
Best Study Material for UPSC Exam
UPSC Exam > UPSC Notes > Medical Science Optional Notes for UPSC > First trimester bleeding
First trimester bleeding | Medical Science Optional Notes for UPSC PDF Download
Abdominal pain during pregnancy-DIFFERENTIAL DIAGNOSIS
Every woman with an early pregnancy, vaginal bleeding, and pain should be evaluated. The primary goal is prompt diagnosis of an ectopic pregnancy. Serial quantitative serum β-hCG and progesterone levels and transvaginal sonography are used to ascertain if there is an intrauterine live fetus. Because these are not 100-percent accurate to confirm early fetal death or location, repeat evaluations are often necessary.
The differential diagnosis for abdominal pain coexistent with pregnancy is extensive.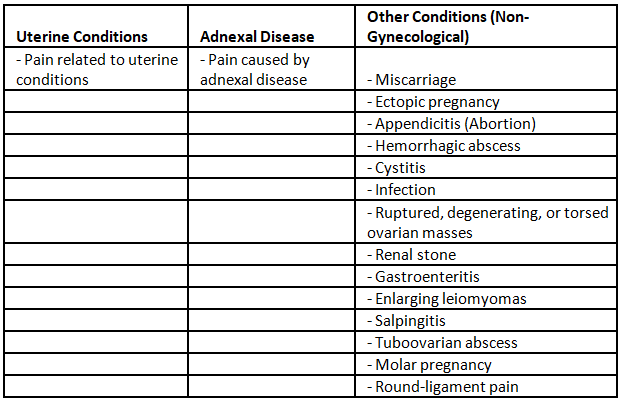
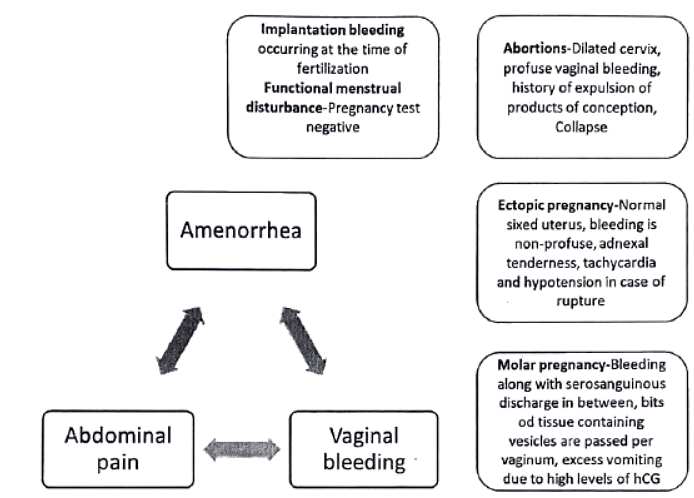
Abortion, Ectopic pregnancy and Molar pregnancy are associated with vaginal bleeding.
Differential diagnosis
First trimester bleeding
Pre-existing or Exacerbated During Pregnancy:
- Cervico-vaginitis
- Vascular erosion
- Cervical polyp
- Uterine fibroid
- Ruptured varicose veins
- Malignancy
- Trauma
- Drugs (Anticoagulants, Antiepileptics)
- Coagulopathy
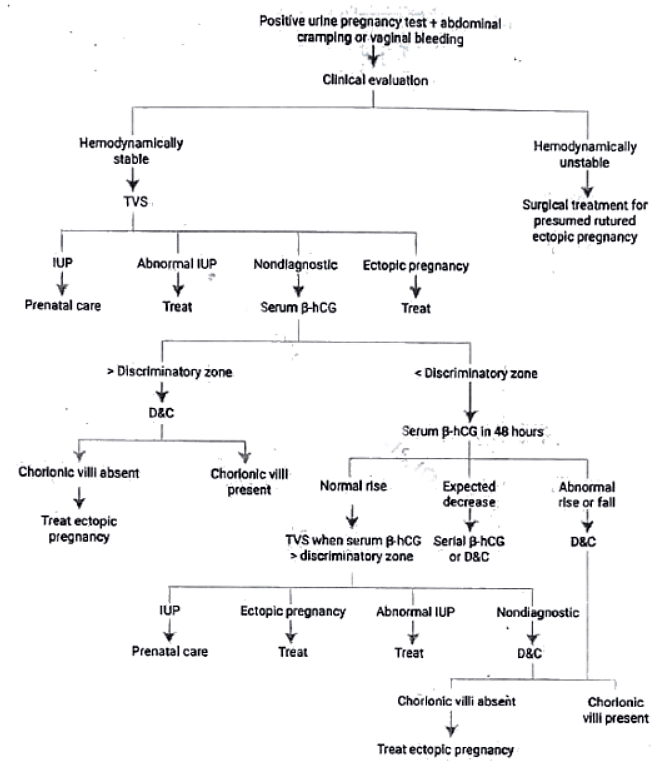
Management protocol
- Diagnostic Process for Bleeding or Pain with Positive Pregnancy Test:
- Initial Trans Vaginal Ultrasound (TVS) commonly performed to locate gestation.
- Identification of Yolk Sac, Embryo, or Fetus:
- If any of these are identified within the uterus or adnexa, a diagnosis can be established.
- Abnormal Intrauterine Pregnancy (IUP) - Hydatidiform Mole:
- In the case of abnormal IUP with a snowstorm appearance and absent fetal parts (hydatidiform mole), appropriate treatment is administered.
- Non-Diagnostic Scenario - Evaluate Serum Beta hCG:
- If there is an absence of fetal parts in both the uterus and adnexa, it is considered non-diagnostic.
- Serum Beta hCG evaluation is recommended in such cases.
- Discriminatory Zone for Serum Beta hCG:
- Investigators have defined a discriminatory zone, i.e., a serum 3-hCG concentration above which failure to visualize an intrauterine pregnancy indicates a nonviable or ectopic pregnancy.
- Barnhart et al. (1994) found that an empty uterus with a serum 3-hCG concentration > 1500 mlU/mL was 100 percent accurate in excluding a live uterine pregnancy.
Question for First trimester bleeding
Try yourself:
Which of the following is not a possible cause of abdominal pain during pregnancy?View Solution
Ectopic Pregnancy
Risk factors
- Congenital anomalies of fallopian tubes
- Prior tubal surgery
- Prior PID
- Use of IUCD
- Use of progestogen contraceptives
- Assisted reproductive technologies
- Previous tubal pregnancies
Options for ectopic tubal pregnancy treatment include medical (single dose or multi dose methotrexate therapy) and surgical (laparoscopic salpingostomy) approaches.
Medical vs Surgical approach
- Women treated with methotrexate had significantly better physical functioning immediately following therapy, but there were no differences in psychological functioning.
- Ectopic resolution success rates were not significantly different between those managed surgically and those treated with methotrexate.
Conclusion from various studies-Women who are hemodynamically stable and in whom there is a small tubal diameter, no fetal cardiac activity, and serum (S-hCG concentrations < 5000 mlU/mL have similar outcomes with medical or surgical management. Despite lower success rates with medical therapy for women with larger tubal size, higher serum (3-hCG levels, and fetal cardiac activity, medical management can be offered to the motivated woman who understands the risks.
Role of expectant management in Ectopic pregnancy
- Indication: Very early tubal pregnancies associated with stable or decreasing serum β-hCG levels.
- Statistics from the American College of Obstetricians and Gynecologists (2012): 88 percent of ectopic pregnancies resolve when β-hCG levels are below 200 mlU/mL.
- Expectant Management Comparative to Surgery and Medical Approaches: Subsequent rates of tubal patency and intrauterine pregnancy are similar with expectant management, surgery, and medical interventions.
- Considerations for Expectant Therapy: The potential serious consequences of tubal rupture, along with the known safety of medical and surgical treatments, emphasize that expectant therapy should be pursued only in appropriately selected and counseled women.
Medical treatment protocol for ectopic pregnancy
Methotrexate is highly effective against rapidly proliferating tissue such as trophoblast, and overall ectopic tubal pregnancy resolution rates approximate 90 percent with its use.
For ease and efficacy, intramuscular methotrexate administration is used most frequently for ectopic pregnancy resolution, and single-dose and multi dose methotrexate protocols are available.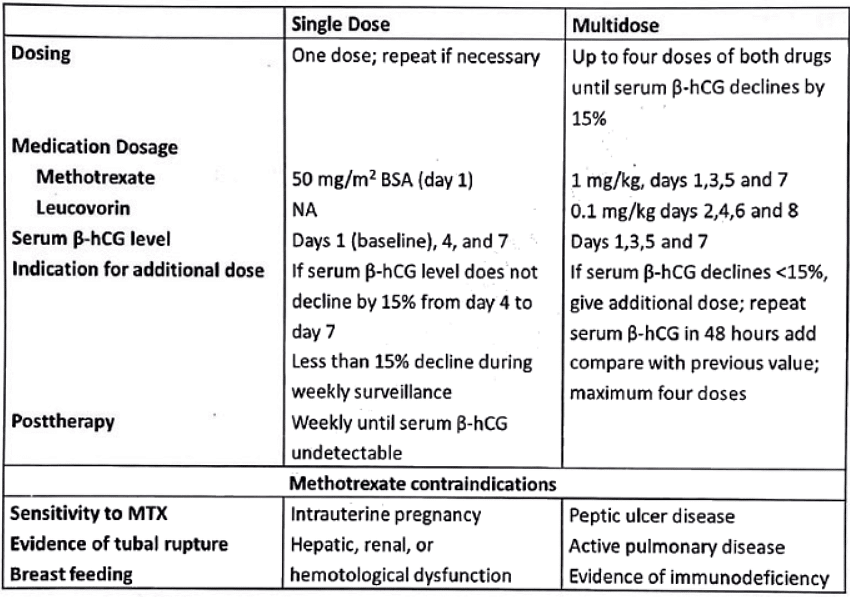 Single-dose therapy offers simplicity, less expense, and less intensive post therapy monitoring and does not require leucovorin rescue. Higher success rate for the multi-dose regimen is reported in most of the studies.
Single-dose therapy offers simplicity, less expense, and less intensive post therapy monitoring and does not require leucovorin rescue. Higher success rate for the multi-dose regimen is reported in most of the studies.
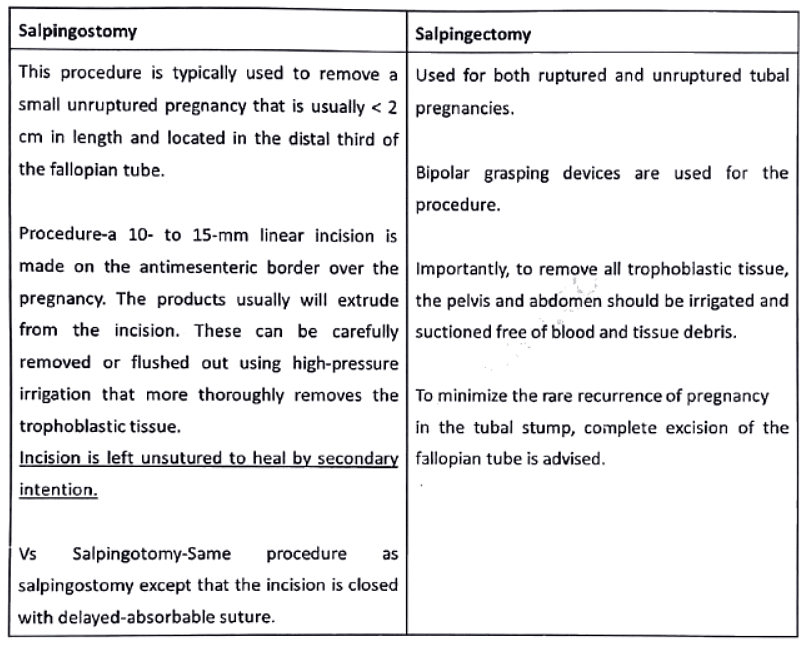
Surgical management for ectopic tubal pregnancy
 |
Download the notes
First trimester bleeding
|
Download as PDF |
Download as PDF
Hydatidiform mole or molar pregnancy-management
After the evacuation, the extended-term outlook for women with a hydatidiform mole does not show improvement with prophylactic chemotherapy. Consequently, the American College of Obstetricians and Gynecologists does not routinely recommend it.
Risk Factors for Trophoblastic Neoplasia Post-Molar Evacuation:
- Complete moles exhibit a 15 to 20 percent incidence of malignant consequences, whereas partial moles show a 1 to 5 percent incidence.
- Advanced age is a risk factor.
- Elevated β-hCG levels (> 100,000 mlU/mL) are associated with an increased risk.
- Larger-than-expected uterine size during gestation is a risk factor.
- The presence of theca-lutein cysts exceeding 6 cm is a risk factor.
- A slow decline in β-hCG levels is also considered a risk factor.
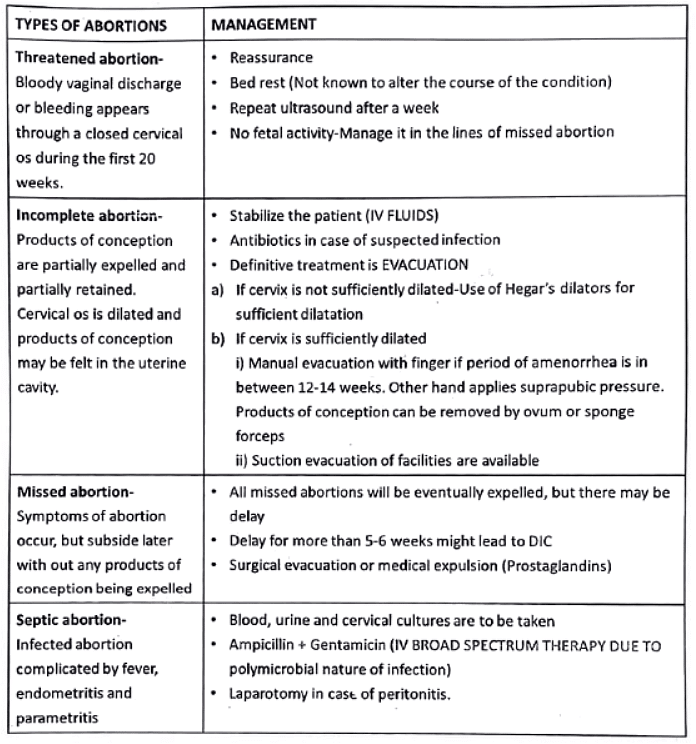
Types of abortions
MTP ACT 2020 (Amendment of MTP ACT 1971)-Bill passed in Lok sabha Mar 17, 2020
- Extension of Termination Limits: The upper limit for termination is extended to 20-24 weeks (previously 20 weeks) for cases involving rape, incest, and significant fetal anomalies.
- Determining Fetal Anomalies: A medical board comprising four members (pediatrician, radiologist, gynecologist, and a member specified by the state government) will decide on substantial fetal anomalies.
- Patient Privacy: Privacy of the patient must be maintained.
- Opinions for Termination: Up to 20 weeks, termination requires the opinion of one doctor, while 20-24 weeks necessitates opinions from two doctors.
- Partner Involvement: The term 'married woman or her husband' is replaced with 'woman or her partner' in cases of termination due to contraception failure.
- Termination Criteria by Central Government: Termination up to 24 weeks is restricted to specific categories of women as prescribed by the central government. Norms for the required medical practitioner's opinion will be notified by the central government.
- Unwanted Pregnancy Resulting from Contraception Failure: If pregnancy occurs due to contraceptive failure, it may be considered a serious threat to the mental health of the woman. The Bill replaces 'married woman or her husband' with 'woman or her partner' in this provision.
- Medical Board Constitution: The upper termination limit does not apply when necessary due to substantial fetal abnormalities diagnosed by a Medical Board. Each state government must establish a Medical Board with specified members, and the central government will outline their powers and functions.
- Protection of Privacy: Registered medical practitioners are prohibited from disclosing the identity of a woman whose pregnancy has been terminated, except to authorized individuals under the law. Violation of this provision is punishable by imprisonment or a fine.
 |
Take a Practice Test
Test yourself on topics from UPSC exam
|
Practice Now |
Practice Now
Methods of first-trimester MTP
- Menstrual Regulation through Aspiration:
- Aspiration of the uterine cavity using Karman's cannula is effective up to 42 days from the last menstrual period (LMP).
- Potential complications include failure to evacuate, incomplete evacuation, hemorrhage, cervical laceration, perforation, infection, and anesthetic issues.
- Dilatation and Suction Evacuation (Vacuum Evacuation):
- Most effective for terminating pregnancies within the first 12 weeks.
- Utilizes a standard negative suction of 650 mm Hg for aspiration.
- Caution is advised against check curettage with a sharp curette to avoid traumatic complications like perforation, synechiae (Asherman syndrome), and the risk of placenta accreta in future pregnancies.
- Priming with prostaglandin gel or suppository helps prevent complications such as cervical tear, lacerations, and internal os injuries leading to an incompetent cervix.
- Medical Methods:
- Permissible up to 9 weeks of gestation (63 days).
- Protocol:
- Day 1: Administer 200 mg of mifepristone as a single dose. Observe the woman for half an hour and then allow her to go home. Anti-D globulin is given to RH-negative women.
- Day 3: Administer 400 mcg of oral misoprostol (prostaglandin) unless abortion has occurred. Monitor pulse and blood pressure for 2 hours. If all is well, allow the woman to go home.
- Late Sequelae of Medical Termination:
- Pelvic inflammatory disease (PID) leading to chronic pelvic pain.
- Infertility due to tubal infection and blockage.
- Incompetent cervix resulting from trauma, leading to preterm births and habitual mid-trimester abortions.
- Adherent placenta in subsequent pregnancies.
- Asherman syndrome.
- Ectopic pregnancy following PID.
- Cervical ectopic pregnancy caused by trauma.
- Intrauterine growth restriction (IUGR).
- Additional Concerns:
- Rh-isoimmunization risk if anti-D has not been administered to non-immunized Rh-negative mothers after the termination.
- Potential psychiatric disorders, especially feelings of regret or distress, may arise if the termination was performed without proper counseling, particularly if infertility follows the procedure.
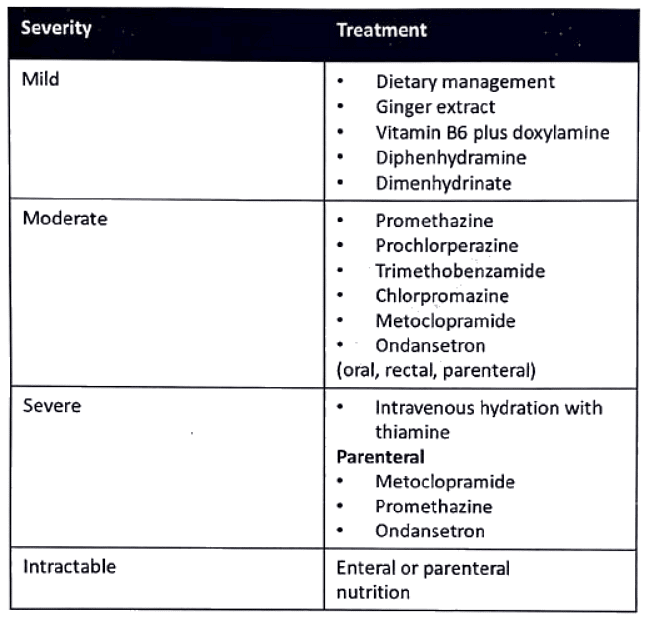
Hyperemesis gravidarum
- Hyperemesis gravidarum is intractable vomiting of pregnancy and is associated with disturbed nutrition.
- Early signs of the disorder include weight loss (up to 5% o f body weight) and ketonuria.
Question for First trimester bleeding
Try yourself:
Which of the following is a risk factor for ectopic pregnancy?View Solution
First trimester bleeding-Repeats
Q1: List the risk factors for ectopic pregnancy. How will you manage a 25-year old woman with ruptured tubal pregnancy (1996)?
Q2: How would you manage a case of bleeding per vaginum with pain abdomen at 8 weeks of gestation (2006)?
Q3: Discuss the differential diagnosis in a 28-year-old woman with two months amenorrhea and acute lower abdominal pain followed by bleeding per vaginum. How would you manage such patient? (2012)
Q4: A 25-year-old married lady presents with history of 10 weeks amenorrhoea, acute lower abdominal pain and fainting. On clinical examination, she has tachycardia, hypertension and pelvic tenderness (2015)
i. What is the most likely diagnosis?
ii. How would you investigate such a patient?
iii. How would you manage such a patient? List the key points.
The document First trimester bleeding | Medical Science Optional Notes for UPSC is a part of the UPSC Course Medical Science Optional Notes for UPSC.
All you need of UPSC at this link: UPSC
|
7 videos|219 docs
|



FAQs on First trimester bleeding - Medical Science Optional Notes for UPSC
| 1. What are the common causes of abdominal pain during pregnancy? |  |
| 2. What is an ectopic pregnancy and how is it managed? | |
Ans. An ectopic pregnancy occurs when the fertilized egg implants outside the uterus, usually in the fallopian tube. It is a medical emergency that requires immediate attention. In early cases, medical treatment with methotrexate may be used to stop the growth of the pregnancy and allow the body to absorb it. In more advanced cases or if there is a rupture, surgical management is necessary, which may involve removing the fallopian tube.
| 3. What is a molar pregnancy and how is it managed? | |
Ans. A molar pregnancy, also known as a hydatidiform mole, is a rare condition in which abnormal tissue grows in the uterus instead of a fetus. It is typically diagnosed through ultrasound and blood tests. The management involves removing the abnormal tissue through a dilation and curettage (D&C) procedure. Close monitoring and follow-up are necessary to ensure complete removal and to detect any signs of persistent or recurrent disease.
| 4. What are the different types of abortions? | |
Ans. The different types of abortions include spontaneous abortion (miscarriage), induced abortion (termination of pregnancy), and therapeutic abortion (performed to protect the mother's health or in cases of severe fetal abnormalities). Spontaneous abortions can occur naturally or may require medical or surgical intervention depending on the circumstances.
| 5. What is hyperemesis gravidarum and how is it managed? | |
Ans. Hyperemesis gravidarum is a severe form of morning sickness characterized by persistent nausea and vomiting during pregnancy. It can lead to dehydration and weight loss. Management typically involves lifestyle modifications, such as dietary changes and rest, along with antiemetic medications to control symptoms. In severe cases, hospitalization may be required for intravenous fluids and nutrition. Regular monitoring and follow-up with a healthcare provider are important.
Related Exams
About this Document

Mar 10, 2025
Last updated
Document Description: First trimester bleeding for UPSC 2025 is part of Medical Science Optional Notes for UPSC preparation.
The notes and questions for First trimester bleeding have been prepared according to the UPSC exam syllabus. Information about First trimester bleeding covers topics
like Abdominal pain during pregnancy-DIFFERENTIAL DIAGNOSIS, Management protocol, Ectopic Pregnancy, Medical treatment protocol for ectopic pregnancy, Surgical management for ectopic tubal pregnancy, Hydatidiform mole or molar pregnancy-management, Types of abortions, MTP ACT 2020 (Amendment of MTP ACT 1971)-Bill passed in Lok sabha Mar 17, 2020, Methods of first-trimester MTP, Hyperemesis gravidarum , First trimester bleeding-Repeats and First trimester bleeding Example, for UPSC 2025 Exam. Find important definitions, questions, notes, meanings, examples, exercises and tests below for First trimester bleeding.
Introduction of First trimester bleeding in English is available as part of our Medical Science Optional Notes for UPSC
for UPSC & First trimester bleeding in Hindi for Medical Science Optional Notes for UPSC course.
Download more important topics related with notes, lectures and mock test series for UPSC
Exam by signing up for free. UPSC: First trimester bleeding | Medical Science Optional Notes for UPSC
Description
Full syllabus notes, lecture & questions for First trimester bleeding | Medical Science Optional Notes for UPSC - UPSC | Plus excerises question with solution to help you revise complete syllabus for Medical Science Optional Notes for UPSC | Best notes, free PDF download
Information about First trimester bleeding
In this doc you can find the meaning of First trimester bleeding defined & explained in the simplest way possible. Besides explaining types of
First trimester bleeding theory, EduRev gives you an ample number of questions to practice First trimester bleeding tests, examples and also practice UPSC
tests

Related Searches
video lectures
,Free
,practice quizzes
,Important questions
,Summary
,First trimester bleeding | Medical Science Optional Notes for UPSC
,past year papers
,Exam
,Semester Notes
,Viva Questions
,Extra Questions
,study material
,First trimester bleeding | Medical Science Optional Notes for UPSC
,First trimester bleeding | Medical Science Optional Notes for UPSC
,shortcuts and tricks
,mock tests for examination
,Previous Year Questions with Solutions
,Objective type Questions
,ppt
,Sample Paper
,MCQs
;






Additional Information about First trimester bleeding for UPSC Preparation
First trimester bleeding Free PDF Download
The First trimester bleeding is an invaluable resource that delves deep into the core of the UPSC exam.
These study notes are curated by experts and cover all the essential topics and concepts, making your preparation more efficient and effective.
With the help of these notes, you can grasp complex subjects quickly, revise important points easily,
and reinforce your understanding of key concepts. The study notes are presented in a concise and easy-to-understand manner,
allowing you to optimize your learning process. Whether you're looking for best-recommended books, sample papers, study material,
or toppers' notes, this PDF has got you covered. Download the First trimester bleeding now and kickstart your journey towards success in the UPSC exam.
Importance of First trimester bleeding
The importance of First trimester bleeding cannot be overstated, especially for UPSC aspirants.
This document holds the key to success in the UPSC exam.
It offers a detailed understanding of the concept, providing invaluable insights into the topic.
By knowing the concepts well in advance, students can plan their preparation effectively.
Utilize this indispensable guide for a well-rounded preparation and achieve your desired results.
First trimester bleeding Notes
First trimester bleeding Notes offer in-depth insights into the specific topic to help you master it with ease.
This comprehensive document covers all aspects related to First trimester bleeding.
It includes detailed information about the exam syllabus, recommended books, and study materials for a well-rounded preparation.
Practice papers and question papers enable you to assess your progress effectively.
Additionally, the paper analysis provides valuable tips for tackling the exam strategically.
Access to Toppers' notes gives you an edge in understanding complex concepts.
Whether you're a beginner or aiming for advanced proficiency, First trimester bleeding Notes on EduRev are your ultimate resource for success.
First trimester bleeding UPSC Questions
The "First trimester bleeding UPSC Questions" guide is a valuable resource for all aspiring students preparing for the
UPSC exam. It focuses on providing a wide range of practice questions to help students gauge
their understanding of the exam topics. These questions cover the entire syllabus, ensuring comprehensive preparation.
The guide includes previous years' question papers for students to familiarize themselves with the exam's format and difficulty level.
Additionally, it offers subject-specific question banks, allowing students to focus on weak areas and improve their performance.
Study First trimester bleeding on the App
Students of UPSC can study First trimester bleeding alongwith tests & analysis from the EduRev app,
which will help them while preparing for their exam. Apart from the First trimester bleeding,
students can also utilize the EduRev App for other study materials such as previous year question papers, syllabus, important questions, etc.
The EduRev App will make your learning easier as you can access it from anywhere you want.
The content of First trimester bleeding is prepared as per the latest UPSC syllabus.
|
© EduRev
|
Education Revolution
|



|











Signup to see your scores
go up within 7 days!
Access 1000+ FREE Docs, Videos and Tests
Takes less than 10 seconds to signup