
Best Study Material for UPSC Exam
UPSC Exam > UPSC Notes > Medical Science Optional Notes for UPSC > Vitiligo
Vitiligo | Medical Science Optional Notes for UPSC PDF Download
| Table of contents |
|
| Hypo pigmented patches-Differential diagnosis |
|
| Vitiligo-Etiology |
|
| Vitiligo-Etiology (Theories) |
|
| Clinical Classification |
|
| Vitiligo-Diagnosis |
|
| Vitiligo-Repeats |
|
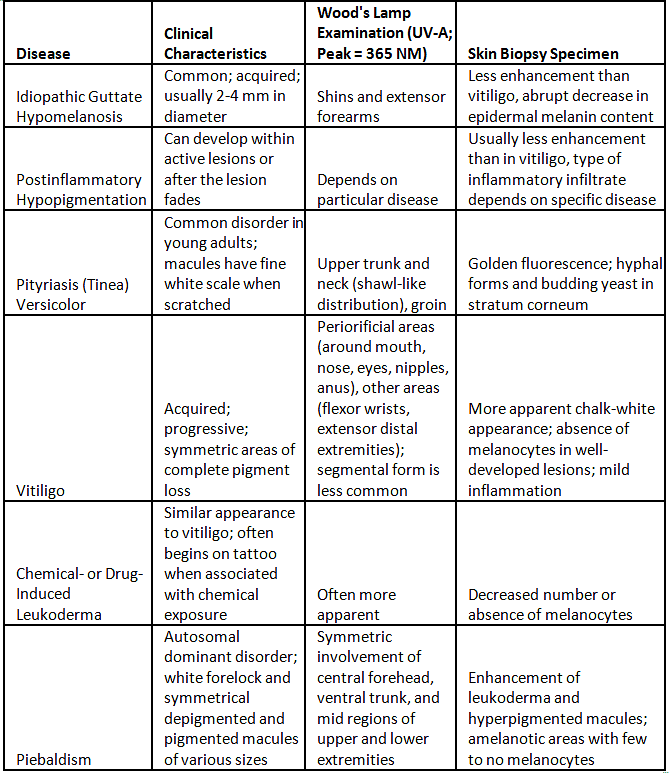
Hypo pigmented patches-Differential diagnosis
I. Primary Cutaneous Disorders
A. Diffuse
- Generalized vitiligo
B. Localized
- Idiopathic guttate hypomelanosis
- Postinflammatory
- Tinea (pityriasis) versicolor
- Vitiligo
- Chemical- or drug-induced leukoderma
- Nevus depigmentosus
- Piebaldism
II. Systemic Diseases
A. Diffuse
- Oculocutaneous albinism
- Hermansky-Pudlak syndrome
- Chediak-Higashi syndrome
- Phenylketonuria
B. Localized
- Systemic sclerosis (scleroderma)
- Melanoma-associated leukoderma
- Vogt-Koyanagi-Harada syndrome
- Onchocerciasis
- Sarcoidosis
- Cutaneous T cell lymphoma (especially mycosis fungoides)
- Tuberculoid and indeterminate leprosy
- Linear nevoid hypopigmentation (hypomelanosis of Ito)
- Incontinentia pigmenti (stage IV)
- Tuberous sclerosis
- Waardenburg syndrome
Question for Vitiligo
Try yourself:
What is the suggested etiology of vitiligo?View Solution
Vitiligo-Etiology
- Uncertain Etiology: The precise cause of Vitiligo remains unidentified.
- Multifactorial Nature: Vitiligo is suggested to be a multifactorial condition, involving a combination of genetic susceptibility and environmental factors.
- Genetic and Environmental Factors: Both genetic predisposition and environmental influences are believed to contribute to the development of Vitiligo.
- Risk Factors:
- Family History: Individuals with a family history of Vitiligo are at an increased risk.
- Autoimmune Diseases: Risk is associated with other autoimmune disorders like Hashimoto's thyroiditis, scleroderma, rheumatoid arthritis, type 1 diabetes mellitus, psoriasis, Addison's disease, pernicious anemia, alopecia areata, systemic lupus erythematosus, hypothyroidism, and celiac disease.
Vitiligo-Etiology (Theories)
- Unknown Cause: Despite various proposed theories, the exact cause of vitiligo remains unknown.
- Agreed Principles:
- Functional loss of melanocytes.
- Histochemically recognized melanocytes may be absent.
- Destruction, likely gradual, leading to a decrease in melanocytes.
- Theories on Destruction:
- Autoimmune Mechanism: Supported by evidence of circulating antibodies against melanocyte proteins in vitiligo patients. This theory suggests alterations in humoral and cellular immunity leading to melanocyte destruction, especially in nonsegmental vitiligo associated with autoimmune conditions.
- Cytotoxic Mechanism: Involves melanocyte dysfunction or destruction due to immune surveillance.
- Intrinsic Melanocyte Defects: Proposes inherent abnormalities in melanocytes hindering their growth and differentiation in conditions supportive of normal melanocytes.
- Oxidant-Antioxidant Mechanisms: Suggests that a metabolic product of melanin synthesis may cause melanocyte destruction.
- Neural Hypothesis: Involves a neurochemical mediator that destroys melanocytes or inhibits melanin production.
- Association with Autoimmune Conditions: Vitiligo, especially nonsegmental vitiligo, is often linked to autoimmune disorders such as Hashimoto thyroiditis, Graves disease, Addison disease, diabetes mellitus, alopecia areata, pernicious anemia, inflammatory bowel disease, psoriasis, and autoimmune polyglandular syndrome.
- Composite Hypothesis: Since none of the individual theories is entirely satisfactory, some suggest a composite hypothesis that combines elements from different theories.
Vitiligo-Presentation
- Distinctive Features:
- Lesions exhibit depigmented papules.
- Margins are sharply outlined and may merge to create geographical patterns.
- Hair in affected areas can lose pigmentation (known as leukotrichia).
- Distribution of lesions is widespread, with a higher susceptibility in trauma-prone regions.
- Lesion Characteristics:
- Lesions can manifest anywhere on the body.
- The progression of the condition is typically slow, although in some cases, it may advance rapidly.
- The presence of Koebner phenomenon is noted, indicating the development of lesions at sites of skin trauma.
Question for Vitiligo
Try yourself:
What are the various etiological factors for the causation of Vitiligo?View Solution
Clinical Classification
Vitiligo is categorized into two main groups: segmental and non-segmental. The differentiation between these two groups holds significant clinical relevance, influencing considerations related to progression, prognosis, and therapeutic approaches.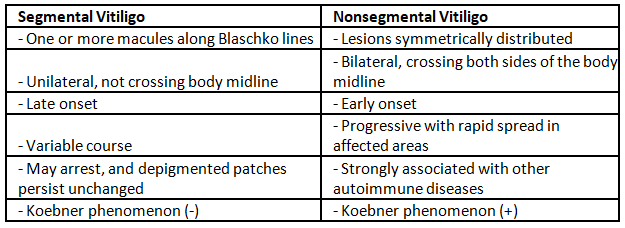
 |
Download the notes
Vitiligo
|
Download as PDF |
Download as PDF
Vitiligo-Diagnosis
Diagnosis of Vitiligo
- Lesions become more apparent and look chalky white under a Wood's lamp.
- Microscopic examination shows a complete loss of epidermal pigmentation, indicating a cell-mediated process destroying melanocytes in the epidermis.
- Immunohistochemistry testing may be performed to assess melanocytes, and laboratory work may include a thyroid panel, antinuclear antibody, and antithyroid peroxidase antibody.
- Assessment of extent and severity of vitiligo involves a numerical score system based on the rule of nines, evaluating five sites affected (head, upper limbs, trunk, lower limbs, and genitalia) using five stages of disease intensity.
- The VETI score is calculated based on the percentage of involvement and the grade of intensity for each site, providing a constant and reproducible measure. The maximum VETI score is 55.5.
 |
Take a Practice Test
Test yourself on topics from UPSC exam
|
Practice Now |
Practice Now
Treatment of Vitiligo
- Localized Disease
- New Lesions: Topical steroids, topical calcineurin inhibitors
- Old Lesions: Topical PUV A/P U V A plus UVA
- Extensive Disease
- New Lesions (Rapid Increase): Oral steroids, PUVA, narrow band UVB
- Old Lesions: Oral steroids, PUVA, narrow band UVB
- Intolerance to PUVA: Oral steroids
- Sunscreen, topical tacrolimus, and camouflage makeup are recommended for cosmetic reasons.
- New Therapies
- Afamelanotide: A long-lasting synthetic analog of alpha-melanocyte-stimulating hormone, which stimulates melanocyte proliferation and melanogenesis.
- Depigmentation: In carefully selected patients, a 20% cream of monobenzyl ether of hydroquinone is applied twice daily for 3-12 months.
- Refractory Patients
- Surgical Techniques: Punch grafting, split skin grafting, blister grafting, and melanocyte transfer can be considered for refractory but stable patients.
Question for Vitiligo
Try yourself:
Which of the following is a risk factor associated with vitiligo?View Solution
Vitiligo-Repeats
Q1: Mention various causes of hypo pigmented lesions of skin. Give a brief account of any two of such lesions. (2002)
Q2: Discuss Etiopathogenesis of Vitiligo. (2009)
Q3: What are various etiological factors for causation of Vitiligo? Enumerate various disorders associated with Vitiligo. (2013)
Q4: A 25-year-old unmarried female presents with asymptomatic depigmented macules of varying sizes over the breast, back, arms and legs for the last two years (2015)
i. List the different diagnosis.
ii. How would you investigate this patient?
iii. How would you treat the most common condition manifesting with the given symptomatology?
Q5: Describe various theories which have been proposed to explain the pathogenesis of vitiligo. How do you assess the severity of vitiligo? Describe the lines of treatment of various grades of the disease. (2018)
The document Vitiligo | Medical Science Optional Notes for UPSC is a part of the UPSC Course Medical Science Optional Notes for UPSC.
All you need of UPSC at this link: UPSC
|
7 videos|219 docs
|


FAQs on Vitiligo - Medical Science Optional Notes for UPSC
| 1. What are the possible causes of hypo-pigmented patches on the skin? |  |
| 2. What is the most common cause of hypo-pigmented patches known as vitiligo? | |
Ans. Vitiligo is a common cause of hypo-pigmented patches on the skin. It is an autoimmune condition where the immune system mistakenly attacks melanocytes, the cells responsible for producing skin pigment.
| 3. What are the theories regarding the etiology of vitiligo? | |
Ans. The etiology of vitiligo is not fully understood, but there are several theories. These include autoimmune theory, neural theory, oxidative stress theory, and genetic factors.
| 4. How is vitiligo clinically classified? | |
Ans. Vitiligo is clinically classified into different types based on the distribution and extent of hypo-pigmented patches. These include focal, segmental, generalized, and universal vitiligo.
| 5. How is vitiligo diagnosed? | |
Ans. Vitiligo is diagnosed through a combination of medical history, physical examination, and sometimes, additional tests such as Wood's lamp examination or skin biopsy. The presence of typical hypo-pigmented patches on the skin and the absence of other underlying conditions help in the diagnosis of vitiligo.
Related Exams
About this Document

4.88/5
Rating

Apr 01, 2025
Last updated
Document Description: Vitiligo for UPSC 2025 is part of Medical Science Optional Notes for UPSC preparation.
The notes and questions for Vitiligo have been prepared according to the UPSC exam syllabus. Information about Vitiligo covers topics
like Hypo pigmented patches-Differential diagnosis, Vitiligo-Etiology, Vitiligo-Etiology (Theories), Clinical Classification, Vitiligo-Diagnosis, Vitiligo-Repeats and Vitiligo Example, for UPSC 2025 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for Vitiligo.
Introduction of Vitiligo in English is available as part of our Medical Science Optional Notes for UPSC
for UPSC & Vitiligo in Hindi for Medical Science Optional Notes for UPSC course.
Download more important topics related with notes, lectures and mock test series for UPSC
Exam by signing up for free. UPSC: Vitiligo | Medical Science Optional Notes for UPSC
Description
Full syllabus notes, lecture & questions for Vitiligo | Medical Science Optional Notes for UPSC - UPSC | Plus excerises question with solution to help you revise complete syllabus for Medical Science Optional Notes for UPSC | Best notes, free PDF download
Information about Vitiligo
In this doc you can find the meaning of Vitiligo defined & explained in the simplest way possible. Besides explaining types of
Vitiligo theory, EduRev gives you an ample number of questions to practice Vitiligo tests, examples and also practice UPSC
tests

Related Searches
Free
,mock tests for examination
,Viva Questions
,Summary
,Exam
,Semester Notes
,MCQs
,video lectures
,Extra Questions
,Sample Paper
,Objective type Questions
,practice quizzes
,shortcuts and tricks
,Important questions
,study material
,past year papers
,Vitiligo | Medical Science Optional Notes for UPSC
,Vitiligo | Medical Science Optional Notes for UPSC
,Previous Year Questions with Solutions
,Vitiligo | Medical Science Optional Notes for UPSC
,ppt
;


Additional Information about Vitiligo for UPSC Preparation
Vitiligo Free PDF Download
The Vitiligo is an invaluable resource that delves deep into the core of the UPSC exam.
These study notes are curated by experts and cover all the essential topics and concepts, making your preparation more efficient and effective.
With the help of these notes, you can grasp complex subjects quickly, revise important points easily,
and reinforce your understanding of key concepts. The study notes are presented in a concise and easy-to-understand manner,
allowing you to optimize your learning process. Whether you're looking for best-recommended books, sample papers, study material,
or toppers' notes, this PDF has got you covered. Download the Vitiligo now and kickstart your journey towards success in the UPSC exam.
Importance of Vitiligo
The importance of Vitiligo cannot be overstated, especially for UPSC aspirants.
This document holds the key to success in the UPSC exam.
It offers a detailed understanding of the concept, providing invaluable insights into the topic.
By knowing the concepts well in advance, students can plan their preparation effectively.
Utilize this indispensable guide for a well-rounded preparation and achieve your desired results.
Vitiligo Notes
Vitiligo Notes offer in-depth insights into the specific topic to help you master it with ease.
This comprehensive document covers all aspects related to Vitiligo.
It includes detailed information about the exam syllabus, recommended books, and study materials for a well-rounded preparation.
Practice papers and question papers enable you to assess your progress effectively.
Additionally, the paper analysis provides valuable tips for tackling the exam strategically.
Access to Toppers' notes gives you an edge in understanding complex concepts.
Whether you're a beginner or aiming for advanced proficiency, Vitiligo Notes on EduRev are your ultimate resource for success.
Vitiligo UPSC Questions
The "Vitiligo UPSC Questions" guide is a valuable resource for all aspiring students preparing for the
UPSC exam. It focuses on providing a wide range of practice questions to help students gauge
their understanding of the exam topics. These questions cover the entire syllabus, ensuring comprehensive preparation.
The guide includes previous years' question papers for students to familiarize themselves with the exam's format and difficulty level.
Additionally, it offers subject-specific question banks, allowing students to focus on weak areas and improve their performance.
Study Vitiligo on the App
Students of UPSC can study Vitiligo alongwith tests & analysis from the EduRev app,
which will help them while preparing for their exam. Apart from the Vitiligo,
students can also utilize the EduRev App for other study materials such as previous year question papers, syllabus, important questions, etc.
The EduRev App will make your learning easier as you can access it from anywhere you want.
The content of Vitiligo is prepared as per the latest UPSC syllabus.
|
© EduRev
|
Education Revolution
|



|







Signup on EduRev and stay on top of your study goals
10M+ students crushing their study goals daily