seems improbable.
- Concealed Firearm Wounds: Wounds caused by firearms that are concealed, leading to unique injury patterns.
Large Atypical Entrance Wound
The entrance wound is usually biggest at close range. As the distance increases, the size of the wound gets smaller. An entrance wound is considered large and unusual if it is bigger than expected at any known range, including the range for a contact shot.
Wound of entry for rifled firearms at different ranges — Summary of details
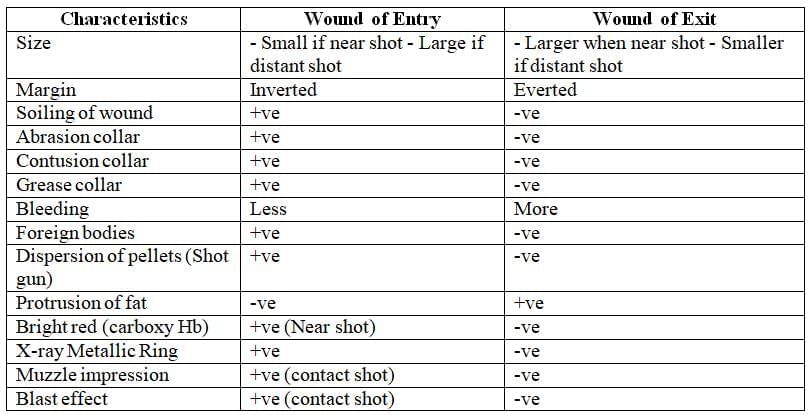
Difference between wound of entry and wound of exit
Causes—Probable causes are enumerated:
- Use of bullets of poor quality
- Wobbling of the tail of the bullet after leaving the muzzle end.
Mechanism
Both causes mentioned above could reduce the penetration power of the bullet, which therefore produces greater tissue damage at the wound of entry, making it unusually large irrespective of the range of firing.
Medicolegal importance
The medicolegal significance of this finding may complicate the assessment of firing range through examination of the entry wound.
Bullet Bruise
A bullet can hit the skin without going through it, causing a bruise at the impact point. This can happen even when wearing soft body armor because the armor stops the bullet but doesn’t prevent the blunt force impact, leading to bruise patterns.
Causes—Possible causes include:
- Use of unjacketed bullets
- Worn-out gun barrel
- Bullet size being smaller than the gun caliber
Mechanism: Any of these factors can decrease the bullet's speed, resulting in a loss of penetration capability. This makes the bullet behave like a blunt object that only causes bruising.
Appearance: The injury looks like a linear bruise, approximately the size of the bullet, showing the typical color changes seen with any bruise.
Medicolegal importance: It can be mistaken for injuries caused by other blunt objects. The color changes in the bruise can offer hints about the time elapsed since the injury occurred.
Bullet Graze (Bullet Slap)
- A bullet graze, also known as a bullet slap, occurs when a bullet strikes the skin at an angle and exits without fully penetrating. This can result in either an abrasion or a laceration, depending on the thickness of the skin.
- These superficial skin injuries can occur due to poor quality bullets or inaccurate aiming.
- The mechanism behind a bullet graze involves various factors that cause the bullet to merely touch the skin before moving away.
- The appearance of the injury may present as a scratch or a laceration, depending on the circumstances.
- From a medicolegal perspective, bullet grazes can be mistaken for injuries caused by blunt or, in some cases, sharp weapons.
Ricochet Bullets
- Ricochet bullets produce a distinctive effect at the entry wound because the bullet bounces off surfaces before entering.
- These bullets can cause irregular and enlarged entry wounds due to their deflected path.
 Peculiar effects of rifled firearm
Peculiar effects of rifled firearm
Causes of Ricochet Bullets
- Inferior Quality Firearms: Using a firearm that is of poor quality can lead to malfunction and improper bullet trajectory, increasing the chances of ricochet.
- Low-Velocity Bullets: Bullets with low velocity are more susceptible to losing gyroscopic stability and can deviate from their intended path, making ricochet more likely.
Appearance of Ricochet Bullet Wounds
- Size: The entry wound is typically large, regardless of the shooting range.
- Shape: The wound shape is often keyhole-like or elongated due to the bullet's deflected path.
- Edges: The edges of the wound are ragged, indicating trauma from a deforming bullet.
Examination of the Bullet
- Deformation: The bullet recovered from a ricochet may be deformed or flattened due to impact with a hard surface before penetrating the target.
- Debris: The bullet may carry paint, dirt, or other debris from the object it deflected off, indicating the surface it struck before entering the target.
Mechanism of Ricochet Bullets
- Ricochet bullets can lose their gyroscopic movement due to impact with a surface, causing a slight deviation in their path.
- The bullet may collide with another object, become deformed, and penetrate a victim or target that was not the intended aim.
- This unpredictable trajectory is what causes the unique entry wounds associated with ricochet bullets.
Examples of Intracranial Bullet Injuries
- Intracranial bullet injuries refer to cases where bullets that ricochet off the skull, known as ricochet bullet injuries. When a bullet enters the cranium, it can deflect off the inner surface of the skull, altering its trajectory and becoming lodged in an unexpected location.
- There are five potential ricochet mechanisms within the cranial cavity:
- Single ricochet the bullet bounces back only once.
- Double ricochet the bullet bounces back twice.
- Inner tangential of entrance side the bullet glides as it enters the skull at the entry point.
- Inner tangential at contralateral side when the bullet strikes the opposite side of the entry wound, it glides and travels a significant distance.
- Inner tangential at contralateral side and ricochet the bullet glides and then bounces in another direction.
- Medico-legal implications: Understanding these mechanisms is crucial for clarifying the bullet's trajectory in the deceased and determining the cause of death.
Single Entry and Multiple Exit Wounds
When a bullet enters a person's body, it can shatter into several pieces upon hitting bones. Each of these fragments can then exit the body separately, leading to multiple exit wounds.
Multiple Wounds of Entry and Exit, but a Single Bullet Recovered
The positioning of the victim can cause a bullet to enter and exit the body multiple times, resulting in several entry and exit wounds. For example:
- If a victim is sitting with their knees pulled up to their chest, the bullet may create wounds in different areas, such as the back, chest, and knees.
- It is essential to take these possibilities into account when reconstructing a shooting incident, particularly when multiple firearms are used and several bullets are fired.
Entry Wound Present, But No Exit Wound or Bullet Recovered
- Explanation. When a bullet enters the body, it can travel through natural passages and may be lost through coughing, vomiting, or by passing through the anus. If the bullet gets lodged in the bones, it might not be retrievable.
- The bullet can also enter a large blood vessel and travel to a distant location, becoming a bullet embolus.
- An X-ray survey is typically performed in shooting deaths to locate the bullet, and this should be done before any internal examination of the body.
Gutter Fracture
Gutter fracture is a type of skull fracture that can occur due to the impact of a bullet. In this case, the entry wound shows multiple bullets lined up one after the other. This phenomenon is particularly relevant when a firearm is not well-maintained or is malfunctioning. If a firearm is fired without proper cleaning, there is a possibility that a bullet fired previously may not have been expelled from the barrel and instead stayed inside. When the firearm is discharged again, both bullets might enter the entry wound simultaneously.
Tandem (Piggy Back) Bullet Effect
- Entry wound present, but no exit wound or bullet found.
- Possible paths the bullet could have taken out and lost.
- Bullet lodged in the bone.
Frangible Bullet Effect
- A frangible bullet is designed to break apart into multiple pieces when it enters the body, leading to severe injuries.
- Upon striking a solid surface such as a steel plate or backstop, the bullet shatters completely into tiny fragments.
Dum-Dum Bullet Effect
- The dum-dum bullet effect refers to specific modifications that enhance the bullet's lethality.
- The term "dum-dum" originates from a town in India where these types of bullets were first utilized.
- A dum-dum bullet features a specialized mechanism at its tip that expands upon impact, splitting into several fragments.
- Each fragment is capable of causing severe injury over a larger area, making the bullet more dangerous.
Rayalaseema Phenomenon
- Origin: The term "Rayalaseema Phenomenon" comes from a specific incident that occurred in the Rayalaseema district of Andhra Pradesh, India.
- Description: This phenomenon refers to a particular type of crime scene manipulation. In this case, a victim who was originally killed by a stab wound was further tampered with by the criminal. To mislead investigators, the criminal filled the stab wound with a bullet.
- Discovery: The deception was only uncovered after a detailed autopsy was conducted. The careful examination revealed the incongruity of the bullet being placed in the stab wound, which helped in understanding the true sequence of events.
Souvenir Bullet
- Definition: Souvenir bullet refers to a bullet that has been lodged in the body for an extended period, typically ranging from 25 to 30 years or more.
- Surrounding Tissue: Over time, a dense fibrous tissue capsule often forms around the bullet, encapsulating it within the body.
- Entry Wound: The original entry wound where the bullet entered the body is usually marked by a small scar, indicating the point of entry.
- Lack of Fresh Bleeding: One of the key indicators that the bullet has been in the body for a long time is the absence of fresh bleeding in the surrounding area.
- Bullet Path: It becomes difficult to trace the bullet's path from the entry wound to its current location, further confirming its long-term presence in the body.
- Historical Bullets: Bullets from the two World Wars are often discovered during CT scans conducted for various medical conditions, highlighting their long-term presence in the body.
- Lead Poisoning Risk: Although rare, lead poisoning can occur from a lead bullet lodged in the body for a long time. This risk is higher when there is a rich blood supply in the tissue surrounding the bullet or prolonged contact with synovial fluid.
The Magic Bullet Theory
The term "magic bullet theory" refers to a controversial explanation put forth by the Warren Commission regarding the assassination of President John F. Kennedy. The theory suggests that a single bullet, known as "Warren Commission Exhibit 399" (CE399), caused multiple non-fatal injuries to both President Kennedy and Texas Governor John Connally during the shooting.
Details of the Theory
- The theory, primarily attributed to Arlen Specter, a member of the Warren Commission, argues that one bullet was responsible for several injuries to both Kennedy and Connally, while a different bullet caused Kennedy's fatal head wound.
According to the theory:
- A 6.5 millimetre rifle bullet was fired from the sixth floor of the Texas School Book Depository.
- The bullet passed through Kennedy's neck, Connally's chest and wrist, and ended up in Connally's thigh.
The bullet's path included:
- Penetrating 15 layers of clothing, 7 layers of skin, and approximately 15 inches of tissue.
- Striking a tie knot, removing 4 inches of rib, and shattering a radius bone.
Discovery of the Bullet
- The bullet believed to have caused these injuries was found on Governor Connally's stretcher at Parkland Memorial Hospital in Dallas.
- It became a key piece of evidence, known as CE399, with an intact copper jacket and a compressed tail.
Commission Findings
- The Warren Commission concluded that there was strong evidence supporting the idea that a single bullet caused Kennedy's neck wound and all of Connally's injuries.
- While there were differing opinions among Commission members about the theory's likelihood, they agreed it was not crucial to their overall findings.
- All members were certain that all shots were fired from the sixth-floor window of the Depository building.
Later Support and Criticism
- In 1978, the House of Representatives' Select Committee on Assassinations endorsed the Single Bullet Theory but disagreed on the timing of the shots.
- The theory has been strongly defended by supporters of the Warren Commission's conclusions but heavily criticized by its opponents.
Concealed Firearm Wound
In some cases, a large blood clot can form over the entry wound due to significant bleeding, concealing it until the clot is removed. Therefore, it is essential to carefully identify the actual bleeding site in all instances where blood loss appears to be the cause of death.
Shotgun Wounds
Shotgun wounds are injuries caused by shotguns or smooth-bore firearms. Shotguns are widely used, and there are more of these guns than rifled ones. As gunshot wounds become more common, it is important for trauma specialists to understand the characteristics of shotgun wounds. The severity of shotgun wounds can vary greatly because the pellets spread out as they travel. Like other gunshot wounds, different aspects of shotgun injuries are best examined in the following sections:
- General considerations of shotgun wounds
General Considerations of Shotgun Wounds
When a shotgun is fired, it discharges a variety of components, including:
- Gunfire
- Gun smoke, which contains soot and gunpowder particles
- Card wads
- Wads
- Gases
- Lead shot
Each of these components can impact the resulting wound in different ways. Understanding the range at which each component can travel is crucial.
While the effects of shotgun wounds are similar to those from rifled firearms, there are significant differences in the entry and exit wounds.
Wound of Entry
- Range or Distance of Firing: The appearance of wounds varies based on the distance from which the shotgun is fired.
- Size of Pellets: The size of the pellets used in the shotgun can significantly impact the size of the wounds produced. Smaller pellets result in smaller wounds, while larger pellets create larger wounds.
- Types of Gunpowder: The type of gunpowder used in the shotgun also affects the wound appearance. Smokeless gunpowder does not produce a soiling effect on the wound, whereas black gunpowder creates a noticeable soiling effect.
Entry Wounds at Varying Distances
- Up to 90 cm: When pellets stay together, they create a single entry wound.
- Beyond 90 cm: Pellets spread out and act like individual projectiles, causing multiple smaller wounds in a specific area.
Distance travelled by components of the shotgun firing discharges with the specific effects produced by them
Entry wounds caused by a shotgun (smooth bore firearm) at various ranges - Summary of Details
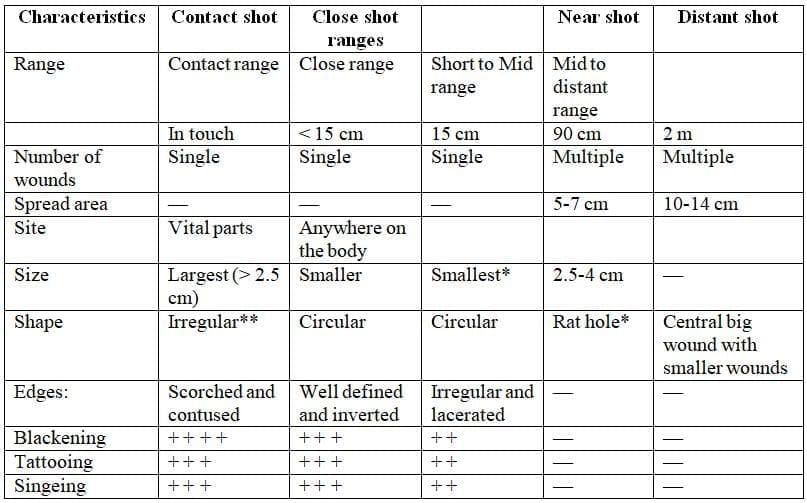
- Both are called as close range ** Irregularly circular with crenated and scalloped edges
Notes:
- Close-range shotgun wounds can be as destructive as those from a high-velocity rifle; however, longer the weapon-victim range-injury produced is minimal.
- The type of shot (size and weight of pellets) used also determines the type of injury; usually more serious injuries are produced by the larger type of buckshot (greater than 0.14 inches in diameter).
Blowback Effect
The effects of a contact or close-range shotgun wound can resemble a blast injury. The primary mechanism involves gases produced during firing accumulating beneath the skin, leading to:
- A larger entry wound
- Muzzle imprint abrasion
- Facial distortion if the muzzle is pressed against the roof of the mouth
Billiard Ball Ricochet Effect
This phenomenon occurs when a close-range shot appears to produce an entry wound similar to one from a longer range (beyond 90 cm). For example, this can happen when a shot passes through an intermediate barrier, such as a wooden partition or window, before hitting the victim.
Explanation: When pellets, tightly grouped at close range, strike an intermediate target (e.g., a wooden partition), the leading pellets slow down upon impact. Subsequent pellets collide with them, causing the pellets to scatter or rebound in a wider pattern, similar to billiard balls struck by a cue ball. This results in a broader spread of wounds on the victim (the secondary target), mimicking the appearance of a shot fired from a greater distance.
This effect diminishes at longer ranges because the pellets are already widely dispersed.
Medicolegal Significance: The billiard ball ricochet effect complicates the estimation of the firing range, as the wound pattern may not accurately reflect the actual distance from which the shot was fired.
Autopsy of John F. Kennedy
- John F. Kennedy, the 35th President of the United States, served from 1961 until his assassination in 1963.
- Born on May 29, 1917, in Brookline, Massachusetts, Kennedy was tragically shot and killed on November 22, 1963, in Dallas, Texas.
- He was married to Jacqueline Lee Bouvier Kennedy at the time of his death.
- The autopsy for President Kennedy began on the evening of November 22, 1963, at around 8 p.m. Eastern Standard Time, and was completed by midnight the same night.
- This examination took place at Bethesda Naval Hospital, located in Bethesda, Maryland.
- The decision to conduct the autopsy at this specific hospital was made at the request of Mrs. Kennedy, reflecting her husband's service as a naval officer during World War II.
Previous Testimony from Dallas Doctors
The Back Wound
- The death certificate, signed by Dr. Burkley, the President's personal physician and a U.S. Navy Admiral, indicated a wound location on President Kennedy that was lower than what was later determined in the autopsy.
- Dr. Burkley estimated that a bullet hit Kennedy at "about" the level of the third thoracic vertebra (T3).
- A diagram from the autopsy report appears to support Dr. Burkley's assessment, showing a bullet hole in Kennedy's upper back; however, the accuracy of this diagram is disputed.
- The diagram is criticized for lacking precision and not specifying anatomical landmarks, a point raised in the later analysis by the House Select Committee on Assassinations (HSCA).
- Dr. Burkley's indicated location at T3 corresponds with the bullet hole found in Kennedy's shirt and suit jacket, which are located about 5 to 6 inches below the top of his collar.
- There is, however, debate about whether the holes in the clothing should align with the location of the back wound, considering that Kennedy was sitting with a raised arm during the assassination.
- Numerous photographs from the motorcade show Kennedy's suit jacket bunched at the back of his neck and shoulder, which would have prevented it from lying closely against his skin.
Official Findings of the Autopsy
The missile wound in the back
- The Bethesda autopsy team attempted to investigate the bullet hole in Kennedy's neck above the scapula, but they were unable to do so because it had passed through the neck strap muscle. They did not carry out a thorough examination or continue tracing it, as they were unaware of the exit wound at the front of the throat, which had been removed by emergency room doctors during the tracheostomy.
- The autopsy report, known as Warren Exhibit CE 386, described the back wound as oval, measuring 6 × 4 mm, and located “above the upper border of the scapula” at a distance of 14 cm (5.5 in) from the tip of the right acromion process and 14 cm (5.5 in) below the right mastoid process (the bony area behind the ear).
- The final page of the Bethesda autopsy report states: “The other missile [the bullet to the back] entered the right superior posterior thorax above the scapula and went through the soft tissues at the base of the right side of the neck.
- The report also mentioned a bruise on the apex (top) of the right lung where it rises above the clavicle. It noted that although the apex and the membrane covering it were bruised, they were not penetrated, indicating that the missile passed close to them but did not enter. The thoracic cavity was not penetrated.
- This missile caused bruises to the right pleura and the upper lobe of the right lung. It damaged the strap muscles on the right side of the neck, affected the trachea, and exited through the front of the neck.
- The single bullet theory from the Warren Commission Report places a bullet wound at the sixth cervical vertebra, consistent with the 5.5 inches (14 cm) below the ear. While the Warren Report discusses the wound locations, it does not definitively conclude on the bullet entry at this vertebra. However, a 1979 report by the House Select Committee on Assassinations (HSCA) noted a defect in the C6 vertebra on the Bethesda X-rays that the autopsy team missed.
- Even without this additional information, the original Bethesda autopsy report included in the Warren Commission report concluded that the bullet passed completely through the president's neck, starting above the scapula and lung (and the pleura over the lung) and exiting through the lower throat.
- Claims that commission members “moved the wound” require further investigation, as Gerald Ford admitted to renaming the wound's location “to make things clearer.” The Bethesda autopsy only noted that JFK was hit in the upper thorax above the scapula (the soft area at the top of the shoulder), and Ford changed this to “the base of the neck.”
- The Commission report, amended by Ford, then stated that the bullet passed through the base of the neck instead of the back. However, Ford’s change aligns with a bullet hit in the shoulder at the C6 vertebral body, where the HSCA and photographs placed the wound based on X-ray damage and tiny lead fragments found there. The neck formally begins (and the thorax ends) at the level of C7, the first cervical vertebral body above the thorax; thus, the original autopsy report is technically incorrect.
Details of the Missile Wound to the Head
- The autopsy conducted at Bethesda describes the wound at the back of President Kennedy's head as a laceration measuring approximately 15 × 6 mm. This wound is located to the right and slightly above the external occipital protuberance.
- Beneath this laceration, there is a corresponding wound in the skull bone, which exhibits beveling. Beveling refers to a cone-shaped widening of the bone margins when viewed from inside the skull.
- Additionally, there is a large and irregular defect on the right side of the head, primarily affecting the parietal bone, but also extending into the temporal and occipital regions. This defect measures about 13 cm (5 inches) in width at its largest point.
- During the examination, three fragments of skull bone were received as separate specimens, and their sizes roughly correspond to that of the large defect.
- The largest fragment includes part of the perimeter of a roughly circular exit wound, which displays beveling on the outer side of the bone. This exit wound measures approximately 2.5 to 3.0 cm in diameter.
- X-ray imaging revealed the presence of tiny metal particles in the bone at the margin of this exit wound.
- Furthermore, small pieces of the projectile were identified by X-ray along the trajectory from the rear wound to the defect in the parietal area of the skull.
Subsequent Government Investigations
Ramsey Clark Panel Analysis (1968)
In 1968, at the request of Attorney General Ramsey Clark, a panel of four physicians was convened in Washington, DC, to reexamine the autopsy of President Kennedy. The panel reviewed a wide range of materials, including:
- Original autopsy records
- Photographs and X-rays
- Clothing
- Films and motion pictures
- Bullet fragments
The panel also considered the Warren Commission report and arrived at several key conclusions:
- Evidence from clothing, photographs, and X-rays indicated that President Kennedy was struck by two bullets from above and behind.
- One bullet passed through the right side of the neck without hitting any bone.
- The second bullet entered the skull from behind, causing an explosive injury on the right side of the head.
The panel's findings aligned with parts of the original Autopsy Report and the Warren Commission's medical assessments. However, there were notable differences and confirmations regarding the Bethesda autopsy and the Warren Report:
- The Clark report positioned the head wound 100 mm (4 inches) higher than described in the Bethesda report, supporting the idea of a high-angle rear entry wound to the skull.
- The report placed the back wound in the neck, above the scapula, indicating it passed through the throat and over the top of the right lung. This finding was consistent with Bethesda's conclusions and was further validated by the presence of metallic fragments along the bullet's path.
Analysis by the Rockefeller Commission (1975)
- The Rockefeller Commission, consisting of five members, investigated the President’s body movements in relation to the head injury that caused his death.
- The Commission examined various materials, including:
- films
- autopsy reports
- photographs
- President Kennedy’s clothing
- back brace
- bullet fragments recovered
- the 1964 Warren Commission report
- After reviewing all the evidence, the panel unanimously concluded that President Kennedy was struck by only two bullets, both fired from behind. One bullet hit the back of his head.
- Three of the physicians observed that the backward and leftward movement of the President’s upper body following the head shot was a strong reaction, causing the body to stiffen due to severe brain damage.
HSCA Analysis (1979)
The United States House of Representatives Select Committee on Assassinations (HSCA) established a forensic panel to review original autopsy photographs and X-rays of President John F. Kennedy and to interview autopsy personnel to verify their authenticity. The panel addressed two key questions:
- Could the photographs and X-rays in the National Archives be confirmed as those of President Kennedy?
- Was there any evidence of alteration in these materials?
Verification of Authenticity:
- Forensic Anthropology Analysis: Experts compared autopsy photographs with pre-death images of President Kennedy, using both metric and morphological features. They also examined autopsy X-rays alongside pre-death X-rays, identifying sufficient unique anatomical characteristics to confirm that the autopsy X-rays were of Kennedy.
- Forensic Dentistry Analysis: The President’s dental records were compared with X-rays from the autopsy that included his teeth, further confirming the materials were of Kennedy.
- Photographic and Radiologic Examination: Photographic scientists and radiologists analyzed the original autopsy photographs, negatives, transparencies, and X-rays, concluding there was no evidence of alteration.
Based on these findings, the HSCA deemed the autopsy materials authentic and reliable for the forensic pathology panel’s conclusions.
Medical-Forensic Conclusions: The HSCA concluded that President Kennedy was struck by two rifle shots, both fired from behind:
- One bullet entered the upper right back and exited through the front of the throat.
- A second bullet entered the right rear of the head near the cowlick area and exited from the right side of the head, causing a massive wound.
Addressing Inconsistencies with Head Movement: The backward motion of Kennedy’s head in the Zapruder film appeared inconsistent with bullets entering from behind. A wound ballistics expert was consulted, who suggested that nerve damage from the head shot could have caused the back muscles to contract, resulting in the head moving backward. This was demonstrated in a filmed experiment involving goats.
Criticisms of the Original Autopsy: The HSCA identified several issues with the Bethesda autopsy and evidence handling:
- The location of the head entry wound was inaccurately described.
- The autopsy report was incomplete, lacked reference to photographs, and contained inaccuracies, particularly regarding the back entry wound.
- Entry and exit wounds on the back and front neck were not described relative to fixed anatomical landmarks or to each other.
Medicolegal Implications: These inconsistencies caused confusion and necessitated further investigation and expert analysis of the autopsy materials. Despite resolving the direction of firing and cause of Kennedy’s death, the case contributed to forensic literature concepts such as the “Kennedy Phenomenon,” the “Single Bullet Theory,” and the “Souvenir Bullet,” which remain significant in forensic discussions.
Estimating Firing Range from Entry Wound Analysis
By examining the entry wound (and any clothing worn), a rough estimate of the firing range can be determined.
Principle: The spread of pellets increases consistently as the firing range increases.
For a non-choked (cylindrical barrel) shotgun:
- Ranges up to 3 meters: The spread area diameter (in cm) can be estimated by multiplying the range (in meters) by 3.5.
- Formula: Range (r) × 3.5 = Spread area diameter (A)
- To find the range: Range (r) = Spread area (A) ÷ 3.5 = A × 2/7 meters
- Ranges beyond 3 meters: The spread area is approximately 25 cm per meter of range. Examples:
- Spread area of 25 cm = Firing range of 1 meter
- Spread area of 50 cm = Firing range of 2 meters
- Spread area of 75 cm = Firing range of 3 meters, and so on.
Exit Wound Characteristics: Exit wounds occur when pellets pass completely through the body. They typically show:
- Everted (outward-turned) margins
- No signs of soiling, singeing, or burning
- Possible multiple exit wounds, as individual pellets or groups may exit separately
Exceptions: Shotgun pellets usually do not exit the body, except in cases of:
- Contact shots
- Tangential wounds with a short path through the body
- Thin body parts (e.g., neck or extremities)
|
73 docs|3 tests
|
FAQs on Firearms and Explosive Injuries - 3 Chapter Notes - Forensic Medicine and Toxicology (FMT) - NEET PG
| 1. What are the peculiar effects of gunshot wounds caused by rifled firearms? |  |
| 2. How do shotgun wounds differ from those caused by rifled firearms? | |
| 3. What is a gutter fracture and how is it related to gunshot wounds? | |
| 4. What factors influence the severity of injury from gunshot wounds? | |
| 5. What are the common medical treatments for gunshot wounds? | |


Firearms and Explosive Injuries - 3 Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,Extra Questions
,Exam
,Summary
,video lectures
,Viva Questions
,shortcuts and tricks
,Objective type Questions
,study material
,Free
,Firearms and Explosive Injuries - 3 Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,Firearms and Explosive Injuries - 3 Chapter Notes | Forensic Medicine and Toxicology (FMT) - NEET PG
,practice quizzes
,Semester Notes
,mock tests for examination
,Previous Year Questions with Solutions
,ppt
,past year papers
,Important questions
,MCQs
,Sample Paper
;


Chapter Notes: Firearms and Explosive Injuries - 3 Free PDF Download
Importance of Chapter Notes: Firearms and Explosive Injuries - 3
Chapter Notes: Firearms and Explosive Injuries - 3
Chapter Notes: Firearms and Explosive Injuries - 3 NEET PG Questions
Study Chapter Notes: Firearms and Explosive Injuries - 3 on the App
|
© EduRev
|
Education Revolution
|



|





