Mechanism: Urine Formation | Biology for JAMB PDF Download

Mechanism of Urine Formation
The mechanism of urine formation involves three steps or processes :
(I) Ultrafiltration or Glomerular filtration
(II) Selective tubular reabsorption
(III) Tubular secretion
(I) Ultrafiltration or Glomerular Filtration
This process occurs in the Malpighian corpuscles of the nephrons. The glomerulus of a Malpighian corpuscle is a network of several (about fifty in man) parallel capillaries. From the blood flowing through glomerular capillaries, about 20% of plasma fluid filters out into the Bowman's capsule through a thin glomerular-capsular membrane due to a net or effective filtration pressure (EFP) of about 10 to 25 mm Hg.
The glomerular-capsular membrane through which ultrafiltration occurs comprises three layers, viz
(1) endothelium
(2) basement membrane of the wall of glomerular capillaries and
(3) squamous epithelial layer of the finger-like processes('foot processes' or pedicels) of podocyte cells of capsular wall entwining the walls of capillaries. A special characteristic of glomerular-capsular membrane is that it is about 100 to 500 times more permeable than the walls of blood capillaries in other tissues of body. Such a tremendous permeability of this membrane is because of the presence of literally thousands of small pores, called fenestrae, in the walls of glomerular capillaries (fenestrated capillaries).
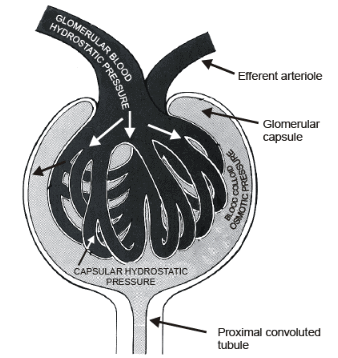
The effective filtration pressure that causes ultrafiltration is determined by three pressures :
(1) glomerular hydrostatic pressure,
(2) colloid osmotic pressure of blood and
(3) capsular hydrostatic pressure.
The glomerular hydrostatic pressure is the blood pressure in glomerular capillaries. It is the chief determinant of effective filtration pressure, i.e. the main driving force to cause filtration. (it is 60 to 75 mm Hg) The colloid osmotic pressure is the osmotic pressure created in the blood of glomerular capillaries due to plasma proteins. It resists the filtration of fluid from the capillaries. (it is 30 to 32 mm Hg) The capsular hydrostatic pressure is the pressure caused by fluid (filtrate) that reaches into Bowman's capsule and resists filtration. (It is about 10 to 18 mm Hg) Normally, the blood pressure in an arteriole that feeds a typical systemic capillary network is about 35 to 40 mm Hg. The pressure in afferent arteriole of glomerulus is about 60 to 75 mm Hg and since the efferent arteriole is thinner in diameter than afferent arteriole, this blood pressure (glomerular hydrostatic pressure) is maintained throughout the glomerulus. The colloid osmotic and capsular hydrostatic pressures, which resist ultrafiltration, are respectively about 30 to 32 mm and 10 to 18 mm Hg. Thus, the net effective filtration pressure is about 10 i.e. (60) – (32 + 18) mm Hg. That is why, the glomerulus is a 'high pressure capillary bed'.
EFP = GHP – [COP + CHP]
∴ EFP ranges from 10 to 25 mm Hg.
 The plasma fluid that filters out from glomerular capillaries into Bowman's capsules of nephrons is called glomerular filtrate.
The plasma fluid that filters out from glomerular capillaries into Bowman's capsules of nephrons is called glomerular filtrate.
The quantity of glomerular filtrate, formed each minute in all the nephrons of both kidneys is called Glomerular filtration rate (GFR). In a normal adult human being, a glomerular filtration pressure of 1 mm Hg causes filtration of about 12.5 mL of plasma fluid from glomerular capillaries per minute. Thus the GFR in a normal adult person is 125 (12.5 × 10) mL of plasma fluid per minute. As already described in the chapter of circulatory system, an average adult person of about 70 kg possesses about five litres of blood all of which is pumped by the heart (cardiac output) into the arteries and received back through veins each minute. About 1250 mL (25% of total blood) of this blood circulated through kidneys each minute, and of this blood, about 650 mL is the blood plasma(52%). This 650 mL is called renal plasma flow (RPF). Obviously, 125/650 i.e. about one-fifth (20%) of the blood plasma, therefore, filters out into kidneys nephrons per minute. This is the ratio of GFR to RPF, and it is called filtration fraction.
With a glomerular filtration rate (GFR) of 125 mL per minute, about 180 litres of plasma fluid from about 1800 litres of blood circulating through both kidneys of an average person each day filters out into kidney nephrons.
But only about 1.45 litres (about 0.8% part) of the total glomerular filtrate is excreted out as urine per day, the rest is reabsorbed into the blood from the nephrons.
Due to continuous beating of the cilia of neck cells, the glomerular filtrate is continously made to flow behind from Bowman's capsules into the proximal convoluted tubules of the nephrons.
(II) Selective Tubular Reabsorption
The glomerular filtrate is like blood plasma minus plasma proteins (colloids) in chemical composition. Thus, it is mostly water with all soluble and diffusible solutes of plasma which include nutrients (glucose, amino acids, etc), electrolytes of salts (Na+, K+,Cl–, HCO3–, H+, etc) and waste products of protein metabolism (urea, uric acid, creatinine, etc). In contrast to glomerular filtrate, the urine which is ultimately extracted from the filtrate in nephrons, contains water, urea, uric acid, creatinine and useless electrolytes in considerably higher concentrations, whereas nutrients are almost absent in it. This proves that, while the filtrate flows through a uriniferous tubule, not only its volume is reduced, but its composition is also considerably changed. These changes are obviously due to an exchange of materials between the filtrate and the blood of Peritubular capillaries.This exchange involves:
(1) A selective reabsorption of useful materials into the the blood from the filtrate and
(2) Absorption of remaining unfiltered amount of excretory substance from blood flowing in the peritubular capillaries, by the cells of uriniferous tubules and then subsequent secretion of these substances into the filtrate. This selective reabsorption and secretion are finely tuned to maintain homeostatic balances in body fluids.
The blood flows rapidly in peritubular capillaries and with a very low pressure (only about 13 mmHg). Due to this reason fluid can diffuse into these capillaries from surrounding tissue fluid, but cannot filter out of them. This reabsorption involves both active and passive processes.
(III) Tubular Secretion
In addition to its role in selective reabsorption of materials from the glomerular filtrate back into the blood of peritubular capillaries via the renal interstitium, the distal part of proximal convoluted tubule also alters the composition of filtrate by a process of secretion. Epithelial cells in this part extract certain excretory substances from the blood of peritubular capillaries and secrete these into the filtrate. For example, uric acid filtered by glomerulus is reabsorbed in the first part of proximal tubule, but is later withdrawn from blood and secreted into the filtrate in distal part of proximal tubule, Other secreted substances include H+, K+, NH4+, creatinine, etc and certain dyes and drugs, like phenol red, penicillin, hippuric acid and its derivatives, etc. Secretion of H+ helps in controlling blood pH.
|
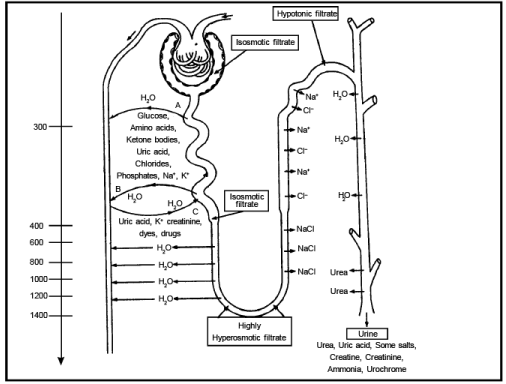
Changes occurring stepwise in the filtrate while it flows through the tubules :
(1) Bowman's Capsule : Since all plasma solutes, except proteins, freely enter into glomerular filtrate from blood, the total solute concentration (osmolality 300 milliosmoles per litre) of the filtrate is essentially the same as that of plasma. Here the filtrate is thus isotonic(isosmotic) to the plasma.
∴ Concentration 4 , Volume 4
(2) Proximal Convoluted Tubule : The microvilli of the "brush-border" columnar cells of the epithelium of this tubule increase the internal surface of the epithelium about 20 times. Hence, this epithelium becomes most suitable for reabsorption. About 65% to 80% of the filtrate is reabsorbed into the blood of peritubular capillaries through this epithelium and surrounding tissue fluid (renal interstitium). Most of the solutes like glucose, amino acids, vitamins, ketone bodies, acetoacetic acid, uric acid, chlorides, sodium, potassium, phosphates etc of the filtrate are reabsorbed into the blood by diffusion and active transport. Some urea is also reabsorbed. Sulphates, creatinine, inulin and PAH (para aminohippuric acid) are not reabsorbed.
As most of the solutes are reabsorbed, water automatically goes back into the blood by osmosis leaving the osmotic pressure in the filtrate unchanged. Thus, the filtrate is reduced in volume, but it still remains isotonic to the plasma
∴ Concentration 4 , Volume 
(3) Descending Limb of Henle's Loop : The loop of Henle is divisible into four parts, namely Thick descending limb, the Thin descending limb, the Thin segment of ascending limb, and the Thick segment of ascending limb.
In mammalian kidneys, the osmolality of renal interstitium is different in renal cortex and medulla.
Whereas the cortical interstitium has the normal osmolality of 300 mL osmol/liter, the medullary interstitium has a gradient of increasing osmolality from the cortex upto the tips of the papillae. (300 to 1400 mL osmol/liter) The thin wall of descending limb of Henle's loop is permeable to water, but not to the solutes. As the isotonic tubular fluid flows down this limb, it gradually loses water by exosmosis due to increasing osmolality of medullary interstitium through which this limb extends. This leaves a small volume of concentrated (hypertonic to blood plasma) tubular fluid to enter into the ascending limb of Henle's loop.
∴ Concentration  , Volume
, Volume
(4) Ascending Limb of Henles Loop : The thin segment of the ascending limb of henle's loop is structurally like the descending limb, but its permeability is different. It is quite permeable to NaCl but not to water.
Due to decreasing osmolality of medullary interstitium towards cortex, the tubular fluid, therefore, loses Na+ and Cl– by diffusion, again becoming diluted and isotonic to plasma without changing in volume.
∴ Concentration , Volume 4
The wall of the thick ascending limb of Henle's loop is virtually impermeable to both water and solutes, but the plasma membrane of its cells is very rich in Na+ –K+ pumps. These pumps pump out Na+ by active transport, and Cl– passively diffuse out following the outflux of Na+. Thus the process of dilution of the tubular fluid continues in this limb. Consequently, the tubular fluid becomes considerably hypotonic to blood plasma without a change in its volume.
∴ Concentration , Volume 4
(5) Distal Convoluted Tubule (DCT) : In the distal convoluted tubule,active reabsorption of Na+ and that of Cl– continues by facilitated diffusion and hence the tubular fluid becomes still more diluted. It also helps to regulate blood pH by reabsorption of HCO3– which is an important buffer.
∴ In proximal DCT Concentration , Volume 4
(6) Collecting Duct : From the distal convoluted tubule, the hypotonic tubular fluid flows into a collecting duct. This duct is quite permeable to water but not to salt (in presence of some ADH). Hence the tubular fluid loses considerable amount of water by exosmosis as the duct runs down through the hypertonic medullary interstitium to empty into the calyx. The distal part of collecting duct is permeable to urea also. Hence same urea is also reabsorbed from tubular fluid and it adds to the hyperosmolality of medullary interstitium.
∴ Concentration , Volume
After losing considerable amount of water and some urea, while flowing through the collecting ducts, the filtrate ultimately becomes urine.
Chemical Composition and Physical Characteristics of Urine
Normal urine contains about 95% water, 2% electrolytes (ions of salts, mainly chlorides, sulphates, phosphates and bicarbonates of sodium, potassium, ammonium, etc), 2.6% urea, 0.3% uric acid and traces of creatinine, ammonia, creatine etc. It is transparent but pale yellow due to the presence of a trace of urochrome pigment. Urochrome is a byproduct of hemoglobin degradation found in blood and filtered into glomerular filtrate Normal urine is slightly acidic with a pH of 6.00 (range is 4.5 to 8.2). Its specific gravity is 1.015 to 1.02. On standing, it becomes cloudy and acquires ammonia odour due to formation of ammonium carbonate.Osmoregulation by Kidneys
Kidneys also perform the important function of osmoregulation (regulation of osmolality) by regulating the amount of water in body fluids. The normally functioning kidneys produce a large volume of dilute urine when more water is taken, and a small volume of concentrated urine when water intake by the body is poor or there is considerable loss of water from the body. This function of kidneys is regulated by the antidiuretic hormone (ADH or Vasopressin) secreted by the posterior lobe of pituitary gland. This hormone increases the water permeability of the last part of distal convoluted tubules and proximal part of the collecting ducts. In absence of ADH, these parts are almost impermeable to water and therefore the urine is dilute. But in presence of ADH, these parts become quite permeable to water, so that much of the water present in tubular fluid is reabsorbed and the urine becomes concentrated. Besides ADH, the hormone aldosterone, secreted by adrenal glands, also plays important role in osmoregulatory function of kidneys by increasing Na+, K+ and Cl– reabsorption from the filterate.
Dilution Mechanism (Cortical nephrons) The osmolality of body fluids normally remains about 300 mL osmol per litre of water. When amount of water increases, this osmolality decreases. This switches off the secretion of a ADH from pituitary gland, but stimulates secretion of aldosterone from adrenal glands. Absence of ADH makes the walls of distal convoluted tubules and collecting ducts almost completely impermeable to water. Contrarily, due to secretion of the aldosterone the walls of ascending limb of Henle's loop, distal convoluted tubule and collecting duct become quite permeable to sodium, potassium and chloride ions. As a result of this Na+ and Cl– ions are reabsorbed from the filtrate flowing up the ascending limb of Henle's loop and mostly water and waste products remain in the filtrate. By the time this filtrate reaches into the distal tubule, it becomes very hypo-osmotic with only about 100 mL osmol/litre osmolality. Then, as this diluted fluid passes through the distal tubule and collecting duct, some more of the remaining ions, especially of sodium (Na+) are reabsorbed actively so that the osmolality of ultimate dilute urine is decreased to as low as about 65 to 70 mL osmol/litre. Dilution of urine mainly occurs in cortical nephrons.
Diuresis and Hypertension : Normally, we excrete about 1.5 litres of urine per day. Diluted urine is excreted in larger volumes a condition called diuresis. When due to the inefficient regulation, the kidneys fail to adequately dilute the urine, the body fluids are diluted and their increased volume causes hypertension (BP).
Glucose, urea, mannitol and other diuretic substances are administered to such patients. The kidneys excrete these substances and water is automatically excreted out with these. Caffeine of tea is also diuretic. That is why, urination becomes more frequent when more tea is taken. Contrarily, If secretion of ADH is permanently hampered or blocked in a patient, the urine becomes very dilute and tasteless (insipid). This condition is called diabetes insipidus. Intermittent urination at short intervals and thirst are the only discomforts in this condition.
Concentration mechanism (Juxtamedullary nephrons) During times of low water intake or excessive water loss, for example, due to heavy perspiration, diarrhoea, vomiting, etc the kidneys must conserve water while still eliminating wastes and excess ions. The kidneys accomplish this by producing concentrated urine. It is primarily the long-looped juxtamedullary nephrons which establish the conditions for producing Concentrated urine which may be four to five times more concentrated (1200 to 1400 mL osmol/litre) than plasma. concentrating the urine is under regulation of ADH and depends on presence of a steep gradient of increasing hyperosmolarity in the interstitial fluids of medullary pyramids.
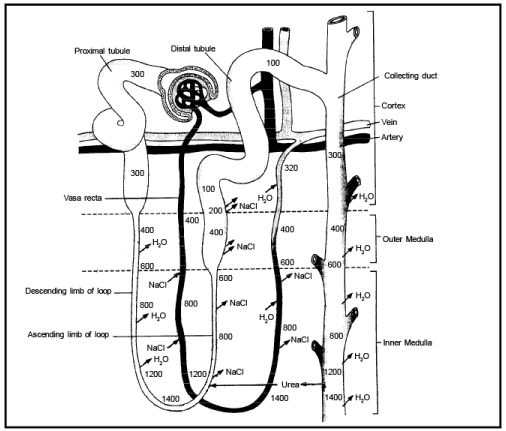
Medullary Heperosmolality :The osmolality of renal cortical interstitium is the same (300 mL osmol/litre) as in other tissues, but that of the interstitium of renal medulla is hypertonic with a gradient of hyperosmolality from renal cortex to the tips of medullary papillae. Under the conditions in which a concentrated urine is to be produced the hyperosmolality of medullary interstitium near the tips of the papillae is as high as 1200 to 1400 mL osmol/litre.
|
221 videos|172 docs|126 tests
|
FAQs on Mechanism: Urine Formation - Biology for JAMB
| 1. How is urine formed in the body? |  |
| 2. What are the main components of urine? | |
| 3. How does the body regulate urine formation? | |
| 4. What factors can affect urine formation? | |
| 5. Are there any medical conditions that can affect urine formation? | |




Viva Questions
,study material
,mock tests for examination
,MCQs
,Sample Paper
,Free
,Mechanism: Urine Formation | Biology for JAMB
,practice quizzes
,video lectures
,ppt
,Important questions
,past year papers
,Mechanism: Urine Formation | Biology for JAMB
,Previous Year Questions with Solutions
,Mechanism: Urine Formation | Biology for JAMB
,Exam
,Summary
,Objective type Questions
,Semester Notes
,Extra Questions
,shortcuts and tricks
;


Mechanism: Urine Formation Free PDF Download
Importance of Mechanism: Urine Formation
Mechanism: Urine Formation Notes
Mechanism: Urine Formation JAMB Questions
Study Mechanism: Urine Formation on the App
|
© EduRev
|
Education Revolution
|



|






within 7 days!