NCERT Summary: Human Capital & Human Development- 1 | Indian Economy for UPSC CSE PDF Download

The two terms sound similar but there is a clear distinction between them. Human development is based on the idea that education and health are integral to human wellbeing because only when people have the ability to read and write and the ability to lead a long and healthy life, they will be able to make other choices which they value. Human capital treats human beings as a means to an gad end being the increase in productivity. In this view, any investment in education and health is unproductive if it does not enhance output of goods and services. In the human development perspective human beings are ends themselves. Human welfare should be increased through investments in education and health even if such investments do not result in higher labour productivity. Therefore, basic education and basic health are important in themselves, irrespective of their contri-bution to labour productivity. In such a view, every individual has a right to get basic education and basic health care, that is, every individual has a right to be literate and lead a healthy life.
HUMAN CAPITAL FORMATION IN INDIA: GREAT PROSPECTS
In this section we are going to analyse human capital formation in India. We have already learnt that human capital formation is the outcome of investments in education, health, on-the-job training, migration and information of these education and health are very important sources of human capital formation. We know that ours is a federal country with a union government, state governments and local governments (Municipal Corporations, Municipalities and Village Panchayats). The Constitution of India mentions the functions to be carried out by each level of government. Accordingly, expenditures on both education and health are to be carried out simultaneously by all the three tiers of the government.
Do you know who takes car& of education and health in India? Before we take up the analysis of the education sector in India, we will look into the need for government intervention in education and health sectors. We do understand that education and health care services create both private and social benefits and this reason for the existence of both private and public institutions in the education and health service markets. Expenditures on education and health make substantial long-term impact and they cannot be easily reversed; hence, government intervention ' essential. For instance, once a child is admitted to a school or health care centre where the required services are not provided, before the decision is taken to shift the child to another institution, substantial amount of damage would have been done.
Moreover, individual consumers of these services do not have complete information about the quality of services and their costs. In this situation, the providers of education and health services acquire monopoly power and are involved in exploitation. The role of government in this situation is to ensure that the private provides of these services adhere to the standards stipulated by the government and charge the correct price.
In India, the ministries of education at the union and state level, departments of education and various organisations like National Council of Educational Research and Training (NCERT), University Grants Commission (UGC) and All India Council of Technical Education (AICTE) regulate the education sector. Similarly, the ministries of health at the union and state level, departments of health and various organisations like Indian Council for Medical Research (ICMR) regulate the health sector. In a developing country like ours, with a large section of the population living below the poverty line, many of us cannot afford to access basic education and health care facilities. Moreover, a substantial section of our people cannot afford to reach super specialty health care and higher education. Furthermore, when basic education and health care is considered as a right of the citizens, then it is essential that the government should provide education and health services free of cost for the deserving citizens and those from the socially oppressed classes. Both, the union and state governments, have been stepping up expenditures in the education sector over the years in order to fulfil the objective of attaining cent per cent literacy and considerably increase the average educational attainment of Indians.
EDUCATION SECTOR IN INDIA
Growth in Government Expenditure on Education: This expenditure by the government is expressed in two ways (i) as a percentage of 'total government expenditure' (ii) as a percentage of Gross Domestic Product (GDP). The percentage of 'education expenditure of total government expenditure' indicates the importance of education in the scheme of things before the government. The percentage of 'education expenditure of GDP' expresses how much of our income is being committed to the development of education in the country. During 1952-2002, education expenditure as percentage of total government expenditure increased from 7.92 to 13.17 and as percentage of GDP increased from 0.64 to 4.02. Throughout this period the increase in education expenditure has not been uniform and there has been irregular rise and fall. To this if we include the private expenditure incurred by individuals and by philanthropic institutions, the total education expenditure should be much higher.
Elementary education takes a major share of total education expenditure and the share of the higher / tertiary education (institutions of higher learning like colleges, polytechnics and universities) is the least. Though, on an average, the government spends less on tertiary education, 'expenditure per student' in tertiary education is higher than that of elementary. This does not mean that financial resources should be transferred from tertiary education to elementary education. As we expand school education, we need more teachers who are trained in the higher educational institutions; therefore, expenditure on all levels of education should be increased.
The per capita education expenditure differs considerably across states from as high as Rs. 34440 in Lakshadweep to as low as Rs. 386 in Bihar. This leads to differences in educational opportunities and attainments across states. One can understand the inadequcy of the expenditure on education if we compare it with the desired level of education expenditure as recommended by the various commissions. More than 40 years ago, the Education Commission (1964-66) had recommended that at least 6 percent of GDP be spent on education so as to make a noticeable rate of growth in educational achievements.
In December 2002, the Government of India, through the 86th Amendment of the Constitution of India, made free and compulsory education a fundamental right of all children in the age group of 6-14 years. The Tapas Majumdar Committee, appointed by the Government of India in 1998, estimated an expenditure of around Rs. 1.37 lakh crore over 10 years (1998-99 to 2006-07) to bring all India children in the age group of 6-14 years under the purview of school education. Compare to this desired level of education expenditure of around 6 per cent of GDP, the current level of a little over 4 per cent has been quite inadequate. In principle, a goal of 6 per cent needs to be reached—this has been accepted as a must for the coming years. In the Union Budget 2000-05, the Government of India levied a 2 per cent 'education cess' on all union taxes. The government estimated to get a revenue of rs. 4,000-5,000 crore and the entire amount was earmarked for spending on elementary education. In addition to this, the government sanctioned a large outlay for the promotion of higher education and new loan schemes for students to pursue higher education.
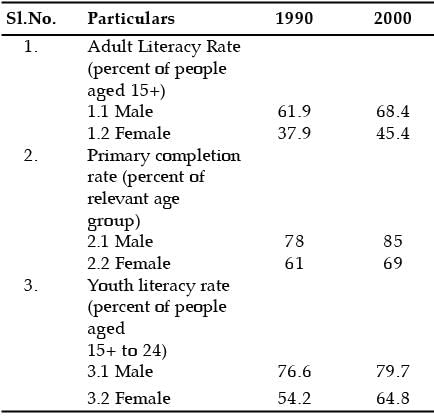
Education Achievements in India: Generally, educational achievements in a country are indicated in terms of adult literacy level, primary education completion rate and youth literacy rate. These statistics for the years 1990 and 2000 are given.
Education Achievements in India
|
108 videos|431 docs|128 tests
|
FAQs on NCERT Summary: Human Capital & Human Development- 1 - Indian Economy for UPSC CSE
| 1. What is human capital and why is it important? |  |
| 2. How does human development differ from human capital? | |
| 3. What are some examples of human capital? | |
| 4. How does investment in human capital contribute to economic growth? | |
| 5. What are the challenges in measuring and improving human capital? | |



NCERT Summary: Human Capital & Human Development- 1 | Indian Economy for UPSC CSE
,Exam
,Previous Year Questions with Solutions
,Objective type Questions
,mock tests for examination
,practice quizzes
,past year papers
,study material
,shortcuts and tricks
,ppt
,Extra Questions
,MCQs
,Important questions
,Sample Paper
,Semester Notes
,Summary
,Free
,NCERT Summary: Human Capital & Human Development- 1 | Indian Economy for UPSC CSE
,Viva Questions
,NCERT Summary: Human Capital & Human Development- 1 | Indian Economy for UPSC CSE
,video lectures
;






NCERT Summary: Human Capital & Human Development- 1 Free PDF Download
Importance of NCERT Summary: Human Capital & Human Development- 1
NCERT Summary: Human Capital & Human Development- 1 Notes
NCERT Summary: Human Capital & Human Development- 1 UPSC Questions
Study NCERT Summary: Human Capital & Human Development- 1 on the App
|
© EduRev
|
Education Revolution
|



|





