Abnormal Labour


Transverse lie
- A lie characterized by the long axis of the fetus positioned at a right angle to that of the uterus.
- True instances of a complete transverse lie are uncommon, as the natural tendency is for the heavier cephalic pole to move towards one of the iliac fossae, while the breech moves in the opposite direction, typically resulting in an oblique lie.
- Oblique lie is a temporary condition, as the onset of labor typically leads to either a longitudinal or transverse lie.
- In cases of transverse lie, the Acromion process serves as the reference point, indicating a shoulder presentation.
- The incidence of transverse lie at term is approximately 0.3%.
Causes of transverse lie
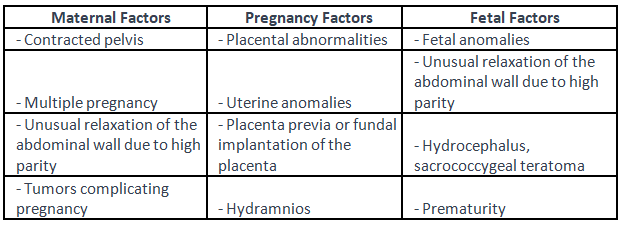
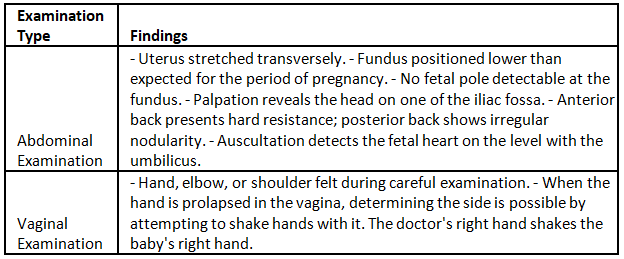
Diagnosis
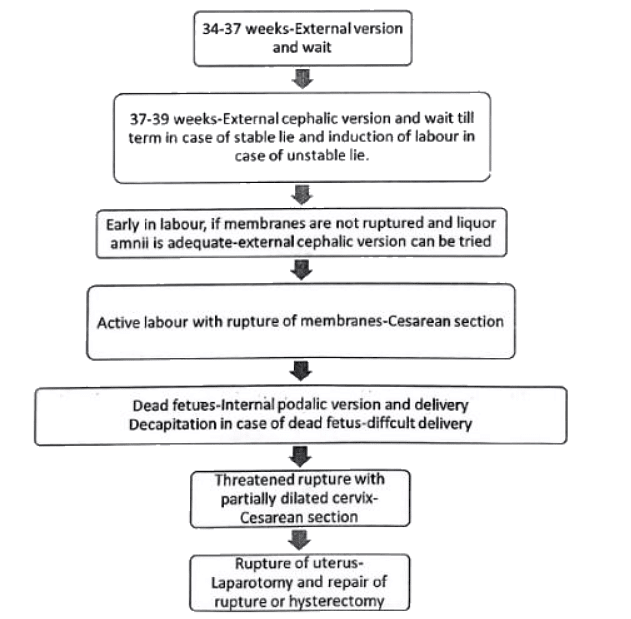
Transverse lie-Management
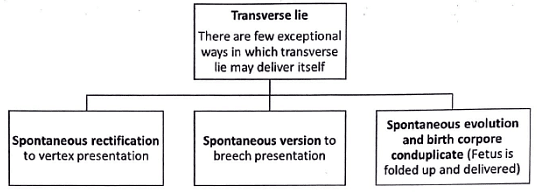
No question of spontaneous labour
Breech Presentation
Breech presentation is often associated with certain features, including:
- Fetal malformations
- Conditions such as hydrocephalus, anencephaly, and trisomy
- Uterine anomalies like septate or bicornuate uterus
- Placental factors like cornual implantation
- Prematurity, which is the most common cause
- Twins
- Oligohydramnios
- Short cord
- Intrauterine fetal demise
- Presence of placenta previa
- Maternal factors such as contracted pelvis
- Hydramnios
- Multiparity
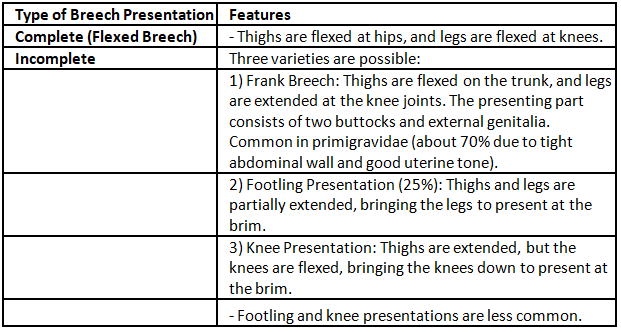
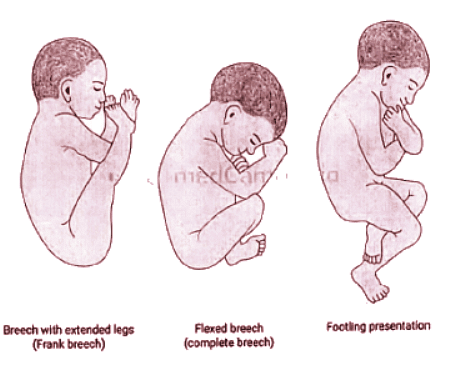
Breech presentation-varieties
There are two varieties of breech presentation
- Complete
- Incomplete
Maternal/Fetal Morbidity and Mortality associated with Breech presentation
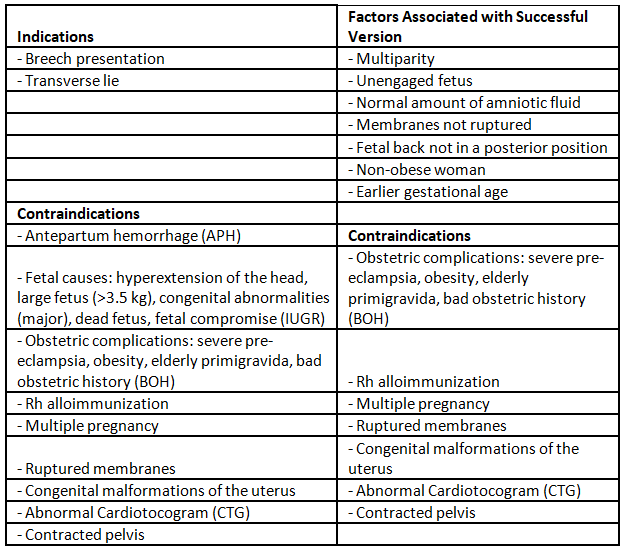
External cephalic version
- Breech presentation, although prevalent, becomes less common as gestational age advances, dropping from 20% at 28 weeks to 5% at 34 weeks and reaching 3-4% at term.
- External cephalic version is usually performed prior to labor in women who have reached 36 weeks of gestation with a breech fetus, aiming to minimize the risk of complications. If performed too early, there's a chance of spontaneous correction.
- Immediate delivery due to version usually does not result in severe complications associated with iatrogenic preterm delivery.
- External cephalic version is a series of maneuvers performed on the maternal abdomen to change the fetal presentation from breech to cephalic, effectively lowering the risks linked to both vaginal breech delivery and cesarean section.
- External cephalic version is contraindicated once labor commences, the fetus is engaged, there's insufficient amniotic fluid, or when fetal heart tracings show nonreassuring patterns.
- Potential risks of external cephalic version encompass placental abruption and cord prolapse, both of which may demand urgent intervention with a cesarean section.
- Providing 250 pg of terbutaline subcutaneously before attempting version is advantageous. If maternal tachycardia, a known terbutaline side effect, arises, the version attempt begins.
- For fetuses with persistent breech presentation, cesarean delivery is the preferred method.
Does external cephalic version reduce the incidence of breech and caesarean delivery and perinatal mortality?
- Patient counseling involves discussing success rates, the possibility of reverting to breech presentation, and the potential risks associated with the procedure itself.
- The procedure's risks encompass placental abruption, uterine rupture, fetomaternal hemorrhage, alloimmunization, preterm labor, fetal compromise, and, in rare cases, death.
- Although some complications can be serious, fetal deaths are infrequent, and the rates of urgent cesarean section are typically 0.5 percent or lower, based on various studies.
- Notably, post-successful version, the cesarean delivery rate may not completely revert to the baseline for vertex presentations. This is despite successful version, as indicated by multiple reports.
- Despite successful version, reports indicate that factors like dystocia, malpresentation, and nonreassuring fetal heart patterns may be more prevalent in these fetuses.
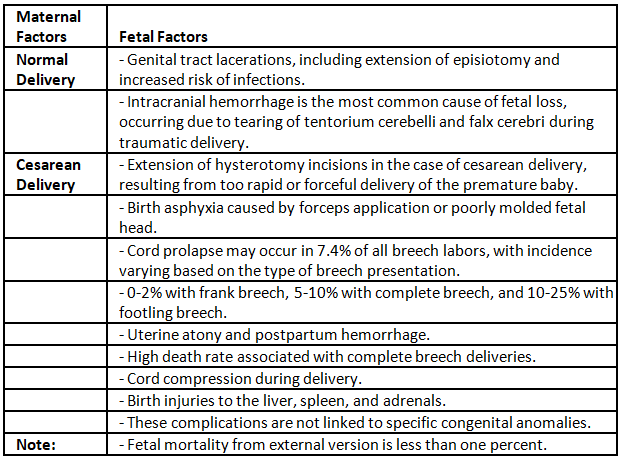
The main causes of perinatal mortality in breech presentation are:
- Fetal loss commonly results from intracranial hemorrhage, attributed to the tearing of the tentorium cerebella and falx cerebri. This occurrence is linked to traumatic delivery, specifically with the aftercoming head or too swift delivery of the soft head in premature infants.
- Birth asphyxia represents another potential complication.
- Cord prolapse can manifest in 7.4% of all breech labors, with the incidence varying based on the type of breech presentation. It is relatively rare in frank breech (0-2%), more common in complete breech (5-10%), and even more prevalent in footling breech (10-25%).
- Cord compression is a possible complication.
- Additionally, there is a risk of birth injuries affecting organs such as the liver, spleen, and adrenals.
Following criteria ideally be fulfilled for conduction of vaginal breech delivery:
- The fetal head is in a flexed position.
- The pelvis is sufficient for the delivery.
- The fetal weight falls within the average range of 1.5 to 3.5 kg.
- There are no accompanying medical or obstetric complications.
- Emergency cesarean section capabilities are available if needed.
- The fetus is not in a compromised state.
- Continuous labor monitoring facilities are in place.
Factors Favoring Cesarean Delivery of the Breech Fetus
- Inadequate operator experience.
- Patient expresses a preference for a cesarean delivery.
- The fetus is larger, exceeding 3800 to 4000 grams.
- A seemingly healthy and viable preterm fetus, either in active labor or requiring indicated delivery.
- Severe fetal growth restriction is present.
- The fetal anomaly is incompatible with vaginal delivery.
- History of previous perinatal death or neonatal birth trauma.
- Incomplete or footling breech presentation.
- Hyperextended fetal head.
- Clinically determined pelvic contraction or unfavorable pelvic shape, possibly assessed through pelvimetry.
- History of a prior cesarean delivery.
Breech presentation-Maneuvers
- Method Head Burns Marshall: A method involving the rotation of the fetal head to align it with the maternal pelvis for delivery.
- Mauriceau-Smellie-Veit method: A technique for delivering the head of a baby during difficult births, usually when the mother is unable to push effectively.
- Piper's forceps: A type of forceps used in childbirth to assist in the delivery of the baby's head when complications arise.
- Extended legs: Sometimes used to help facilitate certain positions for the mother during delivery, providing more space for the baby's descent.
- Pinard's maneuver: This maneuver involves specific hand movements to help reposition the baby inside the womb or assist in the delivery process.
- Extended arm: An adjustment made during delivery to assist with the positioning of the baby for a smoother birth.
- Lovset's maneuver: This technique involves manipulating the position of the baby's head or body to aid in delivery, especially in cases where there might be complications.
- Chin to pubis: Refers to the positioning of the baby's chin towards the mother's pubic bone during birth.
- Prague maneuver: A technique used to manage shoulder dystocia during childbirth, helping to release the baby's shoulder if it becomes stuck behind the mother's pubic bone.

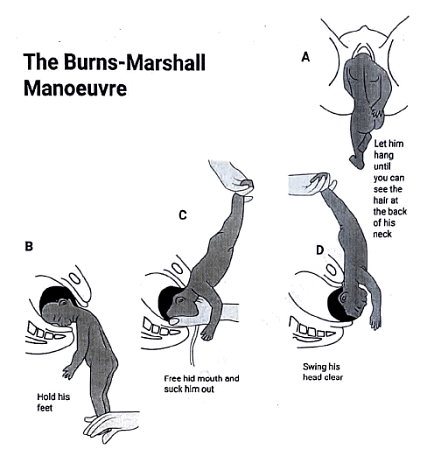
Bums Marshall method
When the occiput is seen under the pubic symphysis steady traction is given on the feet and baby is swung as an arc towards mothers abdomen by simultaneous suprapubic pressure head is born in flexion.
Mariceau-smellie-viet maneuvre
- When the baby's back is facing anteriorly, the Mauriceau-Smellie-Veit maneuver, involving jaw flexion and shoulder traction, can be employed for extraction, delivering the fetus in a head-down position.
- During this maneuver, the baby is placed on the left supinated forearm of the obstetrician, with limbs hanging on either side. The obstetrician's left index and middle fingers are positioned on the malar bones, while the right index and ring fingers rest on the respective shoulders, and the middle finger is placed on the sub-occipital region.
- To induce flexion, traction is applied in a downward and backward direction, while simultaneous suprapubic pressure is maintained by the assistant until the nape of the neck becomes visible.
- Following this, the baby is pulled in an upward and forward direction, allowing the face to be born. Simultaneously, by depressing the trunk, the head is delivered.

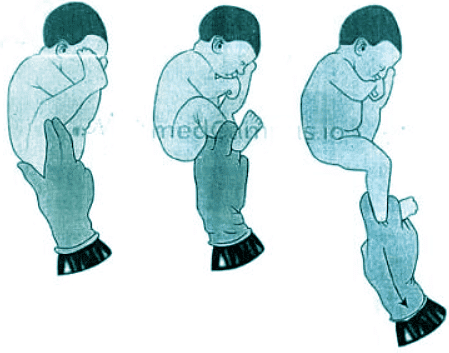
Pinards Maneuvre
- Position the palmar surface of the obstetrician's hand to face the ventral surface of the fetus.
- Apply pressure in the popliteal fossa using the middle and index fingers, and perform abduction of the fossa to induce partial flexion of the leg.
- Grasp the ankle using the internal fingers to bring down the foot.
- Repeat the same process for the other leg, bringing it down in a similar manner.
Lovset's maneuver
- Lovset's maneuver is a commonly employed technique for bringing down an extended arm during breech delivery, effectively correcting any upward displacement of the arms.
- The procedure involves rotating the baby's trunk downward while applying traction, holding the baby at the iliac crest. This maneuver positions the posterior shoulder below the symphysis pubis, facilitating the delivery of the arm. The delivery process includes flexing the shoulder, followed by hooking at the elbow, and then flexing the forearm down in a manner resembling a handshake.
- The same sequence is repeated with a reverse rotation of 180 degrees, ensuring that the anterior shoulder comes below the symphysis pubis.

Prague maneuver
- In cases of breech presentation where the back remains posterior, the modified Prague maneuver is employed to rotate the back to the anterior position.
- During this maneuver, two fingers of one hand are used to grasp the shoulders, while the other hand is utilized to draw the feet up over the maternal abdomen.

Abnormal Labour-Repeats
Q1: What is abnormal lie? Enumerate the various causes of transverse lie in a multiparous woman: How will you manage the case of transverse lie at term with a live foetus? (2014)
Q2: What are the common causes of Breech Presentation? Write down the contraindications to external cephalic version. (1996)
Q3: Answer the following question in less than 150 words. (2018) (2+2+2+4)
(i) What are the maternal risks in breech presentations?
(ii) Does external cephalic version reduce the incidence of breech and caesarean delivery and perinatal mortality?
(iii) Why is external cephalic version recommended at 37 weeks of gestation and not before?
(iv) What is Lovset's Manoeuvre?
FAQs on Abnormal Labour
| 1. What is a transverse lie and how does it affect labor? |  |
| 2. What is breech presentation and how is it managed? | |
| 3. What is an external cephalic version and when is it performed? | |
| 4. What are the maneuvers used to assist in delivering a baby in breech presentation? | |
| 5. What are the signs of abnormal labor and when should medical assistance be sought? | |



